
Abstract

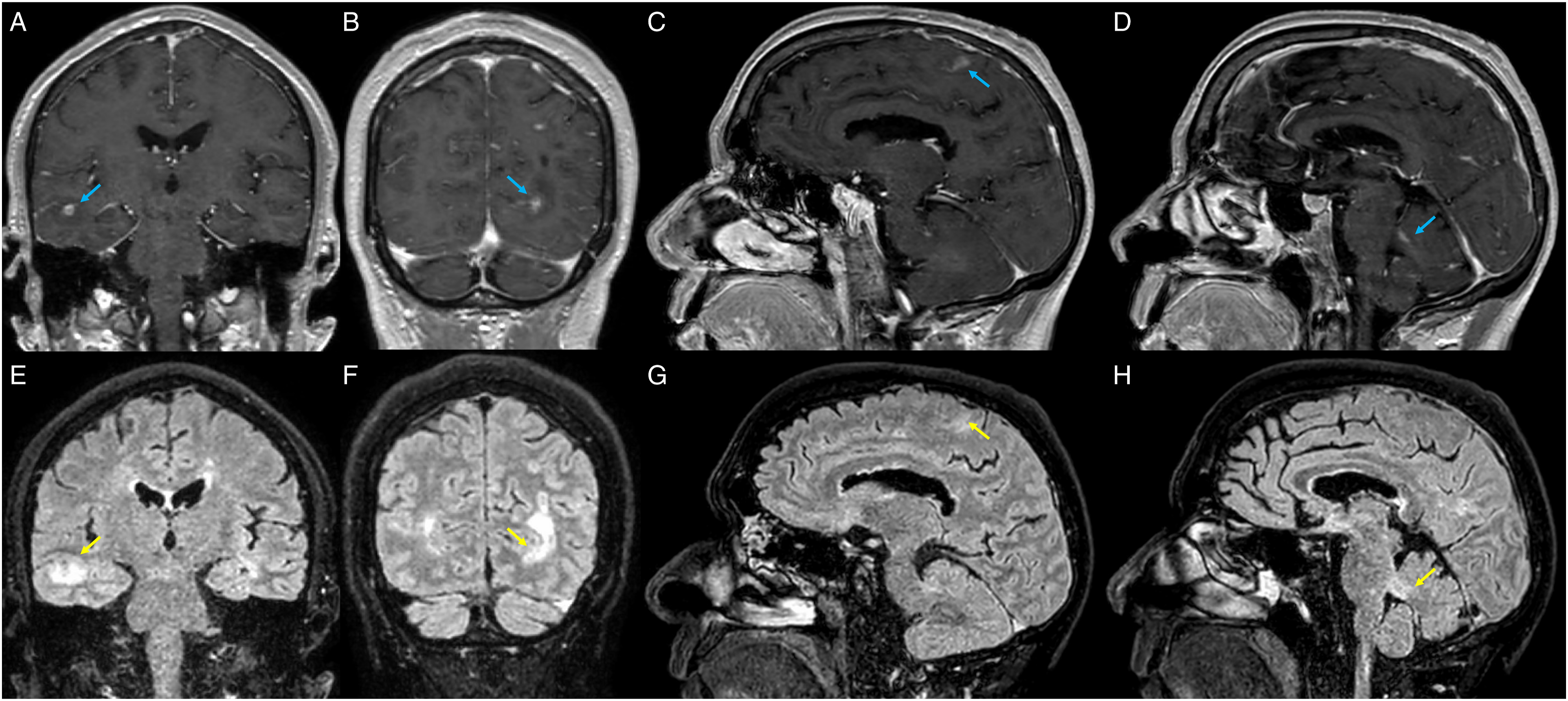
A 67-year-old man with relapsing-remitting multiple sclerosis (MS) presented to the emergency department with word-finding difficulties and gait instability. His MS had previously been well-controlled with fingolimod for 6 years. He was not on any other immunosuppressant. A brain MRI with and without contrast revealed multiple juxtacortical, deep, and periventricular white matter lesions, and new enhancing lesions (Figures 1A-1H, blue arrows, T1 post-contrast) in the parenchyma and leptomeninges with corresponding cortical and subcortical T2 hyperintensities (Figures 1E-1H, yellow arrows, T2/FLAIR). His brain MRI 10 months prior is shown for comparison (Figures 1I-1L, T2/FLAIR). The enhancing lesions (Figures 2A-2D) and corresponding T2 hyperintensities (Figures 2E-2H) are redemonstrated in coronal and sagittal views. Axial T1 post-contrast images (A-D) on brain MRI show enhancing lesions in parenchyma and leptomeninges (blue arrows), corresponding to T2/FLAIR (E-H) hyperintensities (yellow arrows). Axial T2/FLAIR images from 10 months before (I-L) are provided for comparison. Coronal and sagittal T1 post-contrast images (A-D) demonstrate enhancing lesions (blue arrows) with surrounding edema, corresponding to T2/FLAIR (E-H) hyperintensities (yellow arrows).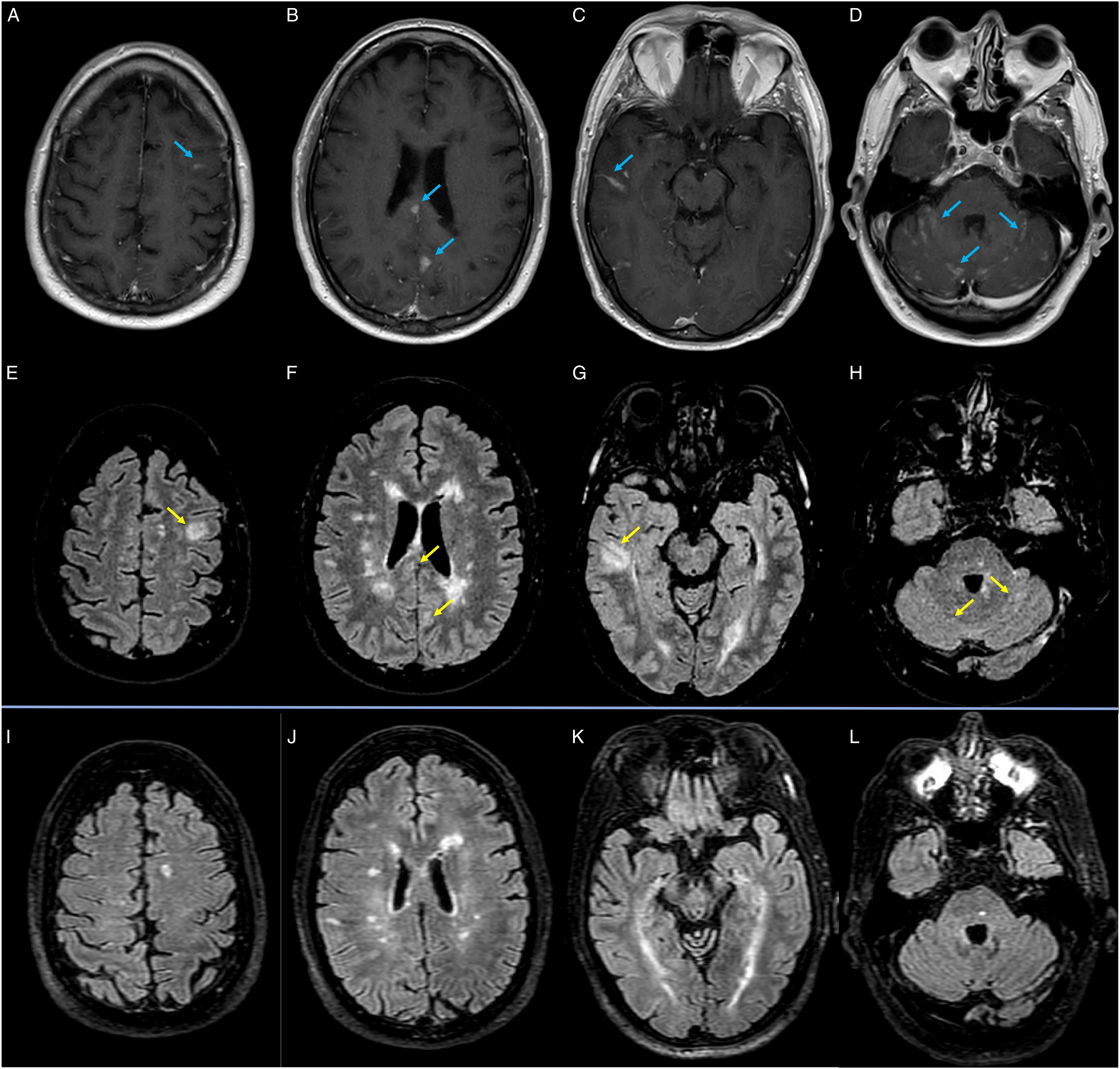
