
Abstract
Objectives
Sensitivity and specificity of Repetitive Nerve Stimulation (RNS) is typically reported from outpatient centers, and we hypothesized that these values might not apply to hospitalized patients with higher grades of weakness. RNS may be helpful in rapidly confirming diagnosis of myasthenia gravis (MG) in the inpatient setting, as results from confirmatory antibody testing are often delayed. We sought to characterize the sensitivity and specificity of RNS in the inpatient setting to assist in the early diagnosis of MG.
Methods
We performed a retrospective analysis of all adult patients who had inpatient RNS at our center from 2016 to 2021. Inclusion criteria included RNS performed at least at one site and a neurological evaluation which prompted an electrodiagnostic study to evaluate for neuromuscular junction (NMJ) pathology. Descriptive statistics and Fisher exact analysis were performed.
Results
Of the 32 identified hospitalized patients, 6 had greater than 10% decrement on slow RNS, confirming NMJ dysfunction. Five were diagnosed with MG, and 1 with Lambert-Eaton myasthenic syndrome. Of the 26 patients with normal RNS, 25 ultimately had alternative causes of weakness. One was later diagnosed as seronegative MG based on clinical improvement with acetylcholinesterase inhibitors. In our inpatient population, the overall sensitivity and specificity of RNS were 83.3% and 96.2% respectively. There was a statistically significant association between a positive RNS and diagnosis of MG (P = .0002).
Conclusions
RNS is a highly sensitive and specific test for the diagnosis of MG in an inpatient setting, and these results are likely more rapidly available compared to antibody testing.
Keywords
Introduction
Repetitive nerve stimulation (RNS) is a common electrodiagnostic test in the diagnosis of myasthenia gravis (MG). Prior studies characterizing the diagnostic sensitivity of RNS have yielded a wide range from 30% to 90% for generalized MG and 10% to 60% for ocular MG.1-4 However, the majority of these studies include a heterogeneous cohort of patients and do not differentiate between outpatient and inpatient cohorts. There is limited evidence examining the sensitivity of RNS in the inpatient setting, even though hospitalized patients present with higher grades of weakness, and diagnostic certainty is needed on a more urgent basis so appropriate therapeutic intervention can be started. Given that the diagnostic sensitivity of RNS increases with the severity of MG, RNS could perhaps serve as a first line diagnostic test in the inpatient setting. One retrospective study suggests that RNS is a sensitive test to diagnose MG when performed in patients presenting with myasthenic crisis. 5 We sought to examine the yield of RNS in both aiding in the rapid inpatient diagnosis of MG and in ruling out a neuromuscular junction (NMJ) pathology in patients presenting with varying patterns of neuromuscular weakness.
Methods
We performed a retrospective analysis of all patients at least 18 years old who had inpatient RNS at the Stanford University Medical Center from June 2016 to August 2021. Inclusion criteria included an inpatient neurological evaluation that led to a request for an inpatient electrodiagnostic study to confirm or exclude a NMJ pathology. Nerve conduction studies (NCS) and electromyography (EMG) were performed to address each clinical presentation. Slow RNS at 2 Hz was performed in at least one site (ulnar, median, spinal accessory, facial nerves), and recording electrodes were placed on the abductor digiti minimi (ADM) for ulnar, abductor pollicis brevis (APB) for median, trapezius for spinal accessory, and nasalis or orbicularis oculi for facial nerve. Sites of RNS were selected based on practicality, tolerability, and the clinical pattern of weakness. Positive RNS was defined as a decrement in compound muscle action potential (CMAP) amplitude of at least 10% from the first to the fourth stimuli. While abnormal decrement on slow RNS supported a diagnosis of NMJ pathology, a final diagnosis of MG was further confirmed based on clinical findings, responsiveness to acetylcholinesterase inhibitors, and/or MG antibody positivity (i.e., acetylcholine receptor (AChR) antibody or muscle-specific tyrosine kinase (MuSK) antibody positive). Descriptive statistics and Fisher exact analysis were performed. This study was approved by the institutional review board (IRB) at Stanford University.
Results
Patient Demographics and Clinical Presentation Prompting Study, RNS Data, and Ultimate Diagnosis.
