
Abstract
Anti-aquaporin-4 antibodies (AQP4-Ab) are highly specific for neuromyelitis optica spectrum disorder (NMOSD), but their prevalence in patients with non-inflammatory diseases, including malignant tumors, is unclear. A 54-year-old man presented with progressive weakness and dysesthesia of the right upper limb over 2 months. Cervical magnetic resonance imaging (MRI) revealed T2 hyperintense lesions in the area postrema and lower cervical/upper thoracic spinal cord, the latter of which demonstrated ring enhancement. Serum AQP4-Ab was positive on cell-based assay. He was initially diagnosed with NMOSD and treated with immunotherapy, but his neurological deficits progressed, and follow-up MRI demonstrated lesion expansion. Given the atypical course, a spinal cord biopsy was performed, and he was diagnosed with glioma with H3K27 M mutation; tumor cells were also AQP4-positive. Subsequent cancer-directed treatment led to improvement of spinal cord swelling and lesion enhancement. This case demonstrates that gliomas can present with both AQP4-Ab positivity and imaging features mimicking NMOSD, highlighting that the diagnosis of NMOSD should be based on comprehensive evaluation of antibody results, imaging findings, and the clinical course.
Keywords
Introduction
Aquaporin-4 (AQP4) is a water channel expressed on the end-foot of astrocytes in the central nervous system (CNS). Autoantibodies against AQP4 (AQP4-Ab) are known to cause neuromyelitis optica spectrum disorder (NMOSD). 1 Cell-based assays (CBA) for AQP4-Ab are now considered to have the highest sensitivity and specificity among assay techniques. 1 In the serostatus of AQP4-Ab measured using CBA during routine clinical care among patients with various neurological disorders, the specificity for the diagnosis of NMOSD was 100%. 2 However, it is not clear whether patients with malignant tumors, such as gliomas, were included in this study. The frequency of AQP4-Ab positivity in patients with non-inflammatory diseases, including malignant tumors, remains unknown. In this report, we present a patient with a high-grade glioma who presented with spinal cord and brain lesions suggestive of NMOSD, including an area-postrema lesion, and a ring-enhancing cervical spinal cord lesion on magnetic resonance imaging (MRI) with positive AQP4-Ab in serum measured using CBA.
Case Presentation
A 54-year-old man developed progressive weakness and dysesthesia of the right upper limb over 2 months. His initial cervical MRI revealed diffuse swelling of the cervical spinal cord with T2 hyperintense signal in the area postrema, and at the C7 and Th1 levels of the spinal cord (Figure 1A). The spinal lesions showed ring enhancement after gadolinium dimeglumine was administered (Figure 1B). There was no abnormal signal in the cerebrum or the optic nerves. Blood tests were positive for AQP4-Ab, as measured by CBA. Cerebrospinal fluid tests revealed 113 cells/μL (88% polymorphonuclear cells) and a normal protein level (38.2 mg/dL). The cytological examination did not reveal any malignant cells (Class I). The patient was diagnosed with NMOSD, and four cycles of intravenous methylprednisolone (1000 mg/day for 3 days each), one course of plasmapheresis, and 5 days of intravenous immunoglobulin (0.4 g/kg/day) were administered. However, his weakness gradually progressed, extending to both upper limbs and the right lower limb, and intractable neck pain and bladder and bowel disturbance developed. A cervical spine MRI performed 4 months after the initial MRI demonstrated more diffuse enlargement of the cervical spinal cord, longitudinal extension of the T2 hyperintense lesion, and an increased number of ring-enhancing lesions (Figure 1C and D). (A–D) MRI of the lower brainstem to cervical spinal cord. The initial MRI shows diffuse swelling of the spinal cord and T2 hyperintense intramedullary lesions in the area postrema (arrowhead) and at the C7 and Th1 levels (A). The cervical lesions were ring-enhanced after the administration of gadolinium dimeglumine (B, arrows). In the MRI performed 4 months later, T2 hyperintense lesions extended all levels of the cervical spinal cord (C) and the number of ring-enhancing lesions increased (D, arrows). (E–I) Pathological findings of spinal cord biopsy. (H, E) stain revealed uniform atypical cells with microvascular proliferation (E). Immunohistochemistry of the tumor was positive for GFAP (F) and H3K27 M (G), with no loss of H3K27me3 detected (H). Tumor cells were also positive for AQP4 (I). Bars: 50 µm. AQP4; aquaporin 4, GFAP; Glial fibrillary acidic protein, H&E; Hematoxylin & Eosin, MRI; magnetic resonance imaging
Given the atypical clinical course of the presumed diagnosis of NMOSD, a spinal cord biopsy was performed. Hematoxylin and eosin staining revealed tumor cells with microvascular proliferation (Figure 1E). Immunohistochemistry staining was positive for glial fibrillary acidic protein (GFAP) and H3K27 M (Figure 1F and G), and negative for isocitrate dehydrogenase 1 (IDH1) and H3K27me3 loss (Figure 1H), consistent with high-grade glioma with H3K27 M mutation. Interestingly, staining against AQP4 was positive on the tumor cells (Figure 1I). The patient received radiation treatment and chemotherapy with bevacizumab and temozolomide against high-grade glioma. Subsequently, an MRI revealed improvement in the spinal cord swelling and diminished lesion enhancement. Serum AQP4-Ab levels measured using CBA turned negative.
