
Abstract
A previously healthy 35-year-old woman in her third trimester of pregnancy presented with 2 weeks of progressive cognitive dysfunction, behavioral changes, and headache. Neurological examination was nonfocal, without evidence of meningeal irritation. Brain MRI showed multifocal punctate diffusion-restricting lesions in the subcortical white matter. The etiology was initially unclear despite extensive testing, Several days later, the patient presented again with worsening symptoms and interval radiographic progression. Ultimately, the constellation of clinical features and diagnostic findings suggested a unifying diagnosis. We discuss her clinical course and highlight the diagnostic reasoning. This case emphasizes the importance of maintaining a broad differential diagnosis and integrating evolving clinical and radiographic features, while balancing pregnancy-specific diagnostic and therapeutic considerations, in the evaluation of subacute encephalopathy.
Case Presentation Section 1
A previously healthy right-handed 35-year-old pregnant woman at 27 weeks of gestation presented to an outside hospital with 2 weeks of confusion, imbalance, nausea, and vomiting. Family members reported personality changes, impaired short-term memory, and new-onset headaches that had worsened over the preceding 5 days. She had difficulty performing previously routine tasks, such as arranging vehicles in her driveway. She denied focal weakness, sensory deficits, episodic loss of consciousness, or involuntary convulsions. Examination showed word-finding difficulty and impaired delayed recall, but no motor deficits, sensory changes, or incoordination. No evidence of meningeal irritation was appreciated. 1. What is the differential diagnosis of subacute progressive encephalopathy in a pregnant woman? 2. What initial testing (labs, imaging, or procedures) should be considered?
Case Presentation Section 2
The patient’s symptoms suggested widespread cortical dysfunction with a broad differential diagnosis encompassing metabolic derangements, infectious or autoimmune meningoencephalitis, multifocal ischemic stroke, drug intoxication, nutrient deficiencies, and nonconvulsive seizures. Pregnancy-related etiologies of encephalopathy to consider include posterior reversible encephalopathy syndrome (PRES, occasionally associated with the syndrome of hemolysis, elevated liver enzymes, and low platelets [HELLP]), thrombotic thrombocytopenic purpura (TTP), dural venous sinus thrombosis, reversible cerebral vasoconstriction syndrome, mitochondrial disorders, urea cycle defects, and Wernicke encephalopathy in cases of hyperemesis gravidarum. Idiopathic intracranial hypertension should be considered in pregnant patients presenting with new-onset headaches, although this condition is not associated with encephalopathy.