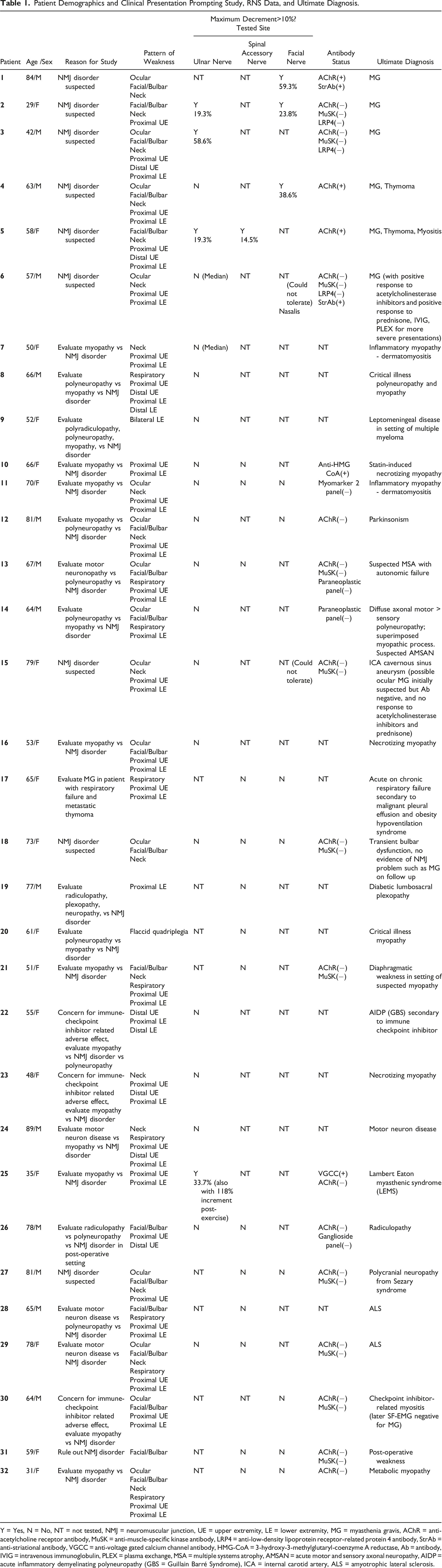
Y = Yes, N = No, NT = not tested, NMJ = neuromuscular junction, UE = upper extremity, LE = lower extremity, MG = myasthenia gravis, AChR = anti-acetylcholine receptor antibody, MuSK = anti-muscle-specific kinase antibody, LRP4 = anti-low-density lipoprotein receptor-related protein 4 antibody, StrAb = anti-striational antibody, VGCC = anti-voltage gated calcium channel antibody, HMG-CoA = 3-hydroxy-3-methylglutaryl-coenzyme A reductase, Ab = antibody, IVIG = intravenous immunoglobulin, PLEX = plasma exchange, MSA = multiple systems atrophy, AMSAN = acute motor and sensory axonal neuropathy, AIDP = acute inflammatory demyelinating polyneuropathy (GBS = Guillain Barré Syndrome), ICA = internal carotid artery, ALS = amyotrophic lateral sclerosis.
Twenty studies were performed on the ulnar nerve, 15 studies were performed on the spinal accessory nerve, 2 on the median nerve, and 11 on the facial nerve; with 14 studies including RNS on greater than one nerve (Table 1). 6 out of 32 patients (19%) had greater than 10% decrement on slow RNS confirming underlying NMJ dysfunction. Five out of these 6 patients (83%) with positive RNS were diagnosed with MG and one was diagnosed with Lambert-Eaton myasthenic syndrome (LEMS). One patient who did not have significant decrement in median nerve RNS and could not tolerate facial RNS, was later diagnosed with seronegative MG based on persistent clinical improvement with acetylcholinesterase inhibitors.
Of the 6 patients receiving a diagnosis of MG, 3 were AChR antibody-positive; the remainder were seronegative (AChR, MuSK, and LRP4 negative). The patient with LEMS also had a significant increment (>100%) in CMAP post exercise and later voltage-gated calcium channel antibodies returned positive, and she was eventually diagnosed with autoimmune LEMS.
Of the 6 MG patients, 5 were treated with immunomodulatory therapy at the time of evaluation; 3 were treated with intravenous immunoglobulin (IVIG), 2 with plasma exchange (PLEX), and all 5 with concurrent prednisone. The patient with LEMS was not on therapy at the time of the study.
