
Abstract
This case describes a 76-year-old male with initial clinical concern for a high-grade glioma, who was ultimately diagnosed with cerebral amyloid angiopathy-related inflammation The patient’s presentation included a tonic-clonic seizure followed by aphasia and right-sided hemiparesis. Magnetic resonance brain imaging demonstrated a large left frontal lesion with parenchymal contrast enhancement. Magnetic resonance spectroscopy indicated elevated choline to creatine and choline to N-acetyl aspartate ratios, further suggestive of high-grade glioma. However, subsequent biopsy findings revealed perivascular amyloid deposits, confirming the diagnosis of CAA-ri. To our knowledge, this is the first case in literature to report elevated choline to creatine and choline to N-acetyl aspartate ratios in cerebral amyloid angiopathy-related inflammation.
Keywords
Introduction
Cerebral amyloid angiopathy (CAA) represents a spectrum of disease, characterized by amyloid beta-peptide deposition within small-to-medium sized blood vessels of the brain and leptomeninges. While the most widely recognized clinical feature of CAA involves lobar intracerebral hemorrhages, non-hemorrhagic manifestations of CAA have also been described in literature. 1 These include cognitive decline, transient focal neurological episodes, and inflammation associated encephalopathy. 2 The inflammatory phenotype, known as CAA-related inflammation (CAA-ri), is an autoimmune response to vascular amyloid. This response is associated with an increase in CSF concentrations of autoantibodies targeting beta-amyloid. 3 Typically, patients with CAA-ri present with acute/subacute cognitive decline and new-onset seizures. 4 However, the clinical spectrum can include stroke-like symptoms, cranial nerve palsies, or tumefactive effects, complicating accurate diagnosis and treatment. Due to its potential reversibility with immunosuppressive therapy, a diagnosis of CAA-ri should warrant a high level of suspicion given appropriate physical examination and imaging. 5 Our case describes a patient with CAA-ri, masquerading as high-grade glioma due to prominent parenchymal enhancement on magnetic resonance (MR) brain imaging and elevated choline to creatine (Cho/Cr) ratio and choline to N-acetyl aspartate (Cho/NAA) ratio on MR spectroscopy (MRS). The correct diagnosis was acquired after biopsy confirmation. In this report, we sought to review this uncommon presentation of CAA-ri to describe features which may facilitate early recognition of this entity.
