
Abstract
Myelin oligodendrocyte glycoprotein (MOG) antibody-associated optic neuritis is a demyelinating disease that shares clinical overlap with Neuromyelitis Optica Spectrum Disorder (NMOSD) and Multiple Sclerosis (MS). The immunosuppressive effects of pregnancy followed by a rebound in the immune system postpartum are thought to affect presentation and relapse rates of NMOSD and MS. Few studies exist describing pregnancy affecting MOG antibody-associated disease. In this case, a 29-year-old female from Ethiopia presented on postpartum day 8 with 4 weeks of progressive, painful bilateral vision loss that had acutely worsened over the past 6 days. Her visual acuity was light perception in the right eye and hand motion in the left eye with a right afferent pupillary defect. Dilated exam revealed bilateral optic nerve head elevation, vascular tortuosity, and macular folds. MRI of the brain and orbits with contrast revealed long segment bilateral optic nerve enhancement and nonspecific white matter changes. Serum MOG IgG was positive (1:160). Her vision rapidly improved with intravenous methylprednisolone 1000 mg daily for 5 days, followed by an oral prednisone taper. After 6 months, the patient’s vision returned to 20/20 in each eye, and she has had no further clinical relapse. This case suggests that initial presentation of MOG optic neuritis may be affected by pregnancy. Physicians must appropriately triage patients with postpartum vision changes to ensure prompt treatment.
Introduction
Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) is an antibody-mediated demyelinating central nervous system disorder that frequently presents as isolated optic neuritis. 1 It is recognized as an immunologically and histopathologically distinct disease from aquaporin-4 antibody neuromyelitis optica spectrum disorders (AQP4-IgG NMOSD), however, they share many clinical features.1-3 Small retrospective studies have indicated that the postpartum period may increase the risk of presentation and relapse rates of NMOSD. 2 Three small retrospectives studies have also suggested that MOG antibody-associated disease may be similarly exacerbated by hormonal and immunologic changes after pregnancy.1,4,5 The authors describe an acute initial onset of severe vision-threatening MOG optic neuritis in late pregnancy to contribute toward our evolving understanding of pregnancy influencing MOG antibody-associated disease.