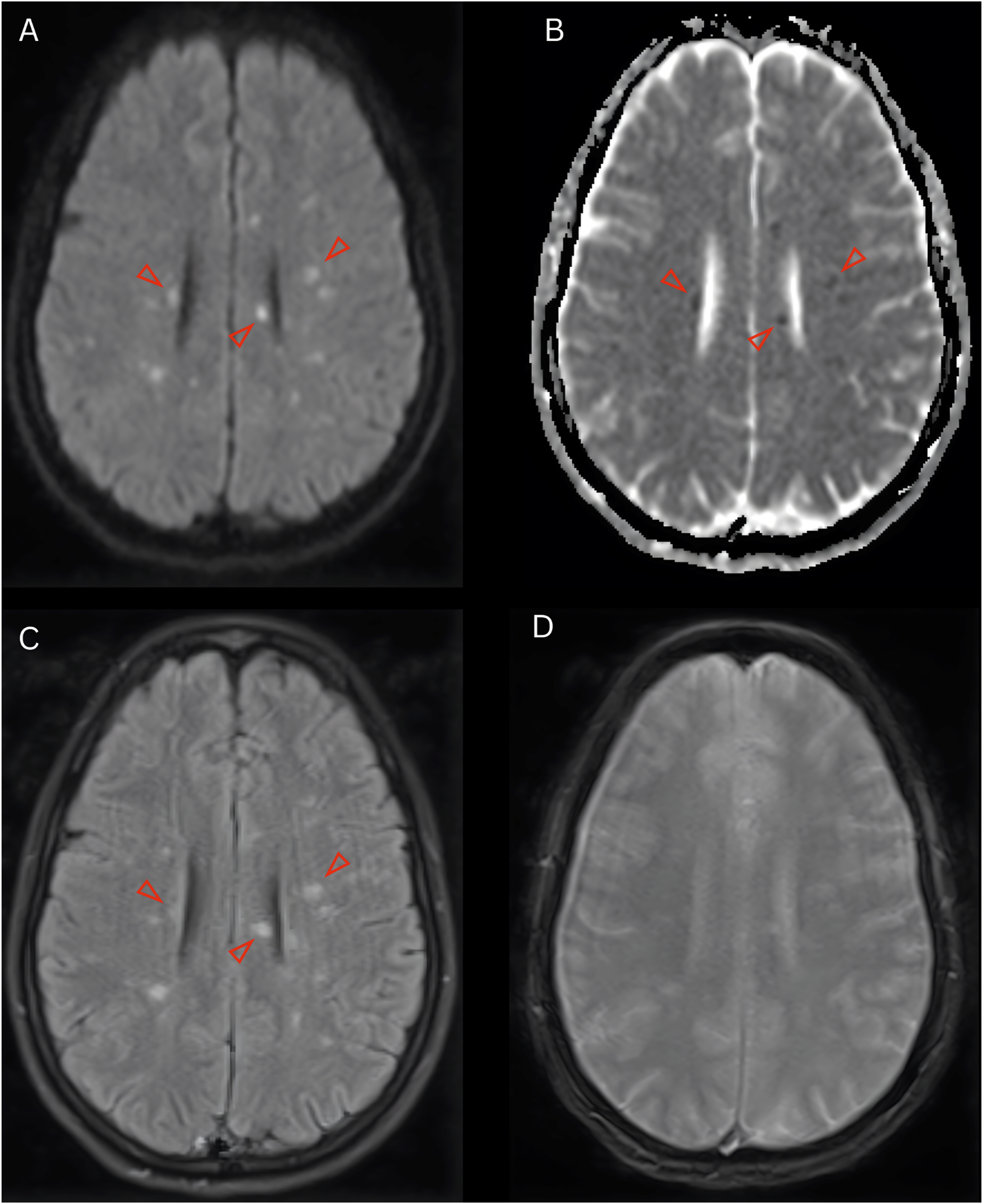
On presentation, the patient was afebrile and normotensive. Complete blood count was remarkable for platelets of 64,000/μL. Subsequent hemolysis studies, including peripheral smear, lactate dehydrogenase, and haptoglobin, were normal. Peripheral blood smear revealed no abnormalities. Based on these results, the patient was suspected of having gestational thrombocytopenia. Comprehensive metabolic panel, thyroid-stimulating hormone, and urine drug screen were unremarkable. Lactic acid was not elevated. B12 was low at 158 pg/mL with a normal methylmalonic acid level. Noncontrast MRI of the brain identified innumerable punctate T2 hyperintense lesions with restricted diffusion in the bilateral subcortical cerebral white matter and basal ganglia (Figure 1) 1. Given the findings on MRI, what are the most likely stroke etiologies? Initial noncontrast MRI of the brain. (A) Axial diffusion-weighted imaging and; (B) apparent diffusion coefficient demonstrated innumerable punctate foci of diffusion restriction within the bilateral subcortical cerebral white matter; (C) The lesions were hyperintense on fluid-attenuated inversion recovery images; (D) No microhemorrhages were identified on gradient echo
Case Presentation Section 3
This multifocal infarct pattern shifted diagnostic consideration toward embolic, hypercoagulable, or inflammatory etiologies. Magnetic resonance angiography (MRA) without contrast revealed patent intracranial large vessels (Figure 2). Transthoracic echocardiography showed a preserved ejection fraction without a patent foramen ovale. There were no hemodynamically significant valvular abnormalities or vegetations. Carotid artery ultrasound demonstrated no significant stenosis of the bilateral carotid or vertebral arteries. Bilateral lower extremity ultrasound was negative for deep venous thrombosis. Laboratory markers of vascular risk factors, including lipid panel and hemoglobin A1c, were normal. A hypercoagulable evaluation, including antithrombin III, protein C and S, β2-glycoprotein I antibodies, lupus anticoagulant, and anticardiolipin antibodies, was unremarkable. Noncontrast MRA of the head showed patent intracranial large vessels
Electroencephalography showed diffuse slowing consistent with encephalopathy; no epileptiform discharges were identified. Lumbar puncture revealed an opening pressure of 14 cmH2O, elevated protein of 87.5 mg/dL, normal glucose of 80 mg/dL (serum glucose of 122 mg/dL), and no pleocytosis or erythrocytosis. Cerebrospinal fluid (CSF) gram stain, culture, meningitis/encephalitis panel, IgG index, and oligoclonal bands were negative. 1. Based on these findings, how has the differential diagnosis changed? 2. If symptoms worsen, what further diagnostic tests should be considered?
