
Abstract
Background and Purpose
Substance use is rising among young adults with stroke. We aimed to assess the prevalence of substance use, and the use of toxicology screening in the diagnostic evaluation, for young individuals with acute ischemic stroke (AIS) at a single comprehensive stroke center.
Methods
This retrospective study was conducted at a single comprehensive stroke center in individuals ages 18 to 55 years old with AIS from 2020-24. Cases of AIS and recent substance use, or the use of cocaine, methamphetamine, marijuana, opioids, or other illicit substances within 30 days of admission, were compared to those with AIS and no substance use. Descriptive statistics and least absolute shrinkage and selection operator (LASSO) modeling were completed to evaluate predictors of toxicology screening.
Results
Of 425 encounters screened, 307 were eligible for inclusion. Recent substance use was documented in 21.5% of encounters. Individuals with recent substance use were younger (median age 46 vs 51 years old in controls). Toxicology screens were ordered for 29.3% of all encounters, and in 27.9% of cryptogenic strokes. Models did not identify a variable that predicted the performance of toxicology screening.
Conclusions
Recent substance use was documented in about 1 in 5 young individuals with AIS. Further research is needed to understand the relationship between AIS and substance use, and the appropriate use of toxicology screening in stroke care.
Introduction
Stroke and substance use are both major public health concerns, however our knowledge about their intersectionality remains limited. Substance use (cocaine, marijuana, methamphetamine, opioids, and other illicit substances) contributes to stroke development through various mechanisms.1-4 Even when substance use is solely comorbid with stroke, the negative health impacts and excess mortality associated with substance use highlight the need for additional study.5,6 Up to 1 in 4 young adults with stroke have comorbid substance use, and this appears to be increasing over time.7,8
Routine toxicology screening is not guideline-recommended in the diagnostic evaluation of stroke. 9 Previous research estimates 32 to 40% of individuals with stroke undergo toxicology screening. Black race, younger age, and documented substance use in the medical record have been associated with toxicology screening.8,10
The aims of this study were to assess the prevalence of identified substance use and use of toxicology screening in young individuals with acute ischemic stroke (AIS) in a single comprehensive stroke center.
Methods
Study Population and Design
This observational study adhered to the STROBE guidelines for observational studies. Local institutional review board approval was obtained. An encounter list for AIS was generated based on ICD-10 codes from an institutional database from January 2020 to June 2024. The study group included consecutive admissions to the primary stroke service for individuals with initial or recurrent AIS, ages 18 to 55 years old at the time of admission. Individuals with diagnoses of transient ischemic attack, or acute or remote central nervous system hemorrhage were excluded. The ischemic stroke mechanism was captured when documented in the medical record, utilizing the Trial of Org 10172 in Acute Stroke Treatment categorization of stroke mechanism, but also including the option for multiple or competing mechanisms as per institutional practice. 11 We also distinguished those with no identified etiology despite a complete standard diagnostic evaluation as cryptogenic. Information was abstracted from the medical record by author E.F.
Recent substance use was defined as use of cocaine, methamphetamine, marijuana, opioids, or other illicit substances within 30 days of admission. History of remote substance use was also collected when available. We categorized the method in which substance use was identified, including: patient/surrogate report, chart review, and/or toxicology screen positivity. Toxicology testing was performed via urine drug screen (UDS) immunoassay. The UDS used included the following substances with defined cut-off values: amphetamines
Statistical Analysis
Cases of AIS with recent substance use were compared to controls, or those with AIS without recent substance use. Descriptive statistics were conducted on demographic and clinical information. Least absolute shrinkage and selection operator (LASSO) modeling, a form of multivariable logistic regression, was completed to evaluate if any demographic or clinical variables, including age, sex, race, ethnicity, stroke number (initial or recurrent), hypertension (HTN), hyperlipidemia (HLD), diabetes mellitus (DM), and atrial fibrillation (AF), were associated with a toxicology screen being ordered. The LASSO model was selected over a traditional multivariable logistic regression due its agnostic, data-driven approach to find the strongest predictors. The LASSO model was trained on a random selection of 80% of encounters and tested on the remaining 20%. LASSO model performance was optimized using the area-under-the-curve (AUC) statistic for ordering a drug screen. For the LASSO model to be considered to have utility, the model must outperform the No Information Rate metric (P < 0.05) in the testing set.
