
Abstract
Background and Purpose
Long-term outcomes after pediatric neurocritical illness are poorly characterized. This study aims to characterize the frequency and risk factors for post-discharge unplanned health resource use in a pediatric neurocritical care population using insurance claims data.
Methods
Retrospective cohort study evaluating children who survived a hospitalization for an acute neurologic illness or injury requiring mechanical ventilation for >72 hours and had insurance eligibility in Colorado’s All Payers Claims database. Insurance claims identified unplanned readmissions and emergency department [ED] visits during the post-discharge year. For patients without pre-existing epilepsy/seizures, we evaluated for post-ICU epilepsy identified by claim(s) for a maintenance anti-seizure medication during months 6-12 post-discharge. Multivariable logistic regression identified factors associated with each outcome.
Results
101 children, median age 3.7 years (interquartile range (IQR) .4-11.9), admitted for trauma (57%), hypoxic-ischemic injury (17%) and seizures (15%). During the post-discharge year, 4 (4%) patients died, 26 (26%) were readmitted, and 48 (48%) had an ED visit. Having a pre-existing complex chronic condition was independently associated with readmission and emergency department visit. Admission for trauma was protective against readmission. Of those without pre-existing seizures (n = 86), 25 (29%) developed post-ICU epilepsy. Acute seizures during admission and prolonged ICU stays were independently associated with post-ICU epilepsy.
Conclusions
Survivors of pediatric neurocritical illness are at risk of unplanned healthcare use and post-ICU epilepsy. Critical illness risk factors including prolonged ICU stay and acute seizures may identify cohorts for targeted follow up or interventions to prevent unplanned healthcare use and post-ICU epilepsy.
Keywords
Introduction
Pediatric intensive care unit (PICU) mortality has decreased in recent decades, but PICU survivors are often discharged with new morbidities and experience increased rates of health resource use.1,2 Children with critical illness due to neurologic diagnoses such as traumatic brain injury (TBI) and stroke are at an increased risk of poor functional outcomes and new morbidities.3-10 While outcomes after TBI have been extensively studied, new morbidities, trajectory of recovery, and post-discharge health resource use in critically ill children with a primary neurologic condition are less well characterized.6,11,12 Specifically, epilepsy is a well-described sequela of TBI and has been associated with hospital readmissions in pediatric trauma.10,13,14 However, the development of epilepsy after severe neurologic injury and risk factors for persistent seizures are poorly characterized in a broad cohort of pediatric neurocritical care (PNCC) patients. 3 Post-discharge interventions such as post-ICU follow-up care targeting PNCC patients at high risk of post-discharge health resource use may optimize recovery and facilitate a safe return to the medical home.15,16
The objectives of this study were to characterize the frequency of unplanned health resource use (hospital readmission and ED visits) during the year after discharge and identify factors associated with unplanned health resource use within a cohort of critically ill children with a primary neurologic diagnosis. Additionally, we conducted exploratory analyses in a subset of the cohort without a prior diagnosis of epilepsy or seizures to evaluate the frequency of post-discharge epilepsy and risk factors associated with this outcome. We hypothesized that children who had seizures during their index hospitalization would have an increased risk of unplanned healthcare utilization including hospital readmission, ED visit and post-discharge epilepsy.
Methods
Subjects
This study was conducted at an urban, quaternary, free-standing children’s hospital with up to 40 PICU beds during winter months that serves as a referral center for a large metropolitan region and includes an inpatient pediatric rehabilitation program. We used our center’s Virtual Pediatric Systems database (VPS) to identify children admitted to the PICU on or after Jan 1, 2013 and discharged from the hospital before January 1, 2017, who survived an episode of
Patient and Hospitalization Characteristics
Patient and hospitalization characteristics were collected from the VPS database which relies on standardized methods to categorize patient conditions and diagnoses. 18 We collected patient (e.g., age, sex, race/ethnicity), admission (e.g., primary diagnosis, severity of illness scores including Pediatric Risk of Mortality [PRISM] III and Pediatric Index of Mortality [PIM] 2), and hospitalization (e.g., PICU and hospital lengths of stay, duration of mechanical ventilation) variables from our site’s VPS database.19,20 Comorbidities were identified by chart review (ABM) and patients were categorized based on the Pediatric Medical Complexity Algorithm (PMCA) as having a pre-existing complex chronic condition (CCC; e.g., trisomy 21, sickle-cell anemia, cerebral palsy), non-complex chronic condition (NCCC; e.g., spinal scoliosis, asthma, obstructive sleep apnea), or no pre-existing chronic conditions.21,22 We specifically collected pre-existing diagnoses of seizures or neurologic complex chronic conditions based on chart review. Primary diagnoses were categorized into five categories: trauma, hypoxic-ischemic injuries, seizures, central nervous system infections, and other diagnoses (Supplemental Table 1). Duration of mechanical ventilation was defined as the longest duration of continuous invasive mechanical ventilation. If a patient was extubated and reintubated in less than 48 hours, this was considered as a period of continuous mechanical ventilation. We categorized patients as having a complicated stay if they received cardiopulmonary resuscitation or had a tracheostomy placed in the PICU.