Case Presentation Section 4
These findings narrowed the differential diagnosis. Metabolic, toxic, and nutritional etiologies were deprioritized given the MRI findings of multifocal diffusion-restricting lesions involving both white and deep gray matter structures. Infectious meningoencephalitis became less plausible in the absence of CSF pleocytosis and a negative infectious panel. PRES and dural venous sinus thrombosis were considered but not supported by normotension and imaging inconsistent with a venous infarction pattern, respectively. HELLP syndrome was considered improbable due to the absence of hemolysis and transaminitis, while TTP was similarly unsupported in the setting of a normal peripheral blood smear without evidence of hemolysis. Although routine stroke investigations were nondiagnostic, a paroxysmal cardioembolic source could not be excluded. Long-term cardiac monitoring was planned. Concern remained for an inflammatory process, with cerebral angiography reserved for clinical deterioration.
Three days later, the patient presented to our institution with worsening encephalopathy and new-onset dysarthria. Family described prominent nocturnal restlessness and increasingly fluctuating mentation, occasionally rendering her unable to answer simple questions. On examination, the patient was oriented to self, city, and place but not year; she followed two-step commands but could not complete a Luria sequence. No other focal neurological deficits were identified.
MRI of the brain demonstrated new diffusion-restricting lesions within the supraventricular white matter involving the body and splenium of the corpus callosum (Figure 3A), as well as a punctate focus at the base of the left cerebral peduncle. The following morning, she developed a new internuclear ophthalmoplegia. Repeat MRI revealed additional diffusion-restricting lesions in the left pons (Figure 3B) and left parietal lobe. Repeat noncontrast MRI of the brain obtained following clinical deterioration showed (A) new diffusion-restricting lesions in the genu and splenium of the corpus callosum and; (B) new left pontine lesions on diffusion-weighted imaging; (C) Follow-up MRI of the brain 4 weeks later showed interval improvement in diffusion-restricting lesions on diffusion-weighted imaging; (D) Sagittal fluid-attenuated inversion recovery images demonstrated persistent “snowball lesions” in the corpus callosum characteristic of Susac syndrome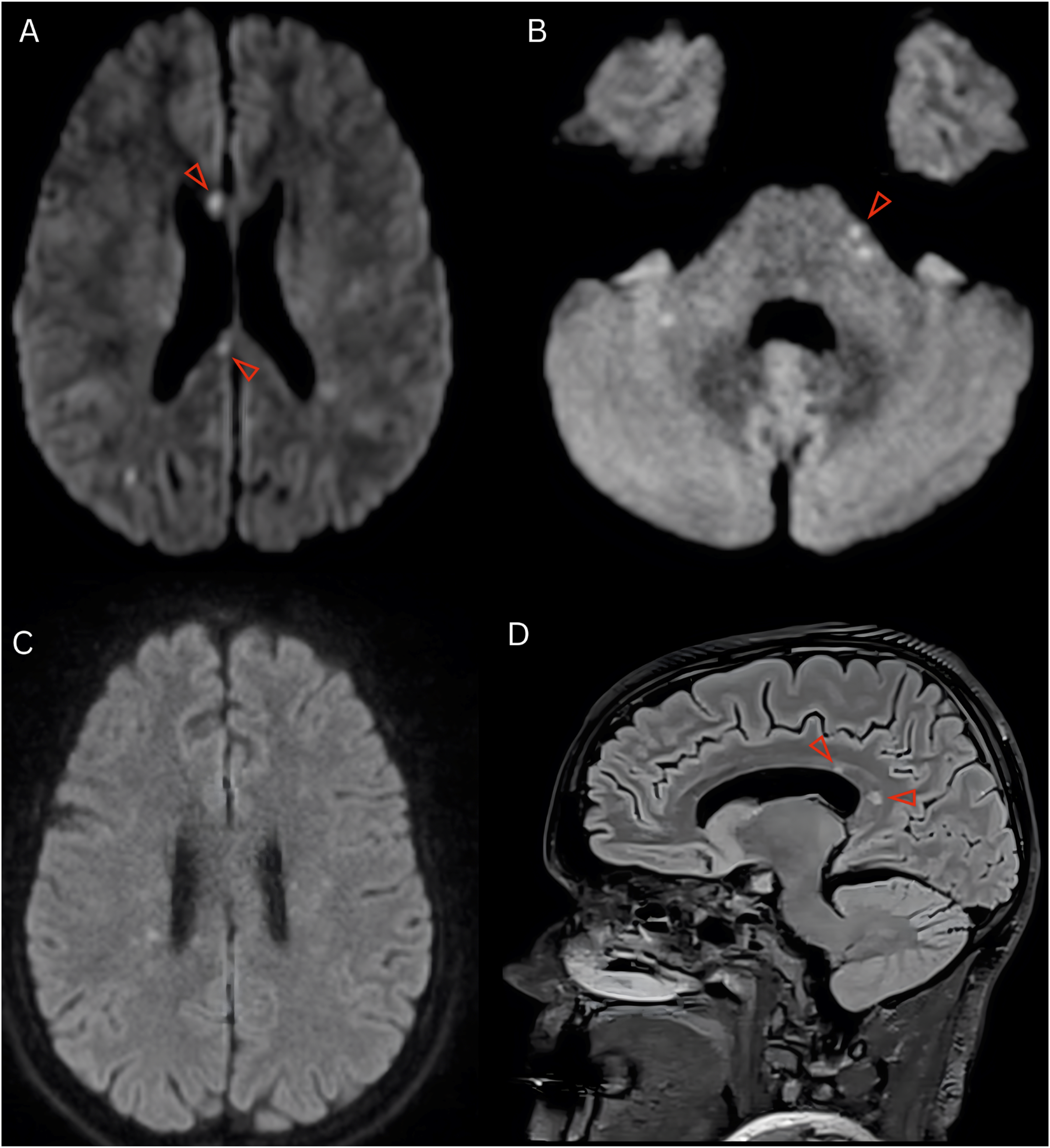
Considering the prior negative workup for embolism and hypercoagulable disorders, the clinical picture became increasingly concerning for an inflammatory vasculopathy. Empiric treatment with high-dose intravenous methylprednisolone at 1000 mg daily for 5 days was initiated. Repeat MRA head without contrast was normal. Serological investigations of systemic vasculitis were negative and included antineutrophil cytoplasmic antibodies, antinuclear antibodies, extractable nuclear antigen panel, anti-Sjogren’s syndrome-related antigen, complement levels, erythrocyte sedimentation rate, C-reactive protein, HIV antibodies, Lyme antibodies, and treponemal IgG. A diagnosis of primary central nervous system (CNS) vasculitis was considered. Subsequent cerebral angiography was normal without evidence of vasculitis. There was brief discussion of a brain biopsy to definitively exclude a small vessel vasculitis.