Discussion
Clinical Features of Cases With Non-Demyelinating Disorders, Presenting Positive Anti-Aquaporin-4 Antibodies Measured Using CBA
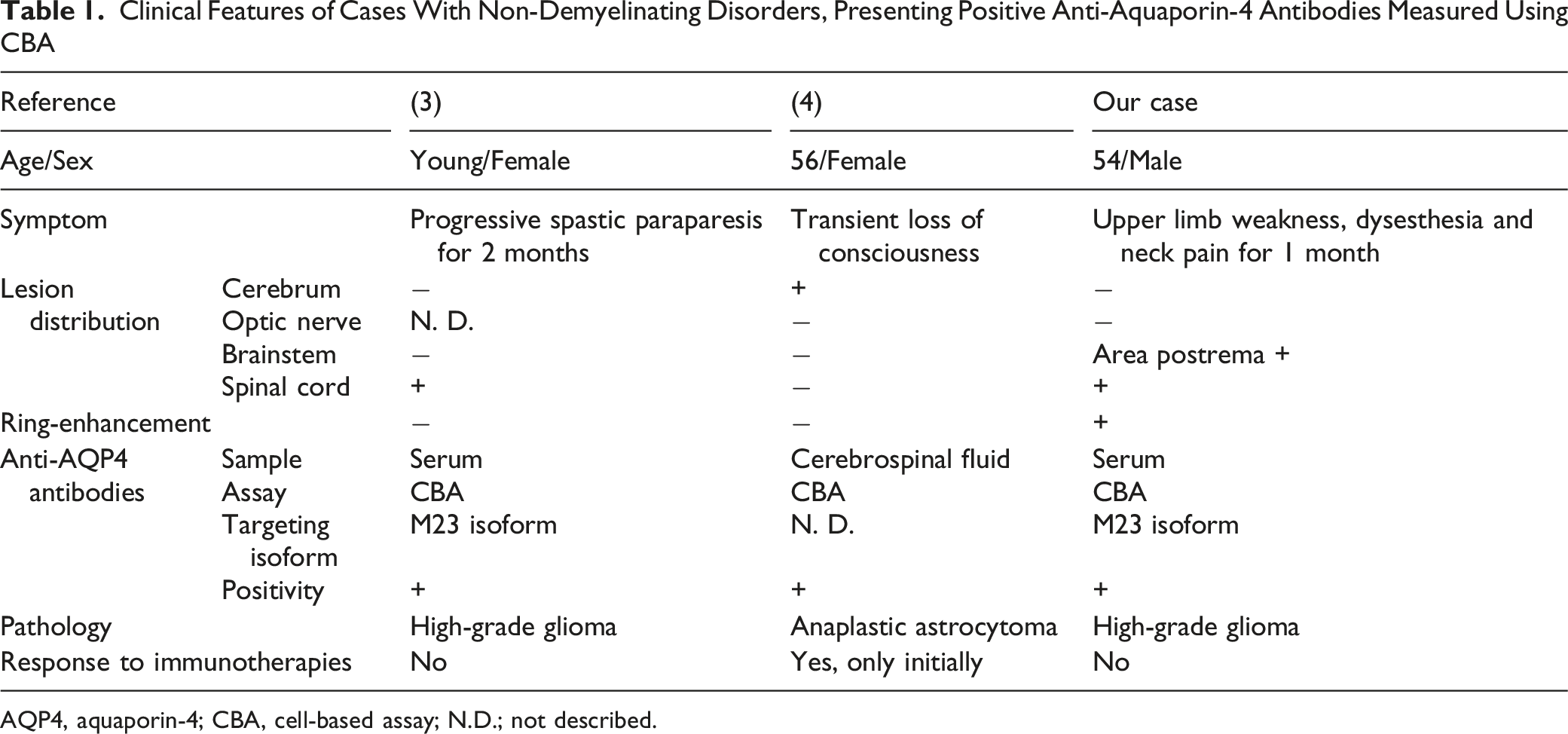
AQP4, aquaporin-4; CBA, cell-based assay; N.D.; not described.
In the pathogenesis of glioma, AQP4 is reportedly overexpressed in the tumor cells, contributing to tumor cell invasion and cerebral edema. 7 This overexpression could potentially promote the production of AQP4-Ab. We hypothesize that the disruption of the blood-brain barrier, indicated by microvascular proliferation in tumor tissue, 8 might expose AQP4 to the peripheral blood, contributing to the production of AQP4-Ab. Further studies are needed to investigate the frequency of AQP4-Ab positivity and the mechanisms of autoantibody production in patients with glioma.
Of note, although immunohistochemistry was positive for H3K27 M in our case, H3K27me3 expression was retained. Therefore, the diagnosis did not strictly fulfill the criteria for diffuse midline glioma, H3K27-altered, defined in the 2021 WHO classification. 9 One possible explanation is that the expression level of mutant H3K27 M protein may have been insufficient to fully inhibit the Polycomb Repressive Complex 2 (PRC2), resulting in preserved H3K27me3.
In conclusion, we present a case of spinal cord glioma with AQP4-Ab positivity, suggesting tumor-triggered antibody production. Physicians should be aware that glioma patients may present with AQP4-Ab positivity.
Footnotes
Acknowledgements
Ethical Considerations
This case report describes a non-interventional observation and did not require ethical approval.
Consent for Publication
Informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Author Contributions
S.T.: Conceptualization, Investigation, Data Collection, Writing - original draft. M.S.: Writing - Review & Editing. T.I.: Writing - Review & Editing. J.K.: Pathological investigation. H.S.: Pathological investigation. M.I.: Surgical investigation. Y.N.: Conceptualization, Writing - Review & Editing, Supervision. T.Y.: Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized data not published within this article will be made available by request from any qualified investigator.