Health Care Utilization
Subjects were linked in the Colorado All Payers Claims Database (APCD) by medical record number and hospital discharge date. Insurance claims in the APCD include mandated reporting from Medicaid, Medicare Advantage and Medicare Fee-for-Service, commercial, and voluntary reporting from self-insured employer-based plans. 23 We collected insurance claims including hospital admissions, ED visits, and medication claims of all medication prescriptions filled during the year after hospital discharge. In patients with a readmission, we characterized the readmission as planned or unplanned based on chart review and only included unplanned readmissions in our analyses. For the readmissions, the primary diagnosis was determined by chart review (AM). We also collected pre-admission hospitalization and ED claims within the 13 months to 1 month prior to hospital admission. Post-discharge deaths were collected from the Colorado Department of Public Health and Environment database.
Identification of Post-ICU Epilepsy
In the subset of patients without a diagnosis of epilepsy or seizures prior to their index hospitalization, we evaluated for patients with a new diagnosis of epilepsy after discharge. Post-ICU epilepsy was defined by a medication claim (i.e., prescriptions filled) for a maintenance anti-seizure medication during months 6-12 after discharge, reflective of new or ongoing treatment of seizures. “Emergency” or “Rescue” medications (e.g., rectal diazepam and intranasal midazolam) were not considered maintenance anti-seizure medications.
Data Analysis
Patient and index hospitalization characteristics were summarized using count and proportion for categorical variables or median and interquartile range (IQR) for continuous variables. We compared patients who matched in the APCD (study cohort) to those who did not have insurance eligibility for inclusion in the APCD and were excluded from our study. The primary outcome was unplanned health resource use including hospital readmission or ED visit during the post-discharge year. For each outcome, we used elastic net regularized regression with 10-fold cross validation to select the set of variables that minimized cross validation error. Variables considered for inclusion in the multivariable model were patient (age, sex, race/ethnicity, PMCA category), admission (primary diagnosis category, pre-hospital cardiac arrest, PRISM III and PIM-2 severity of illness scores), and clinical course (seizures during the index hospitalization, complicated PICU stay, duration of mechanical ventilation, and PICU length of stay) characteristics. Using the set of variables selected by the elastic net procedure, we used logistic regression with the Firth adjustment to make inferences of the associations between the independent and outcome variables.24,25 In the sub-cohort without a pre-existing diagnosis of epilepsy or seizures, we used the same process to identify patient, admission, and clinical characteristics associated with post-ICU epilepsy. Significance of univariable associations between the categorical and continuous variables and outcomes were assessed using Fisher’s exact test and the Wilcoxon-Mann-Whitney test, respectively. Statistical analysis was performed using R version 4.0.2 (R Foundation (Vienna), 2020-06-22). The study received a waiver of consent and authorization from the Institutional Review Board (Protocol #18-0488).
Results
Cohort Characteristics.