Case Report
A 29-year-old Ethiopian female presented to the emergency department postpartum day 8 with a 4 week history of progressive, painful bilateral vision loss that acutely worsened over the preceding 6 days. Her pregnancy was complicated by gestational diabetes mellitus and frequent headaches. She was otherwise healthy and had an uncomplicated vaginal delivery at 37 weeks gestation. She had noticed progressive visual disturbances over the 3 weeks leading up to delivery, however an ophthalmic exam was not performed until the postpartum period. These symptoms started with stabbing eye pain, greater in the right eye than the left as well as blurry vision, but no vision loss. One week postpartum, she initially developed acute fulminant vision loss in both eyes that progressed to black out vision over several days. Her initial exam revealed visual acuity of bare light perception in the right eye and hand motion in the left eye with a right afferent pupillary defect. Her intraocular pressure, extraocular movements, and anterior segment exam were within normal limits bilaterally. Dilated eye exam revealed bilateral optic nerve head elevation, vascular tortuosity, and macular folds.
Optical coherence tomography (OCT) demonstrated bilateral retinal nerve fiber layer (RNFL) thickening, measuring 339 μm and 269 μm on the right and left, respectively. Magnetic resonance imaging (MRI) of the brain and orbits with contrast revealed long segment bilateral optic nerve central enhancement from the globes to the prechiasmatic segments, right greater than left, with mild nonspecific chronic cerebral white matter changes (Figure 1). MRI of the brain and MRI of the cervical and thoracic spine were normal. Laboratory workup including CBC, CMP, PT/INR, ESR, and CRP were within normal limits. Serum HIV, RPR, Lyme, and Aquaporin-4 antibodies were negative. Serum MOG IgG was positive in a fixed cell-based assay from ARUP labs titer (1:160). Magnetic resonance imaging (MRI) of the brain and orbits with contrast on initial presentation. T1 (above) and T2 (below) weighted MRI images reveal bilateral optic nerve central enhancement extending from the globes to the prechiasmatic segments.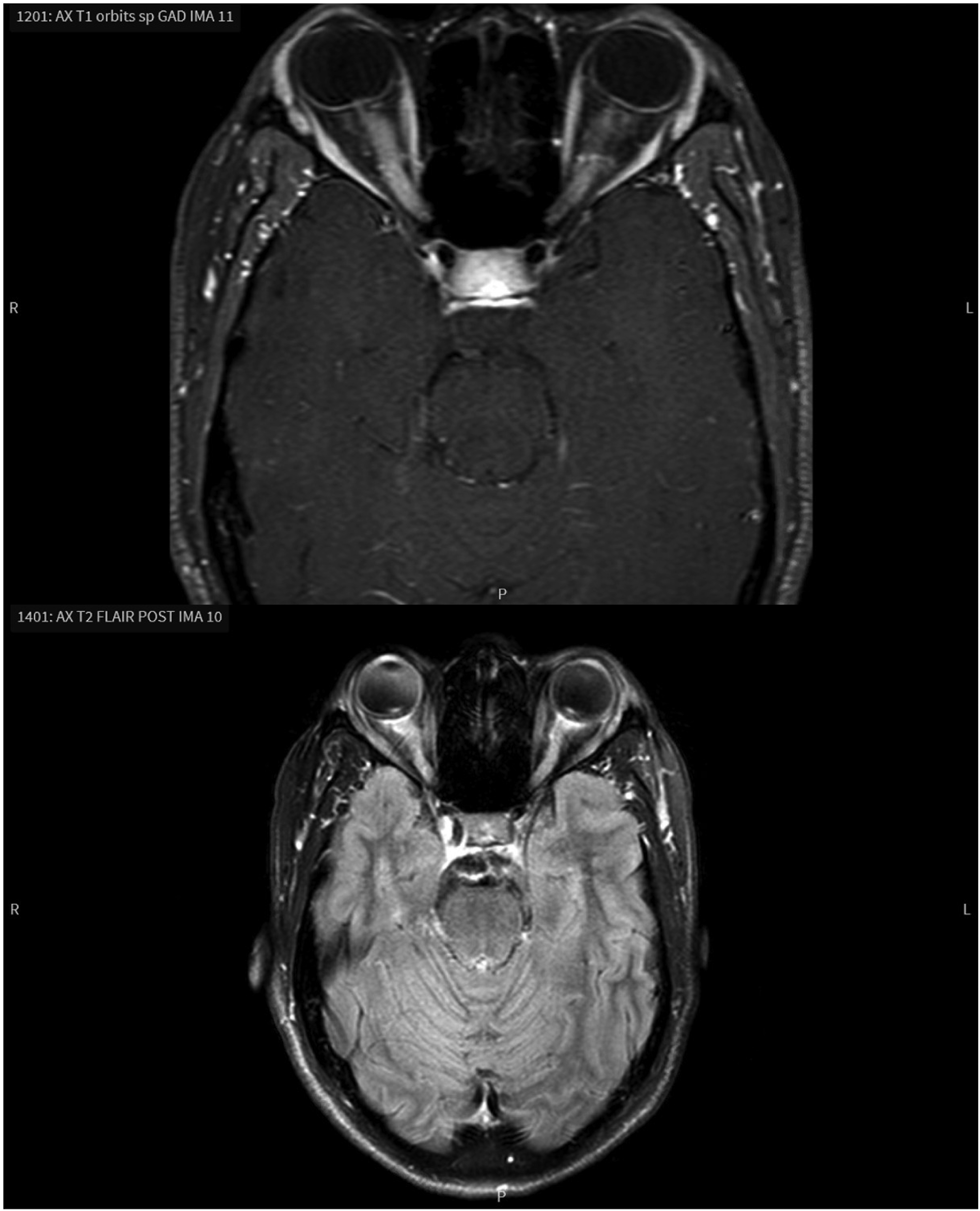