Of the 3 patients who had a known thymoma at time of study, one received a new diagnosis of MG confirmed with positive RNS. The other 2 patients with thymoma with normal RNS studies received respective diagnoses of myositis secondary to immune checkpoint inhibitor therapy and acute on chronic respiratory failure secondary to malignant pleural effusions.
Twenty five out of the 26 patients with normal RNS were found to have alternative causes of weakness (Table 1). These included, but are not limited to, motor neuron disease, inflammatory myopathy, critical illness myopathy and polyneuropathy, and checkpoint inhibitor associated myopathy and polyneuropathy.
In our inpatient population, the overall sensitivity and specificity of RNS in the diagnosis of MG were 83.3% and 96.2% respectively. There was a statistically significant association between a positive RNS and diagnosis of MG (P = .0002).
Discussion
In this retrospective analysis, we demonstrate that inpatient RNS is both a sensitive and specific test to evaluate for MG in hospitalized patients presenting with acute weakness. Our study adds to the wider literature demonstrating the utility of inpatient electrodiagnostic studies in the evaluation and acute management of patients with suspected neuromuscular disease. 7
In one of our cases, an abnormal RNS study supported clinical suspicion for MG, prompting rapid initiation of treatment with immunotherapy and acetylcholinesterase inhibitor immediately following the study, while antibody results were still pending (later returned AChR-positive). Confirmatory testing such as antibody testing for AChR or MuSK antibodies usually take longer than 7 days at most medical centers, as these are not performed locally at most hospital clinical laboratories. While this delay in obtaining diagnosis might not be critical in patients who are not critically ill, in patients presenting as an atypical myasthenic syndrome or in myasthenic crisis, timely and accurate diagnosis is critical. Our study, similar to others, 5 suggests that RNS serves this purpose well.
Single-fiber EMG (SFEMG) is reported to be more sensitive (90-98%) than RNS; 8 however, SFEMG is more technically difficult to perform, is not as widely available (especially in the inpatient setting), and may not be as specific in diverse populations with non-NMJ related weakness. Although SFEMG remains a gold standard electrodiagnostic test for MG, targeted RNS may offer an equally sensitive and more rapid diagnosis in certain clinical contexts.
It is important to acknowledge that the sensitivity of RNS depends on multiple factors including distribution and severity of muscle weakness.3,9 While accounting for heterogeneity of sites tested, the sensitivity of RNS in our study may be relatively higher than other cohorts1-4,10 due to higher grades of weakness in hospitalized patients. This likely supports the finding of higher sensitivity of RNS to diagnose new onset MG in patients presenting in myasthenic crisis. 5 In contrast, one study found that some patients with acute MG presentation even with MGFA 4B classification, did not have significant decrement in repetitive stimulation. 11 In an inpatient cohort with higher severity of weakness, the presence of alternative diagnostic findings on EMG/NCS, in addition to a negative RNS, improves the degree of diagnostic certainty in ruling out MG. We also note that our study was designed to calculate the sensitivity and specificity of RNS for the diagnosis of MG in particular. The patient with a diagnosis of LEMS therefore represented an important false positive, while still accurately assessing for and distinguishing between disorders of NMJ dysfunction.
Limitations of our study include its retrospective nature and variation in RNS site selection, but this likely reflects clinical practice across many large academic centers. We have a relatively small number of patients with an ultimate diagnosis of MG in our cohort. This is likely because we offer prompt electrodiagnostic testing at our center for our inpatient services with dedicated staff, leading to heterogeneity of ultimate diagnoses. We also had a relatively high percentage of seronegative generalized MG (50%) compared to the general population, 12 which likely reflects a biased inpatient population. As SFEMG was not performed in our MG cohort, we did not have an additional gold standard test to confirm the RNS results particularly in our seronegative patients, however our MG patients met accepted diagnostic criteria used in clinical trials. We also recognize that inpatient electrodiagnostic studies, particularly those performed in the intensive care unit, are at increased risk of being affected by artifact. However, within our cohort, there were no concerns that study quality was suboptimal to address the clinical question.
In conclusion, targeted RNS offers rapid results which would aid in more timely diagnosis. Given its relatively high specificity and sensitivity, RNS should be considered and more widely adopted in the inpatient diagnosis of MG.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.