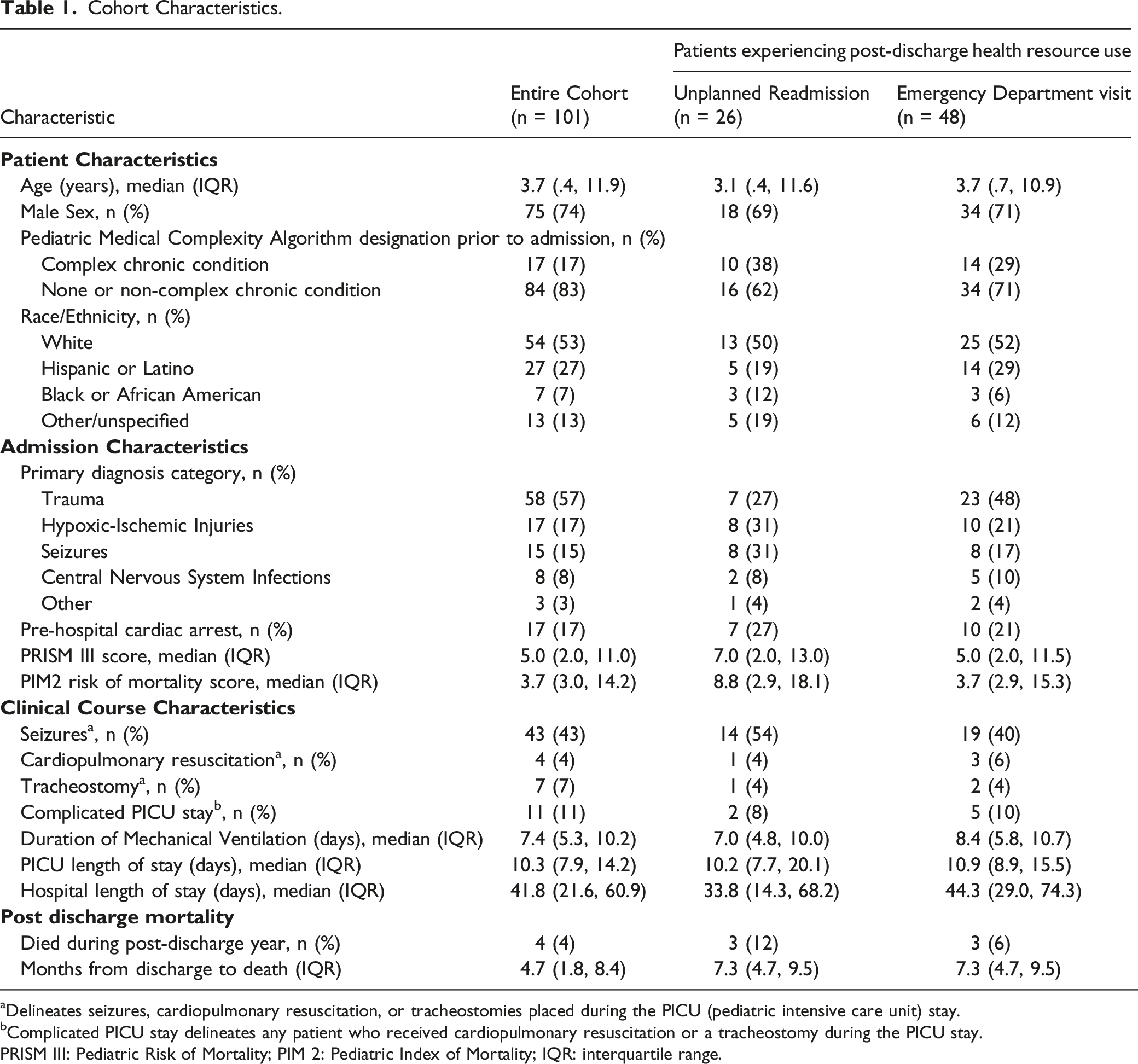
aDelineates seizures, cardiopulmonary resuscitation, or tracheostomies placed during the PICU (pediatric intensive care unit) stay.
bComplicated PICU stay delineates any patient who received cardiopulmonary resuscitation or a tracheostomy during the PICU stay.
PRISM III: Pediatric Risk of Mortality; PIM 2: Pediatric Index of Mortality; IQR: interquartile range.
Post-Discharge Outcomes
During the post-discharge year, 4 (4%) patients died a median 4.7 months (IQR 1.8-8.4) after discharge. Twenty-six (26%) patients experienced an unplanned hospital readmission a median of 2.7 months (IQR .5-4.6) after discharge. Of the readmitted patients, the most common reasons for readmission were neurologic conditions (n = 11, 42%) including 5 of whom were readmitted for seizures, and respiratory illness (n = 11, 42%). Forty-eight (48%) patients had at least one ED visit which occurred a median of 1.6 months (IQR .5-4.8) after discharge. Of the patients who had an ED visit, the median (IQR) number of visits during the post discharge year was 2 (2, 5). Of the 78 patients with pre-admission data, patients who had been admitted to the hospital during the year prior to the index hospitalization were more likely to have an unplanned readmission in the year following discharge (11/19 [58%] vs 12/59 [20%], P = .002).