Results
Screening was performed on 425 encounters (Figure 1). Individuals were excluded if admission was not to the primary stroke service (n, 100), admission was not for AIS (n, 12), there was a history of CNS hemorrhage (n, 3), or the individual did not meet age criteria (n, 1). Two duplicate entries in the database were identified during screening as well. The study group included 290 individuals in 307 encounters, with 17 individuals admitted twice within the study period. Flow of eligibility for inclusion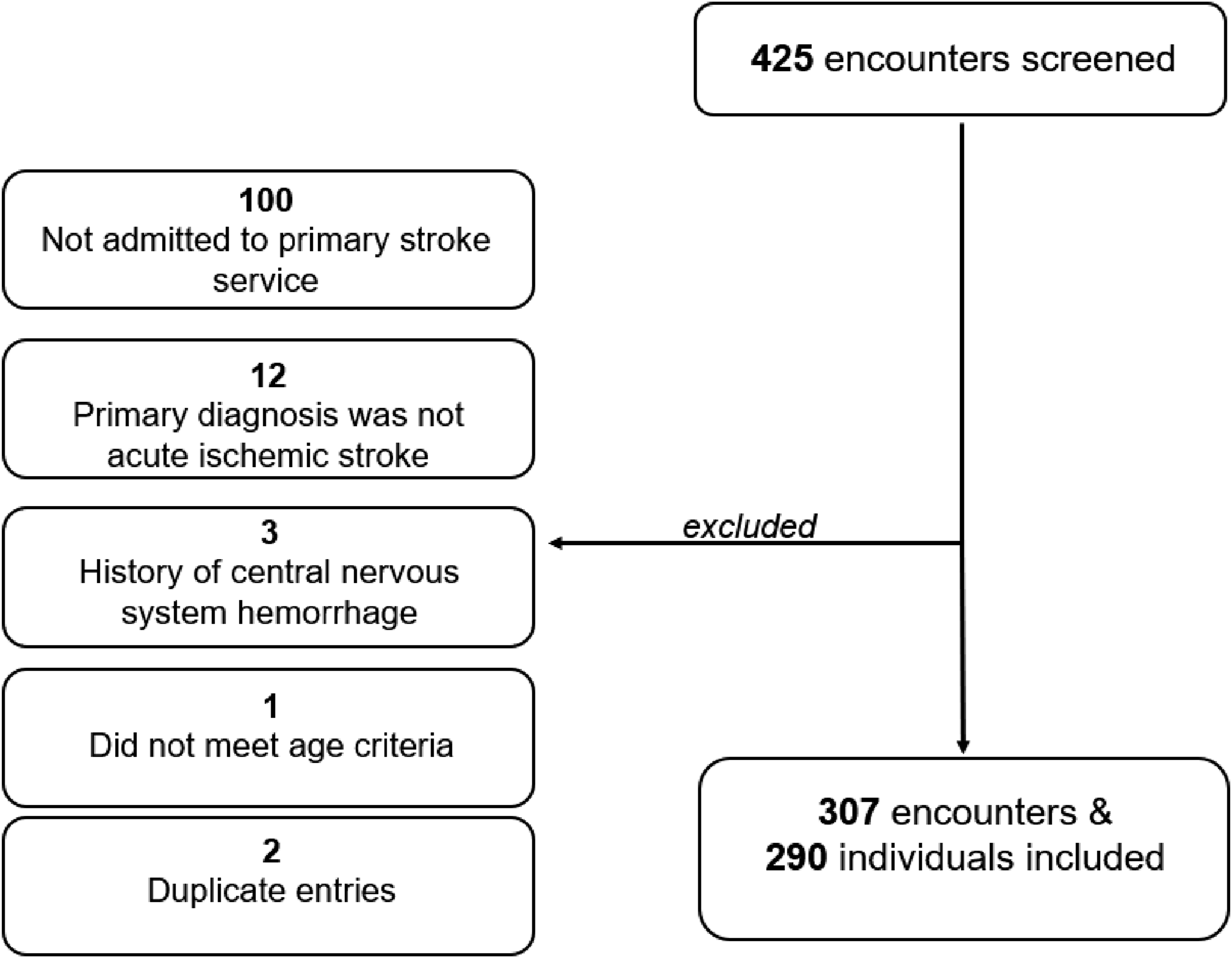
Demographic and Clinical Characteristics of Young Individuals With Acute Ischemic Stroke
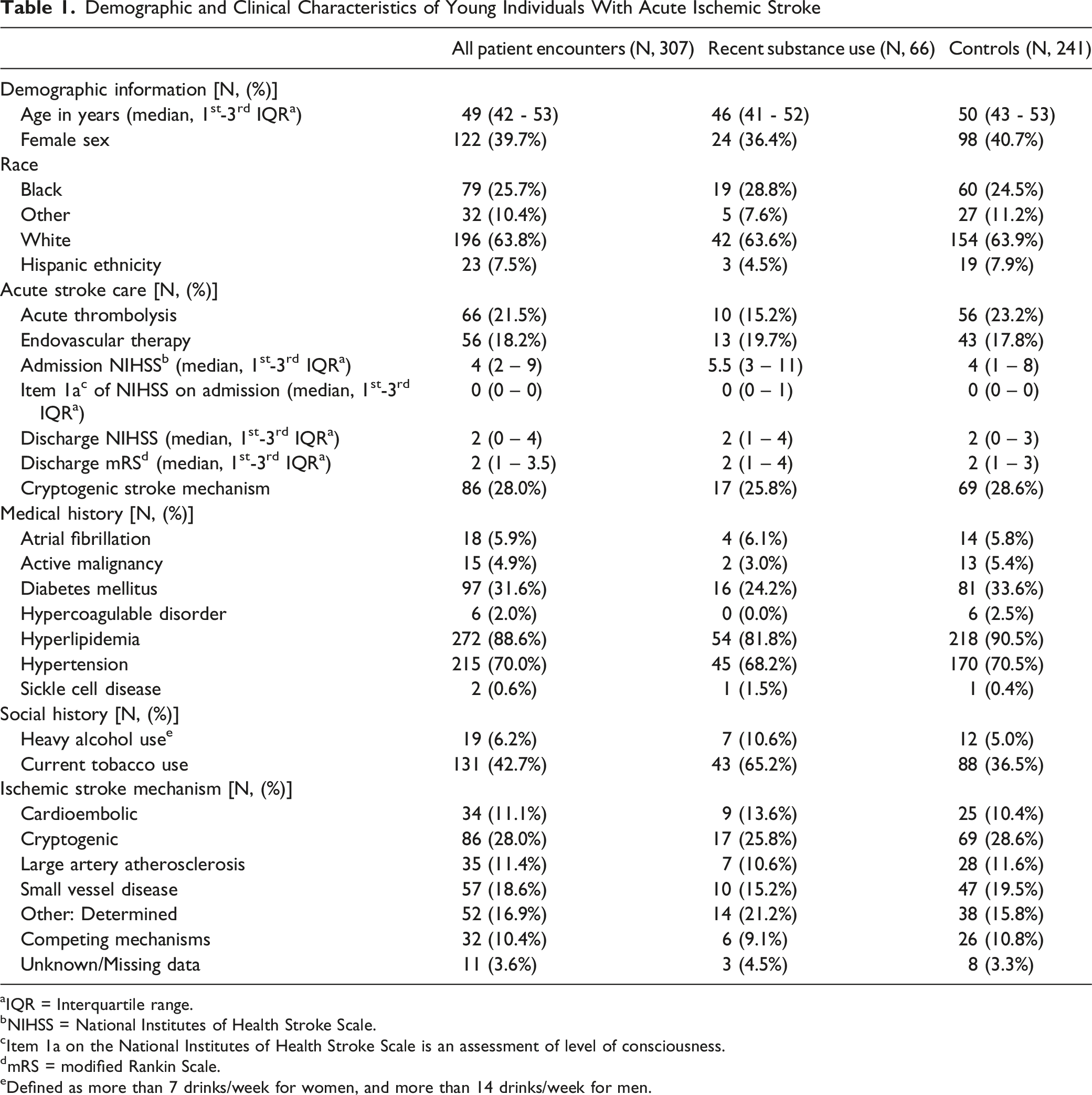
aIQR = Interquartile range.