Initially thought to have an MS flare, he received 1 gram of intravenous methylprednisolone and was discharged from the hospital on oral prednisone. Two days later, he returned with a worsening headache and confusion. Serum and cerebrospinal fluid analyses confirmed the diagnosis of meningoencephalitis by Cryptococcus neoformans (Supplemental Table).
Recent growing evidence suggests that long-term treatment with fingolimod can be associated with the development of cryptococcal meningitis. 1 Neuroimaging results of cryptococcal meningitis are variable and may show intraparenchymal lesions mimicking those of an MS flare.2,3 Red flags in our patient’s imaging included bilateral cerebellar folial leptomeningeal enhancements and large, globular T2 lesions, some cortical, with associated leptomeningeal enhancement, which are atypical for MS.4–6 In evaluating patients taking fingolimod, the presence of new onset headaches, altered mental status, or leptomeningeal enhancement on MRI should raise suspicion for cryptococcal meningoencephalitis.
Supplemental Material
Supplemental Material - Cryptococcal Meningoencephalitis Mimicking a Multiple Sclerosis Flare in a Patient Taking Fingolimod
Supplemental Material for Cryptococcal Meningoencephalitis Mimicking a Multiple Sclerosis Flare in a Patient Taking Fingolimod by Daniel J. Zhou, Miguel Situ-Kcomt, and Mac T. McLaughlin in The Neurohospitalist
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.