Predictors of Post-discharge Health Resource Utilization
Characteristics Associated With Unplanned Health Care Encounters During The Post-Discharge Year in Univariable Analyses.
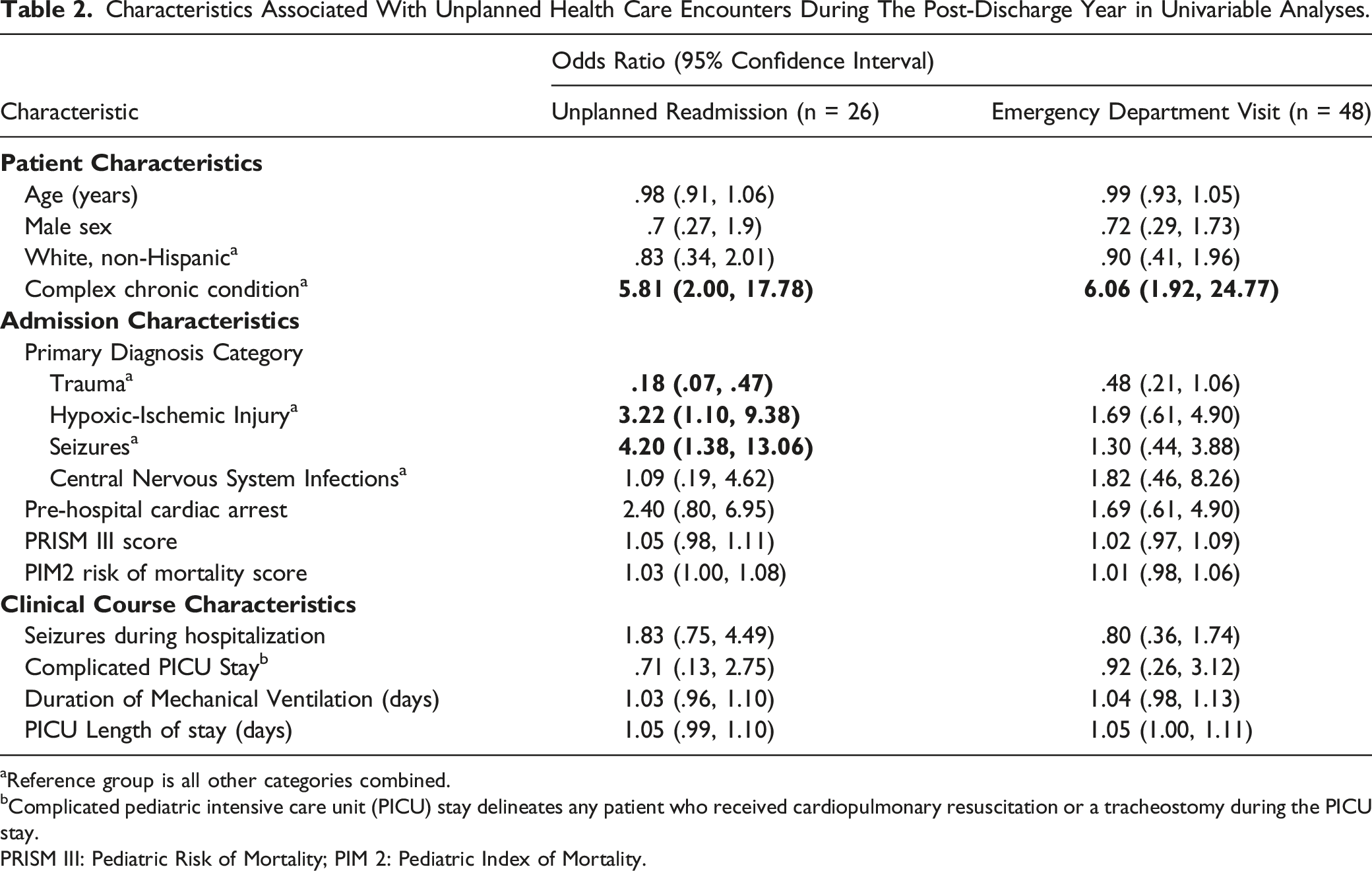
aReference group is all other categories combined.
bComplicated pediatric intensive care unit (PICU) stay delineates any patient who received cardiopulmonary resuscitation or a tracheostomy during the PICU stay.
PRISM III: Pediatric Risk of Mortality; PIM 2: Pediatric Index of Mortality.