Case Presentation
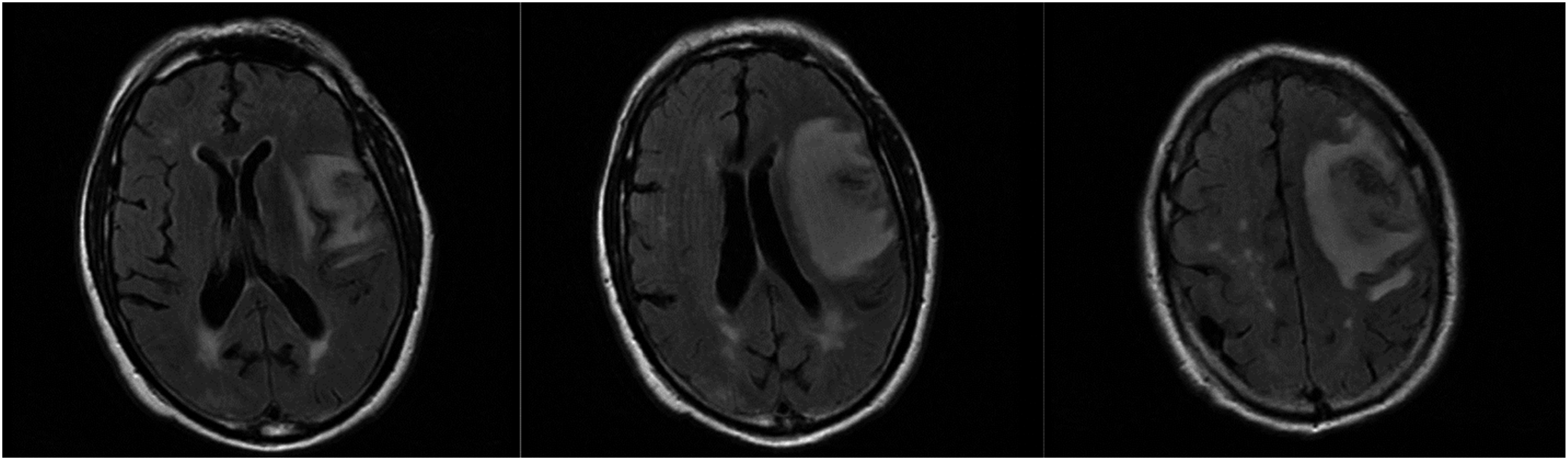
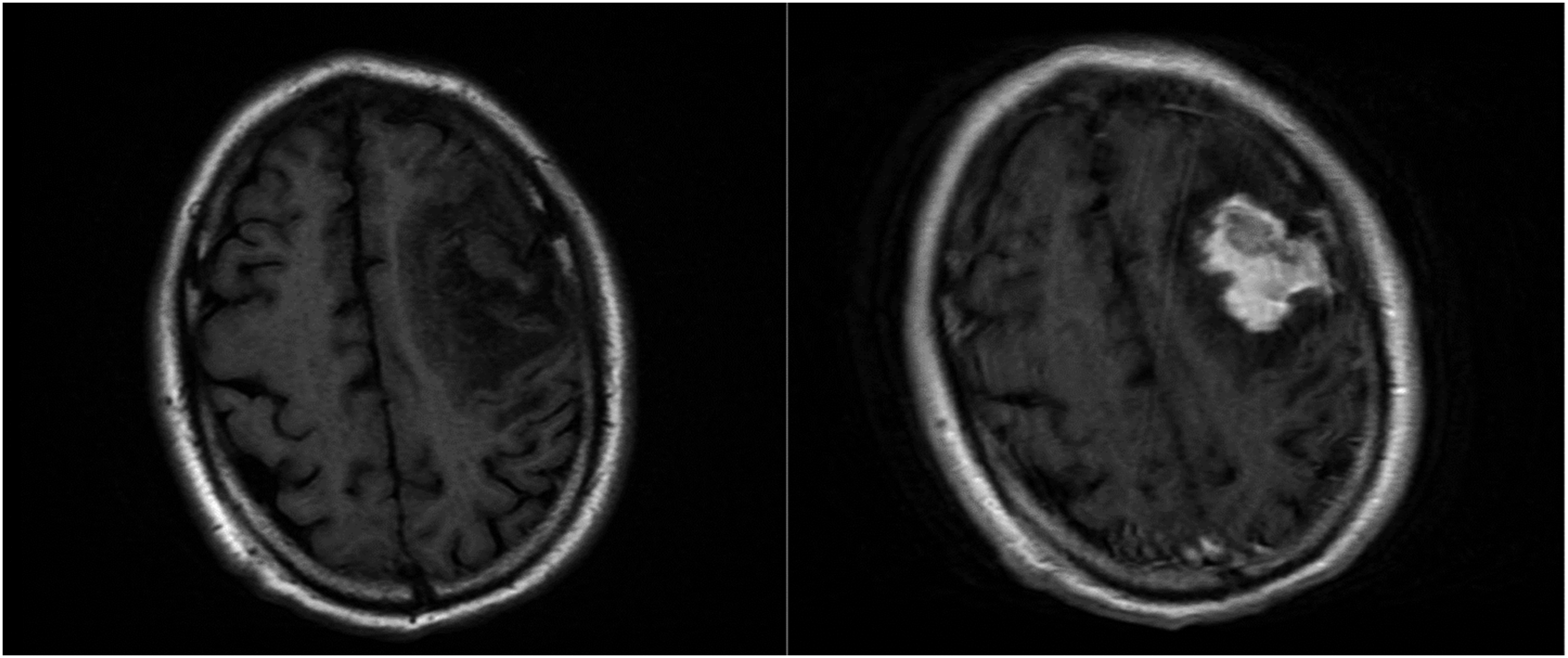
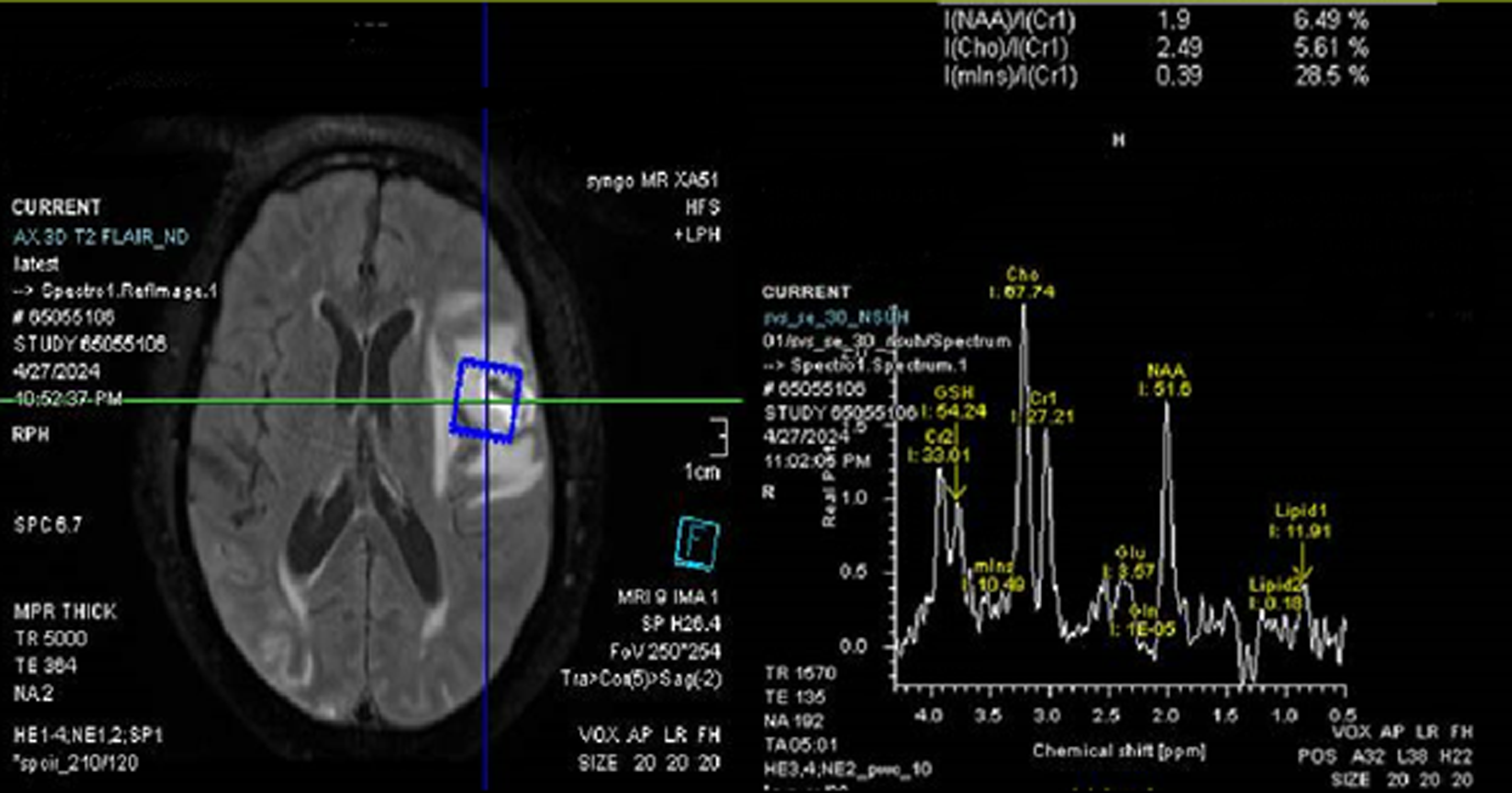
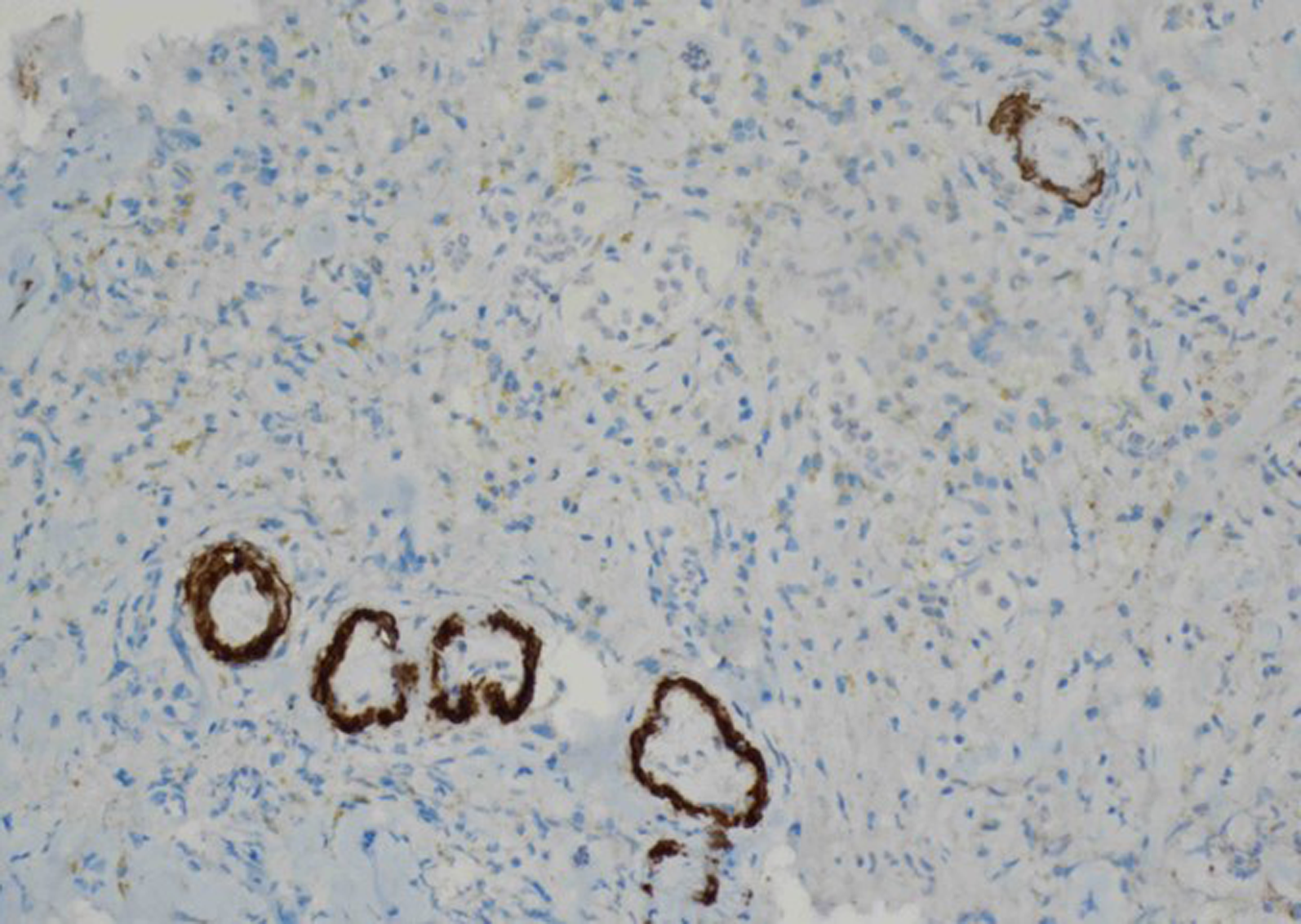
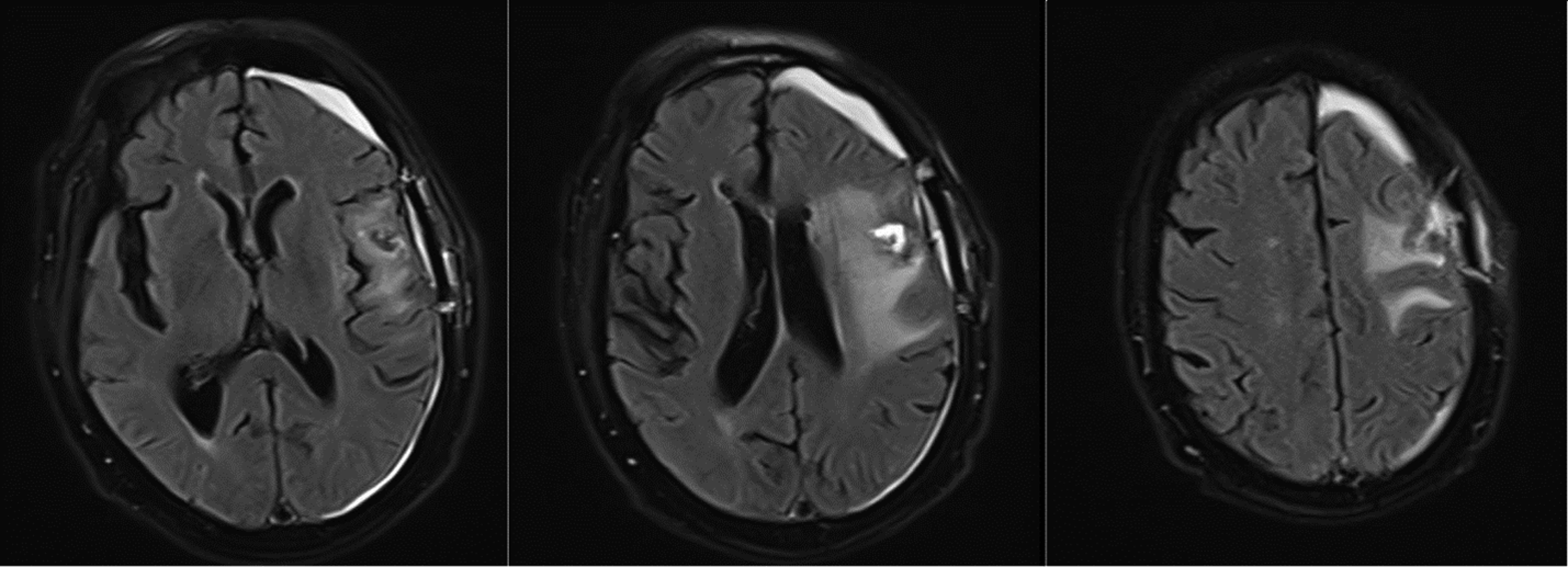
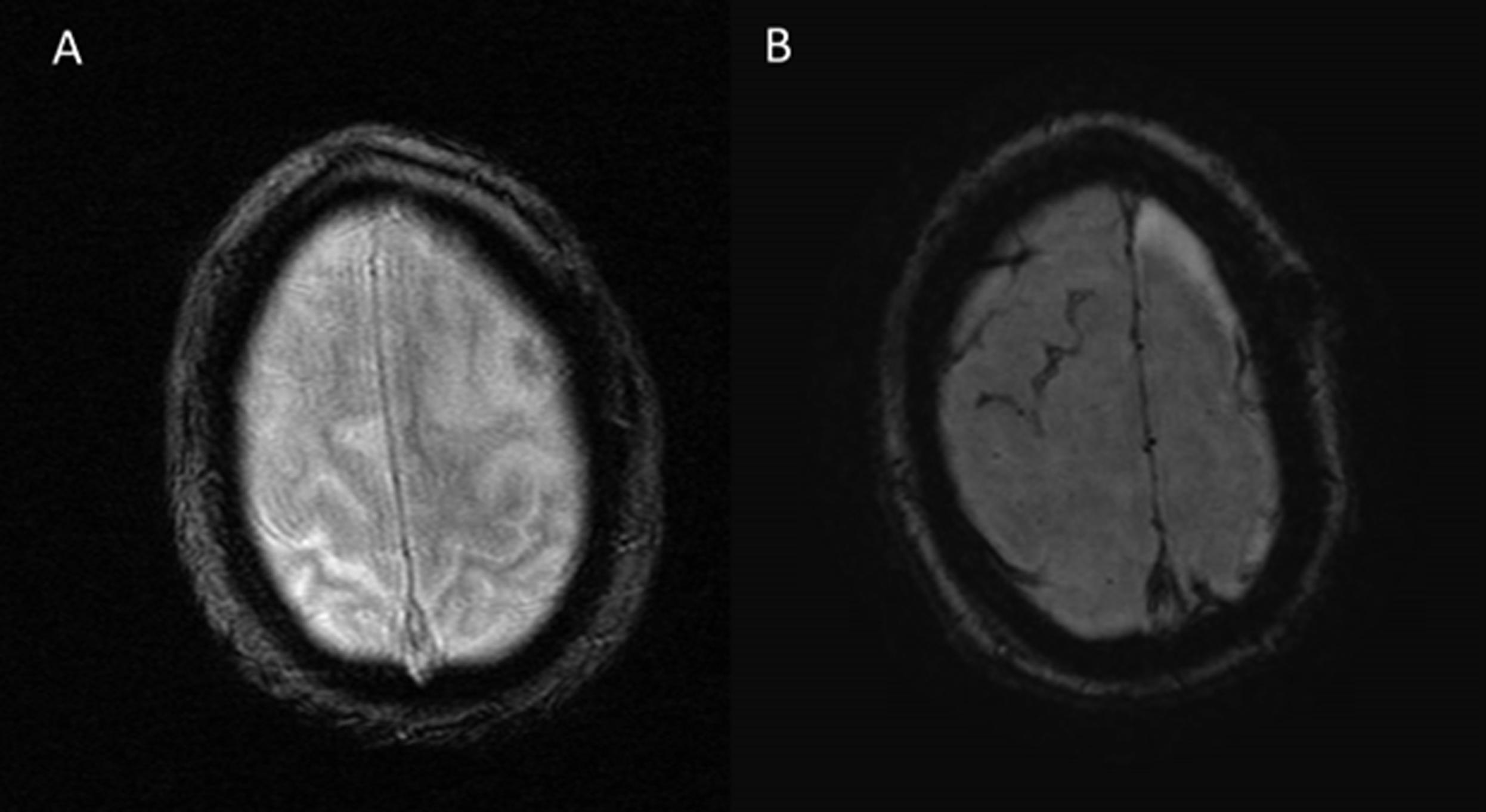
A 76-year-old male presented with a new-onset generalized tonic-clonic seizure followed by aphasia and right-sided hemiparesis. His past medical history was remarkable for hypertension and prostate cancer. Prior to this event, the patient was independent at his baseline. His neurological examination revealed non-fluent aphasia, a right facial droop, and right-sided hemiparesis in the range of 3/5. Initial computed tomography (CT) of the head demonstrated a large hypodense lesion in the left frontal lobe with extension to subcortical structures (Figure 1). CT angiogram of the head and neck did not reveal any evidence of vascular pathology, including vasculitis. The patient was admitted with an initial diagnosis of ischemic stroke; however, a subsequent MR brain demonstrated no diffusion