Her symptoms rapidly improved with intravenous methylprednisolone 1000 mg daily for 5 days. This was followed by oral prednisone starting at 60 mg per day and tapered slowly over 3 months. Visual acuity improved to 20/25 in each eye 12 days after initiation of steroids. Repeat OCT demonstrated more than a fifty percent decrease in RNFL thickness with 141 μm on the right and 129 μm on the left. Visual field testing revealed dense bilateral inferior field loss 12 days after initiation of steroids, which was greatly improved 3 months later (Figure 2). After 6 months, the patient had no further clinical relapse, and her vision returned to 20/20 in each eye. Humphrey visual field (HVF) 30-2 analysis at 2 time points. Twelve days after initiation of systemic steroids (above) HVF reveals dense bilateral inferior visual field loss. Three months after the first HVF, the second HVF (below) shows improvement of the inferior visual field loss bilaterally. FL: fixation losses; FP: false positive; FN: false negative; MD: mean deviation.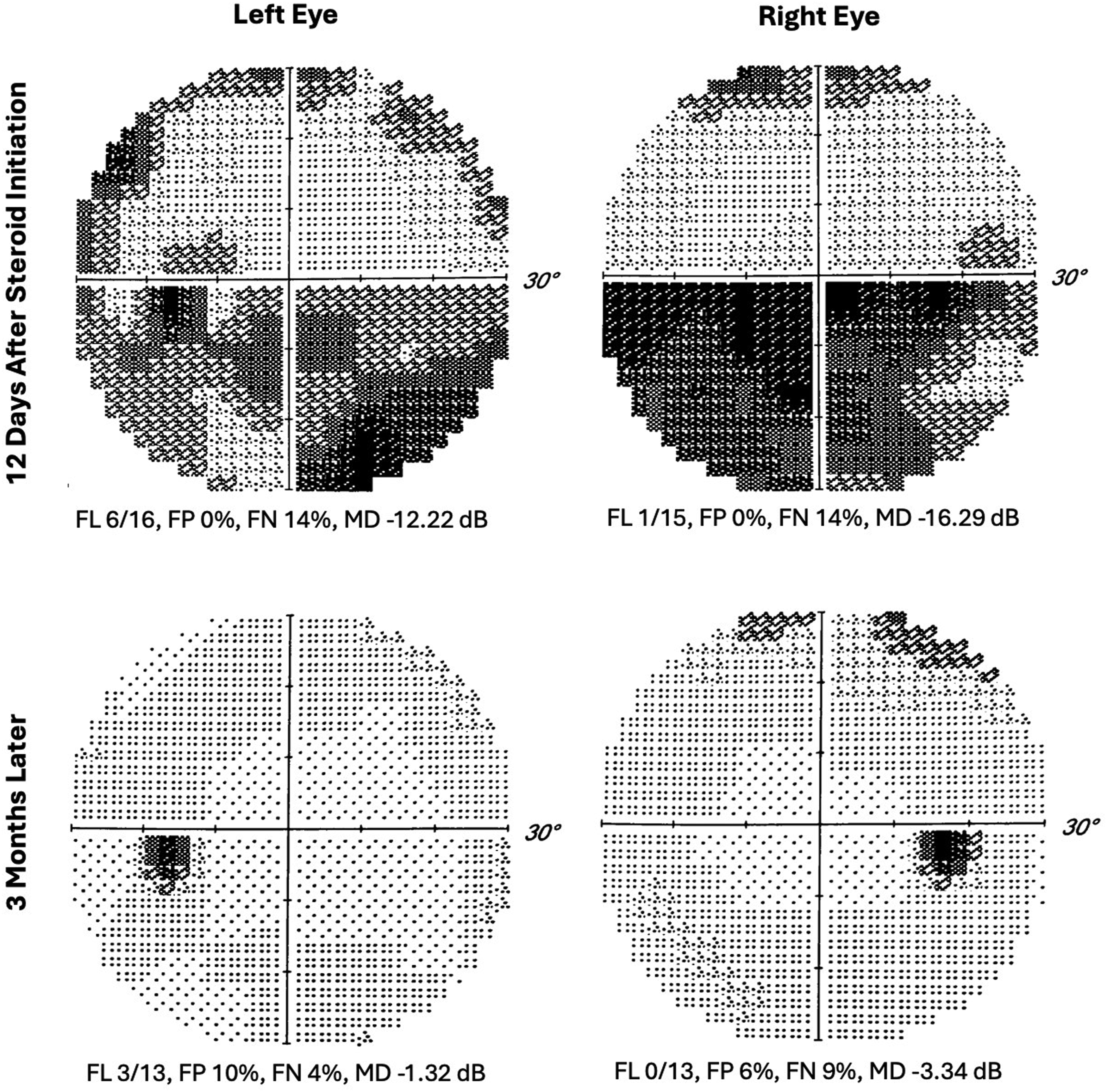
Discussion
Although limited evidence exists to determine if pregnancy-associated immunosuppressive mechanisms affect initial onset or recurrence of MOGAD, this case and similar cases indicate a possible association. Similar cases have been observed in patients with multiple sclerosis and NMOSD, where suppression of the immune system during pregnancy may lead to a rebound effect in the late third trimester and after birth. 1 Although incompletely understood, this is likely secondary to immunosuppressive mechanisms during pregnancy, which provide relative protection against demyelinating disease. 2 Our case adds to a small body of literature supporting the potential for MOGAD attacks to be suppressed by pregnancy, thus increasing the risk for relapse either during late gestation or postpartum.