Multivariable Model Evaluating Risk Factors Associated With Hospital Readmission and Emergency Department Visit During The Post-Discharge Year.
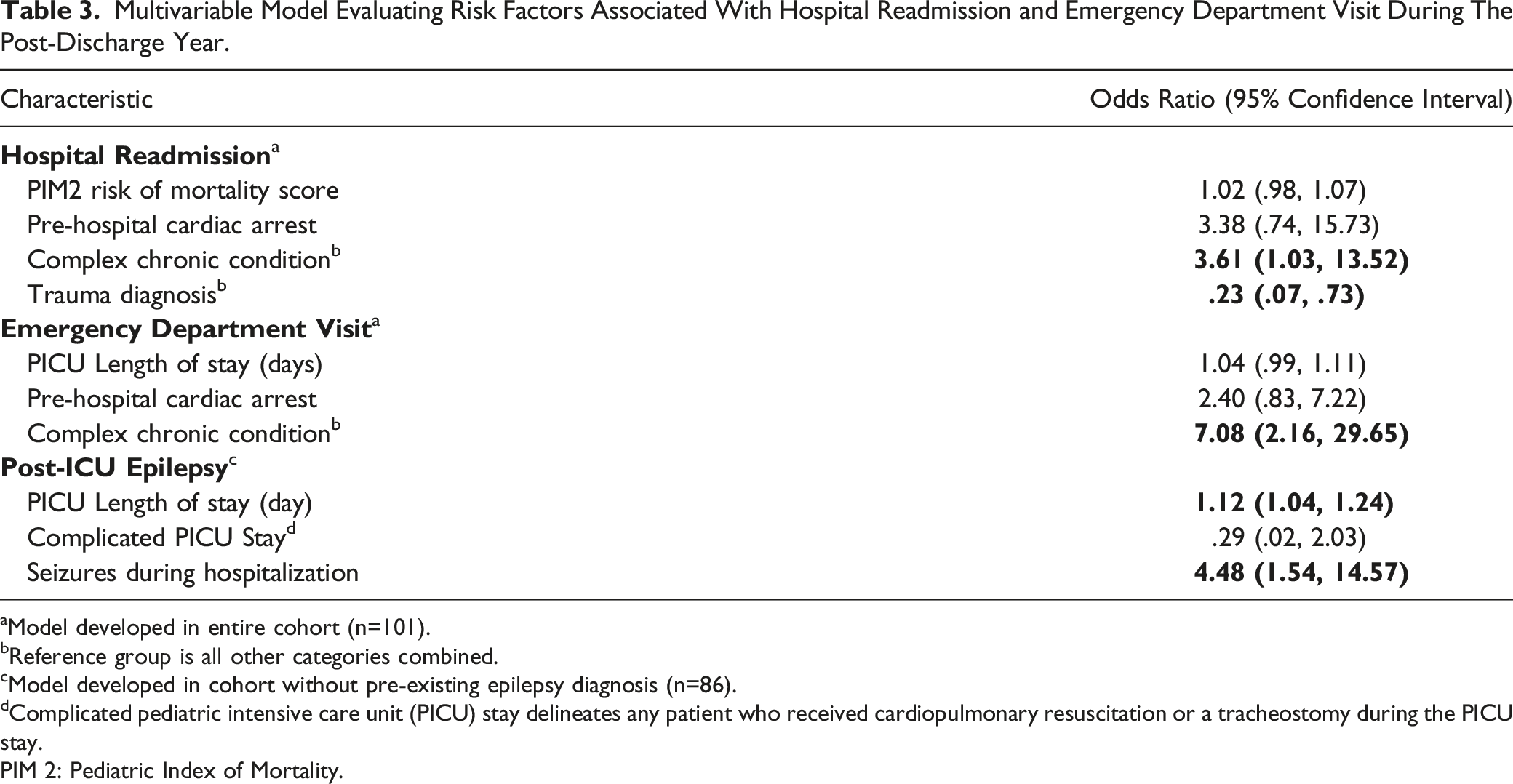
aModel developed in entire cohort (n=101).
bReference group is all other categories combined.
cModel developed in cohort without pre-existing epilepsy diagnosis (n=86).
dComplicated pediatric intensive care unit (PICU) stay delineates any patient who received cardiopulmonary resuscitation or a tracheostomy during the PICU stay.
PIM 2: Pediatric Index of Mortality.