restriction. MR brain also revealed a large left frontal region of hyperintense signal on T2/fluid attenuated inversion recovery (FLAIR) with contrast enhancement (Figures 2 and 3). Gradient echo (GRE) showed a 2 × 3 cm hemorrhagic core of the lesion; however, there was no evidence of cortical microbleeds or superficial siderosis. At this point, a diagnosis of high-grade glioma was considered. An MRS was obtained, demonstrating an elevated Cho/Cr and Cho/NAA ratios (Figure 4), which further supported a diagnosis of a high-grade glioma. Notably, laboratory investigations were unremarkable for infectious or autoimmune processes. The patient then underwent an open biopsy of the left frontal lesion which revealed extensive lymphocytic and histiocytic infiltration with hemosiderin deposition. The resulting immunostaining was positive for beta-amyloid, indicating the presence of CAA (Figure 5). The patient was subsequently treated with pulse methylprednisolone followed by a prednisone taper with significant improvement in his neurological exam. A follow-up MR brain study completed 4 weeks after the initial presentation showed markedly decreased size of the lesion (Figure 6). In addition, susceptibility weighted imaging (SWI) demonstrated evidence of superficial siderosis, supporting the diagnosis of CAA-ri (Figure 7). Initial CT head demonstrating a large hypodense left frontal lesion. Initial MR brain demonstrating hyperintense T2/FLAIR lesion in the left frontal lobe, extending into the subcortical areas. T1 pre and post contrast images, demonstrating prominent gadolinium enhancement. MRS shows an increased choline (Cho) level of 67.74, a decreased N-acetyl aspartate (NAA) level of 51.6, and a normal creatine (Cr) level of 27.21 in the lesion. The Cho/Cr ratio is elevated at 2.49, and the Cho/NAA ratio is elevated at 1.31. Immunohistochemistry demonstrating perivascular amyloid deposits. Follow up MR brain in 4 weeks, demonstrating post-biopsy changes and a significant reduction of the lesion on T2/FLAIR status post steroid treatment. A, GRE sequence on the initial MR brain did not show superficial siderosis. B, The 4-week follow-up MR brain scan demonstrated superficial cortical siderosis on the SWI sequence.
Discussion