In our comprehensive literature review of all pregnancy-associated MOGAD retrospective studies and case reports, we found a total of 47 patients who experienced a pregnancy-related acute initial onset of MOGAD, whether it was optic neuritis, transverse myelitis, or encephalitis.1,4-12 Of these cases, 7 were diagnosed during pregnancy, 21 were diagnosed postpartum, and 19 did not specify whether the attack was during pregnancy or in the postpartum period. Of published case reports and the detailed cases described by Jarius et al, 7 other cases have specifically reported an initial pregnancy-related onset of disease as isolated optic neuritis.1,8-10 In 2 of the cases, symptoms began in the first and third trimester. 8 In the other 5 cases the optic neuritis presented within 8 months postpartum.1,9,10
Jarius et al 1 reported a series including 3 patients with an initial onset of MOGAD in the postpartum period. The same series described 2 patients with an antenatal diagnosis of MOGAD who experienced disease relapse during pregnancy. Wang et al 5 similarly reported 5 cases of pregnancy-related MOGAD recurrence, as well as 16 cases of pregnancy-related initial disease onset. Three attacks occurred in the first or second trimester, and all other attacks occurred postpartum. The annualized relapse rate (ARR) in the 21 patients before pregnancy was 0.40 (95% CI: 0.26-0.54) and postpartum was 0.60 (95% CI: 0.38 to 0.82). They found approximately 86% of these deliveries had no complications. Collongues et al 4 reported 17 MOGAD patients with pregnancy-associated relapses and 3 patients with onset of disease during or after pregnancy. They reported a higher ARR postpartum compared with levels during pregnancy.
In contrast to other studies, Carra-Dalliere et al 7 found in 20 previously diagnosed MOGAD patients who became pregnant, there were no MOGAD relapses during pregnancy and 5 relapses within 1 year postpartum. However, 9 patients had received disease modifying therapy within 1 year prior to pregnancy and 6 continued therapy during pregnancy. The ARR was 0.67 (95% CI: 0.40-1.10) during the pre-pregnancy period and 0.22 (95% CI: 0.09-0.53) in the first year postpartum. They reported 1 miscarriage and 2 preterm births of the 25 pregnancies which is similar to complication rates seen in the general population. They separately reported 18 cases of MOGAD initially presenting during or within 1 year after pregnancy.
Regarding treatment, acute optic neuritis should be treated with several days of high-dose steroids followed by a slow oral steroid taper. 13 A recent cohort study of 240 adults found that earlier treatment of a first acute MOGAD attack decreased their risk of relapse. 14 In a patient who is currently pregnancy, oral corticosteroids should be used with minimal dose and duration depending on the severity of symptoms. 15 Although many studies have shown no fetal risks from steroid use during pregnancy, some conflicting data has shown a potential increase in risks such as preterm delivery or low birth weight. 15 In the event of relapse with persistently elevated MOG-IgG, chronic immunosuppression should be considered, such as rituximab, azathioprine, or mycophenolate. 16 Further studies are needed to determine any potential teratogenic risks from taking these medications during pregnancy, so they are generally avoided unless the benefits outweigh the risks17-19 In severe or refractory cases, especially those involving severe vision loss, plasma exchange (PLEX) followed by intravenous immunoglobulin (IVIG) can be considered during pregnancy. PLEX is generally considered safe for the mother and fetus if deemed necessary. 20 IVIG can be used to treat autoimmune disease relapses, although patients should be closely monitored for complications including preterm birth, gestational diabetes, and preeclampsia.20,21 Typically, optic neuritis due to MOGAD respond well to high dose steroids and will not require PLEX or IVIG. In cases where vision is not beginning to recover with high dose steroids, treatment with PLEX is typically recommended for use as soon as possible. While there is no prospective data to support the use of PLEX in optic neuritis, several retrospective studies suggest better outcomes of visual acuity. 22 This is particularly within 7 days or less from the onset of vision loss. 22 In the future, the use of tocilizumab, an IL-6 inhibitor, may become more frequent as it has shown promising results in small cohorts of MOGAD relapse patients who did not respond to common treatment regimens. 23 Physicians are advised to engage in patient-centered discussions regarding treatment options during pregnancy for those with a prior MOGAD diagnosis. Additionally, careful triage and management are crucial during the vulnerable postpartum period.
Consent for Publication
Written informed consent to publish this case was obtained.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Osborne receives honorarium from Alexion and Amgen for lectures on the topic of NMOSD (speakers bureau); he also receives royalties from UpToDate for chapters written on the topics of optic neuritis and optic neuropathies.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.