In univariable analyses, experiencing an ED visit after discharge was associated with having a pre-existing CCC (Table 2). Pre-existing CCC, cardiac arrest prior to admission, and PICU length of stay were identified as key variables to include in multivariable analysis (Table 3). Pre-existing CCC was most strongly associated with having an ED visit after discharge (OR 7.08 [95% CI: 2.16, 29.65]). Of the 78 patients with pre-admission data, patients who had an ED visit during the year prior to the index hospitalization were more likely to have an ED visit in the year following discharge (16/21 [76%] vs 24/57 [42%], P = .01).
Post-ICU Epilepsy
Patient, Diagnosis, and Clinical Course Characteristics of Subset of Cohort Without Pre-Admission Diagnosis of Seizure or Epilepsy.
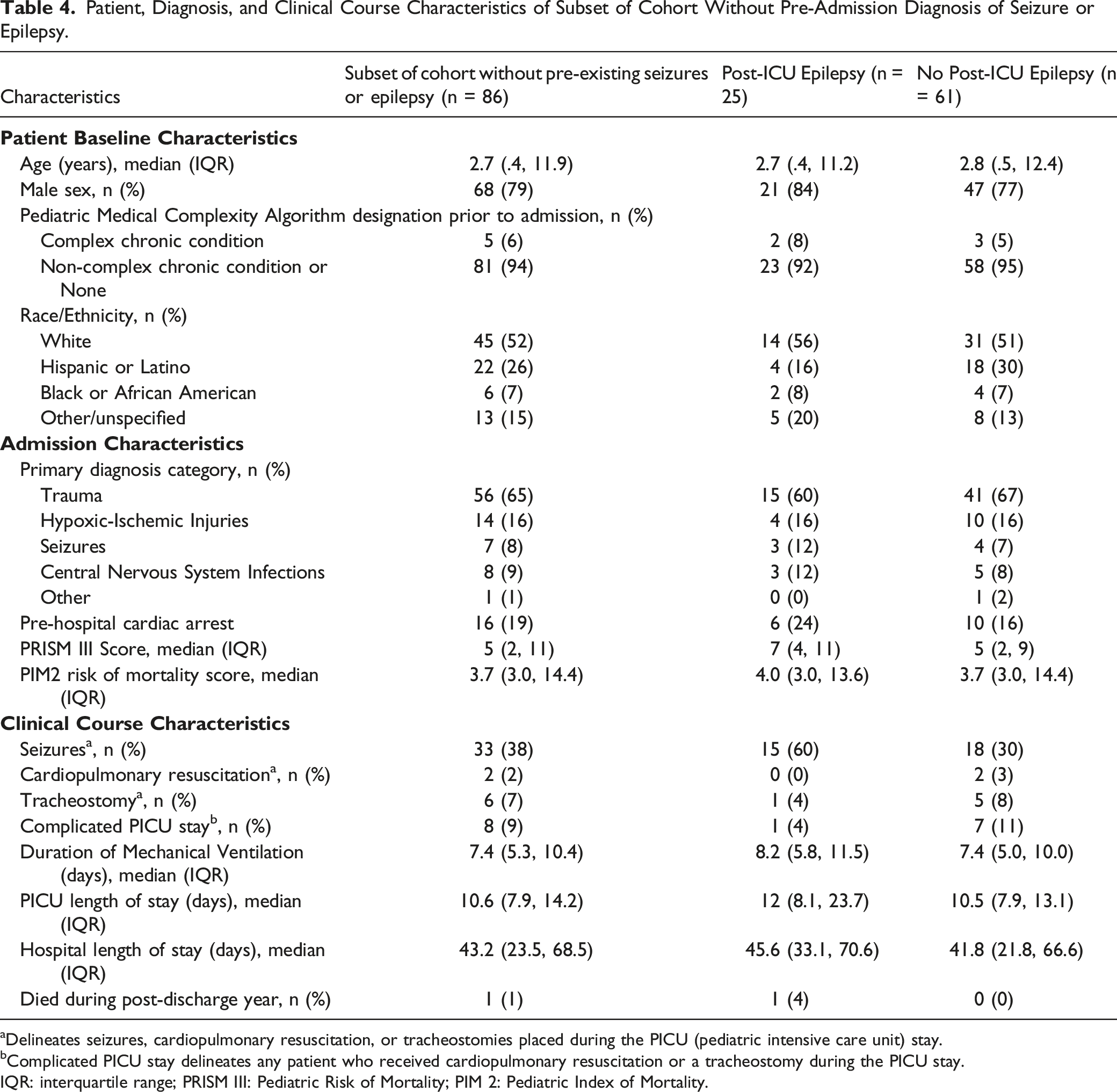
aDelineates seizures, cardiopulmonary resuscitation, or tracheostomies placed during the PICU (pediatric intensive care unit) stay.
bComplicated PICU stay delineates any patient who received cardiopulmonary resuscitation or a tracheostomy during the PICU stay.