Manifestations of CAA-ri are nonspecific. Patients most often present with subacute cognitive decline, seizures, and focal neurological deficits. The diagnostic process can be complex, requiring a comprehensive evaluation and consideration of a wide differential diagnosis. In our case, the patient presented with a first-time episode of generalized tonic-clonic seizure, aphasia, and right-sided hemiparesis, and was found to have an infiltrating T2/FLAIR hyperintense lesion. Given the prominent parenchymal T1 contrast enhancement on MR brain and MRS with findings of elevated Cho/Cr ratio, there was a high suspicion of high-grade glioma. The patient subsequently underwent a biopsy, of which the pathology was negative for malignancy and demonstrated amyloid deposits. As suggested by Auriel et al. (2016), in most of CAA-ri cases diagnoses can be established solely on clinic radiological criteria without a requirement for a biopsy. 6 However, in our case, a malignant neoplasm could not be excluded based on clinic radiological criteria alone and, therefore, a biopsy was performed. After immunohistochemistry revealed amyloid deposits, the patient met the criteria of probable CAA utilizing the Boston Criteria v2.0. 7 Notably, the initial MR brain GRE sequence did not demonstrate evidence of superficial siderosis, which was later observed on the follow-up MR brain with the SWI sequence. SWI generally offers greater sensitivity for detecting cortical microhemorrhages and superficial siderosis. 8 It is highly unlikely that the surgical biopsy led to the interval development of superficial siderosis, as this pathology is quite specific to CAA. 9
As mentioned in the introduction, CAA represents a spectrum of disease. Classical CAA manifests with cerebral microhemorrhages, superficial siderosis, and lobar intracranial hemorrhages. CAA-ri, on the other hand, represents a non-hemorrhagic spectrum, where the predominant pathophysiology is an autoimmune inflammatory response to beta-amyloid.1,5
The probable criteria for CAA-ri include age ≥40 years, presence of ≥1 features: headache, decrease in consciousness, behavioral change, or focal neurological signs and seizures. The third criterion is unifocal or multifocal WMH lesions on MRI that are asymmetric and extend to subcortical white matter. The fourth criterion is presence of ≥1 corticosubcortical hemorrhagic lesions, and the last criterion is absence of neoplasm or infection. Following a negative biopsy for malignancy, our patient fit in the criteria of probable diagnosis for CAA-ri.