bNIHSS = National Institutes of Health Stroke Scale.
cItem 1a on the National Institutes of Health Stroke Scale is an assessment of level of consciousness.
dmRS = modified Rankin Scale.
eDefined as more than 7 drinks/week for women, and more than 14 drinks/week for men.
Details of Identified Substance Use
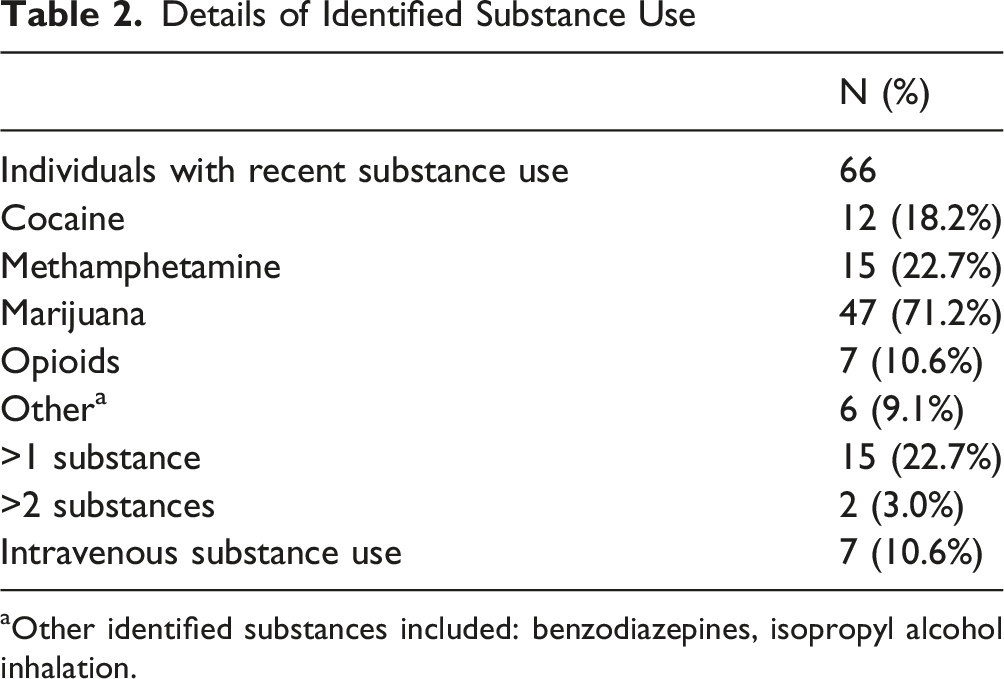
aOther identified substances included: benzodiazepines, isopropyl alcohol inhalation.
Cryptogenic Stroke Diagnostic Evaluations

Toxicology screens were ordered in 29.3% of all encounters (90 of 307), less often in initial compared to recurrent AIS (24.4% vs 33.3%). In cryptogenic stroke, the frequency of toxicology screening was similar for those with or without recent substance use (25.8% vs 28.6%).