IQR: interquartile range; PRISM III: Pediatric Risk of Mortality; PIM 2: Pediatric Index of Mortality.
In univariable analyses, seizures during the index hospitalization and longer PICU stay were associated with post-ICU epilepsy. In multivariable analysis, the strongest predictors of a patient developing post-ICU epilepsy was having seizures during the index hospitalization (OR 4.48 [95% CI: 1.54, 14.57]) and longer PICU lengths of stay (OR 1.12 [95% CI: 1.04, 1.24]).
Notably, there were 10 patients who did not have seizures during the index hospitalization but developed post-ICU epilepsy (Supplemental Table 4). These patients were predominantly older (median age 12.4 years [IQR 5.4-13.4]), did not have a pre-existing CCC, were admitted for trauma (n = 6) or hypoxic-ischemic injury (n = 3), and had high illness severity (median PIM2 risk of mortality 11.6% [IQR 3.4%-15.8%]). Hospitalization characteristics were notable for long durations of mechanical ventilation (median 8.7 days [IQR 6.7-11.4]) and prolonged PICU and hospital lengths of stay (18.3 days [IQR 11.2-23.8] and 92.2 [46.8-135.1]), respectively.
Discussion
In this retrospective cohort study of PNCC patients who required mechanical ventilation for at least 3 days, we found that one in four patients had an unplanned readmission during the year after discharge and half of the patients had a hospital readmission or ED visit, both occurring predominantly during the first 3 months after discharge. Readmissions and ED visits were strongly associated with having a pre-existing CCC. Also, independent of pre-hospital characteristics, we found that patients admitted with a primary diagnosis of trauma were less likely be readmitted. Additionally, amongst the patients without a history of seizures, nearly one in three developed post-ICU epilepsy and most patients with post-ICU epilepsy experienced unplanned health resource use during the post-discharge year.
The high rate of unplanned readmission (26%) and ED visits (48%) in this cohort identifies PNCC patients as a cohort at high risk of unplanned health resource use. In comparison, critically ill children with sepsis are recognized as a cohort at increased risk of readmission and experience rates of readmission of approximately 20%.26,27 Post-discharge follow-up care has been targeted at pediatric sepsis patients to ensure optimization of recovery to improve post-discharge outcomes. 28 For this post-sepsis cohort, a targeted approach was used to identify patients at risk of undiagnosed sequelae or inadequate follow-up. Pilot studies of post-neurocritical care clinics have been described recently, with providers identifying needs not recognized at hospital discharge.15,16 These models of care may be helpful in preventing post-discharge unplanned healthcare use. Additionally, families of patients in these clinics have reported high levels of satisfaction in part due to having well-informed expectations in the months after neurocritical care admissions; indeed, such family-centered practices have been identified as areas of focus for future research.29-31 Importantly, within our PNCC cohort, we found that TBI patients may be at lower risk of readmission compared to the other admission diagnoses. This finding is consistent with a recently published report demonstrating a lower readmission rate of 8.6% in a large cohort of children hospitalized for TBI. 10 The relatively lower rate of readmissions for patients hospitalized with TBI may be related to injury maturation resulting in a more favorable recovery trajectory relative to patients with more chronic neurologic conditions or differences in post-discharge support structures. Further elucidation of factors associated with unplanned health resource use could identify a cohort most likely to benefit from a targeted post-discharge intervention.