Ronsin et al. (2016) postulates that CAA-ri usually presents as a non-enhancing mass with hyperintense signal on T2/FLAIR and normal metabolic ratios on MRS, resembling a low-grade glioma. 10 In their case series, only 2 out of 28 patients had parenchymal T1 contrast enhancement. MRS was performed in 7 patients and demonstrated normal Cho/Cr and Cho/NAA ratios. Notably, leptomeningeal enhancement was observed in 11 patients. Salvarani et al. (2016) included 5 biopsy proven patients with CAA-ri in a single-institution study and demonstrated similar findings: 4 out 5 patients were found to have leptomeningeal T1 contrast enhancement, and no parenchymal enhancement was observed. 11 However, MRS was not utilized. A larger retrospective cohort study from 2020 reviewed 48 patients with CAA-ri diagnosed with biopsy or with probable clinic radiological criteria for CAA-ri. 5 Again, a similar pattern was noted: a minority (10 out 48) of the patients had a parenchymal T1 contrast enhancement, and MRS was also not utilized. A recent case series further supported this data: only 11 out of 128 patients had parenchymal enhancement on MR, however, half of the patients (49%) had leptomeningeal enhancement. 12 Given the high prevalence of leptomeningeal enhancement, the authors proposed to include these findings in the clinic radiological criteria of CAA-ri. To summarize, the presence of significant T1 gadolinium parenchymal enhancement would be considered unusual for tumefactive presentation of CAA-ri and thus require further investigation with additional testing such as MRS and/or biopsy.
MRS has been established as a valuable tool to enhance the diagnostic precision of brain neoplasms. 13 MRS complements MR imaging by revealing biochemical changes in tissue and analyzing metabolite profiles in specific brain regions. Both high-grade and low-grade gliomas are characterized by an elevated Cho/Cr ratio with decreased NAA, with high-grade gliomas showing a higher contrast in values. 14 Despite the more robust literature on CAA-ri in recent years, there is a paucity of clinical data regarding the MRS pattern in CAA-ri. Safriel et al. (2004) described two patients with confirmed CAA-ri, where MRS demonstrated a normal Cho/Cr and Cho/NAA ratios. 15 Ronsin et al. (2016) demonstrated the same pattern in their case series. 10
In our patient, however, MRS showed increased Cho/Cr and Cho/NAA ratios which would be more typical for CNS malignancy rather than CAA-ri. To our knowledge, this is the first case in the literature to report such a finding. The exact pathophysiology behind the increased MRS ratios in CAA-ri is unclear and requires further investigation. Inflammation within brain tissue can lead to an increase in Cho and a decrease in NAA, resulting in a shift in the ratios. 16 One possible explanation for the abnormal MRS in our case is that the prominent inflammatory response to beta-amyloid mimicked a neoplastic process.
Conclusion
Cases of CAA-ri presenting with clinical and radiological appearances of an intracranial mass are rare. Case series and retrospective studies have described non-enhancing lesions with initial suspicion of low-grade tumors, such as astrocytoma. MR spectroscopy data are limited, but reported cases demonstrated a normal Cho/Cr and Cho/NAA ratios. In our case, the patient presented with T1 contrast enhancing parenchymal lesion and increased Cho/Cre and Cho/NAA ratios on MRS with initial clinical concern for a high-grade glioma. Despite the more robust literature on CAA-ri in recent years, diagnosis of CAA-ri with a tumefactive presentation remains a clinical challenge. Our case emphasizes the need for further clinical research and data collection, particularly regarding the MR spectroscopy patterns.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.