LASSO regression resulted in non-zero beta coefficients for age (−0.04), stroke number (0.67), HLD (−0.78), DM (−0.58), and AF (0.84) for predicting ordering a toxicology screen. The AUC decreases from ordering (0.70) a drug screen to 0.65 in the testing set. While the model has an AUC greater than chance (0.5), it did not achieve greater accuracy over the No Information Rate of 0.71 (P = 0.668).
Discussion
In this study of young adults with AIS, substance use in the 30 days prior to admission was noted in about 1 in 5 individuals (21.5%), similar to prior research. 8 Toxicology screening was completed slightly less often (29.3%) compared to prior research.8,10 Of note, other studies have included additional diagnoses such as intracerebral hemorrhage, subarachnoid hemorrhage, and transient ischemic attack, and there is likely heterogeneity regarding both the suspicion for substance use and prevalence of substance use among these stoke subtypes. Advanced modeling did not detect a demographic or clinical factor associated with a toxicology screen being ordered in our study, unlike other studies.8,10
Evaluating the method of substance use detection, recent substance use was typically identified by multiple means. However, 1 in 5 of those with recent substance use were only identified by positive toxicology results. The American Heart Association guidelines for secondary stroke prevention suggest that in those with cryptogenic stroke, tests for drug use are reasonable to perform as clinically indicated. 9 This guideline about toxicology screening for cryptogenic stroke could plausibly lead to more frequent screening being done compared to other ischemic stroke mechanisms, however, this was not observed in our population. Our results likely reflect the ongoing heterogeneity among emergency medicine and stroke physicians regarding the relevance of toxicology testing. Presently, the best practice for utilization of toxicology screening in the evaluation for stroke remains unknown. Further research focused on the significance of toxicologic exposures in stroke, regarding risk factors, clinical care, and outcomes, is warranted to guide our clinical practices regarding screening. The rapidly changing landscape regarding marijuana legalization in many states within the United States will likely influence both the prevalence of marijuana use and the frequency of toxicology testing.
The strengths of this work include a clear definition and comprehensive capture of substance use from the medical record. This included pertinent sub-categorizations of frequently used substances in the stroke population, a specification of the time of use relative to presentation to care (30 days or less), and notation of the identification method (patient interview, chart history, and/or toxicology screens). There are limitations to this work. First, by the nature of the retrospective design, there is an inherent incomplete capture of the prevalence of substance use. Second, only when a toxicology screen was positive, confirmatory testing was utilized with gas chromatography-mass spectrometry (GC-MS), though there remains a risk of false positives. 13 Third, this is a focused study of young individuals with ischemic stroke cared for by a dedicated stroke service at a single comprehensive stroke center. Our results are therefore not readily generalizable but should prompt additional study of this topic in a large, multicenter population.
In summary, our study highlights a high prevalence of substance use among young adults with acute ischemic stroke, noted in about 20% of the study group. Studying the relationship between substance use and stroke is challenging, due to limited documentation in the medical record and variable screening practices. As most research on substance use and stroke is observational, future research with prospective study would enhance our knowledge substantially. Additional research is needed on the prevalence and significance of substance use in stroke patients to inform best practices in overall care, and to support equitable practices in toxicology screening.
Footnotes
Ethical Considerations
Local institutional review board approval was obtained (University of Virginia IRB-HSR:300048).
Consent to Participate
Not applicable as this was a retrospective, chart-based review.
Author Contributions
Emily Fisher (corresponding author) is responsible for study design, data collection, assistance with the statistical analysis, and manuscript writing and editing. Chad Aldrige is responsible for study design, statistical analysis, and manuscript editing. Rohini Bhole is responsible for manuscript editing. Bradford Worrall is responsible for study design and manuscript editing. Christopher Holstege is responsible for study design and manuscript editing. Nassima Ait-Daoud Tiouririne is responsible for study design and manuscript editing. Karen Johnston is responsible for study design and manuscript editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized data will be shared with qualified investigators upon request.