Children with medical complexity comprise less than 1% of the pediatric population, but account for a much larger share of health care utilization.32,33 Almost one-fifth of our PNCC cohort had a pre-existing CCC and, as we would have expected, these children represented a particularly vulnerable cohort with a 3.6-times greater likelihood of rehospitalization and 7-times greater likelihood of an ED visit within the post-discharge year. Similar discrepancies in health resource use have been described in 90-day readmission rates of children with sepsis with readmission rates of 7.2% in previously healthy children compared with 25.5% in children with chronic conditions. 27 Similarly, a recent study evaluating children with neurologic conditions identified that health resource use variables such as number of medications and prior health resource use were more strongly associated with hospital readmission compared to the patient’s specific neurologic condition. 34 The underlying risk factors associated with medically complex children are unlikely to be modifiable, yet research suggests that reduction of risk of hospital readmission is possible. A systematic review identified that programs focused on the hospital-to-home transition, including parental coaching and home visitation, were associated with decreased readmissions in medically complex children. 35 Though many patients in our PNCC cohort likely received specialized ongoing care after discharge, targeting the post-ICU period with innovative modalities of health care delivery may decrease unplanned health care use.
Post-ICU epilepsy was a common outcome amongst our cohort, occurring in nearly one-third of patients without epilepsy or seizures prior to admission. Seizures during the index hospitalization and longer PICU stays were independently associated with post-ICU epilepsy. In a study by Williams et al evaluating a cohort of 325 PNCC patients, these investigators also identified seizures during the index admission as a risk factor for worse outcomes across a cohort of children with varying neurologic diagnoses. 6 Acute seizures and PICU length of stay may represent non-modifiable markers of illness severity, or they may represent opportunities for interventional treatments. For example, improved seizure control during the index hospitalization may decrease the secondary injury inflicted by seizures and result in decreased rates of post-ICU epilepsy. Future studies should consider testing for modifiable risk factors associated with post-ICU epilepsy as it may be a targetable long-term outcome in interventional trials. Interestingly, while seizures during the index hospitalization were associated with development of post-ICU epilepsy, ten patients who did not have seizures while hospitalized developed post-ICU epilepsy. As suggested in a previous study of critically ill children with TBI, we hypothesize that seizures may be reflective of evolution of brain recovery. 3
This study has several limitations. The cohort is limited to children with critical illness who were mechanically ventilated for at least 72 hours and, therefore, is not representative of all PNCC patients. For example, some PNCC patients with specific underlying conditions (e.g., neuromuscular weakness) may have been more likely to be included as they may be at increased risk of prolonged intubation. Additionally, the single center study design represents the population at our quaternary care facility but generalizability to other sites requires additional investigation. Similarly, we limited our study to patients with insurance eligibility in the APCD and additional studies are needed to ensure generalizability across insurance status and types including the uninsured. Additionally, patients residing outside of Colorado may have underreported rates of readmission and ED visits. Notably, except for a higher proportion of male patients in the matched cohort, the patient and index hospitalization characteristics did not differ between the matched and unmatched cohorts. As a retrospective study, the analyzable variables were limited to those which were collected through VPS, and some important factors (e.g., imaging findings, medications, seizure duration) were not included. Additionally, we were unable to delineate whether a patient had a prior or subsequent ICU stay relative to the index hospitalization as our APCD data did not include level of care, thus limiting our ability to understand the relationship between multiple ICU exposures. Lastly, to identify post-ICU epilepsy, we used a surrogate of prescriptions filled for anti-seizure medications in lieu of a formal diagnosis. To decrease the possibility of including patients prescribed anti-seizure medications for only a brief period after their hospitalization, we limited the post-ICU epilepsy cohort to those who received anti-seizure medications beyond 6 months after discharge.
Conclusions
Pediatric neurocritical care patients are at high risk of unplanned health resource use after discharge. Targeted follow-up and anticipatory guidance for high-risk patients including those with a pre-existing CCC and non-trauma admission diagnoses, may prevent unplanned use of resources in the ED and avoid readmissions. Future interventional trials aimed at decreasing rates of post-ICU epilepsy will require targeting patients at highest risk of this outcome. Additional studies are needed to identify potentially modifiable factors related to this outcome.
Supplemental Material
Supplemental material - Unplanned Admissions, Emergency Department Visits, and Epilepsy After Critical Neurological Illness Requiring Prolonged Mechanical Ventilation in Children
Supplemental material for Unplanned Admissions, Emergency Department Visits, and Epilepsy After Critical Neurological Illness Requiring Prolonged Mechanical Ventilation in Children by Matthew B. Spear, Kristen Miller, Craig Press, Christopher Ruzas, Jaime LaVelle, Peter M. Mourani, Tellen D. Bennett, and Aline B. Maddux in The Neurohospitalist
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (K23HD096018) and the Francis Family Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. For the remaining authors, there are no relevant conflicts of interest.
Data Sharing Agreement
Deidentified data are available through collaboration with the study investigators through a data use agreement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.