However, new lesions in the corpus callosum, and additional historical details elicited from the patient, raised an alternative possibility. The patient reported recent treatment for a presumed ear infection characterized by bilateral aural fullness, left greater than right, and tinnitus. She also endorsed episodic blurred vision in the left eye several weeks prior, but no overt vision loss. An inpatient dilated fundoscopic examination revealed a few peripheral sclerotic vessels bilaterally. Definitive visualization via fluorescein angiography was contraindicated due to pregnancy; however, spectral-domain optical coherence tomography (SD-OCT) visualized no retinal abnormalities. Audiologic evaluation demonstrated severe low-frequency sensorineural hearing loss in the left ear and moderate low-frequency sensorineural hearing loss in the right ear. 1. What is the most likely diagnosis? 2. How should this condition be treated?
Case Presentation Section 5
The constellation of clinical, radiographic, and audiologic findings were highly suggestive of Susac syndrome. Brain biopsy was deferred, and the patient was ultimately treated with intravenous immunoglobulin (IVIG) 2 g/kg administered over 5 days.
At discharge, the patient’s cognitive, auditory, and visual symptoms had improved. She was discharged with a prolonged corticosteroid taper and plans to initiate rituximab following delivery. Repeat MRI brain 4 weeks later showed interval improvement in diffusion restricting lesions with residual corpus callosum lesions (Figure 3C–D). Coordination with maternal-fetal medicine regarding the timing of delivery and post-partum management is ongoing.
Discussion
Susac syndrome is a rare, autoimmune endotheliopathy characterized by microvascular occlusions within the brain, inner ear, and retina. The ensuing microinfarctions are responsible for the classic clinical triad of encephalopathy, sensorineural hearing loss, and branch retinal artery occlusions (BRAOs). Symptoms may manifest simultaneously at disease onset but more commonly emerge sequentially over the course of weeks or months, thereby obscuring early diagnosis. 1 Both encephalopathic (as in the present patient) and recurrent BRAO disease phenotypes have been described, with the former considered more severe and meriting aggressive management. 2
Characteristic MRI findings include multifocal, small, diffusion-restricting T2 hyperintense lesions in the supraventricular white matter, which may also involve the deep gray nuclei, brainstem, and cerebellar peduncles. 3 Callosal lesions, a radiographic hallmark of the disorder, may appear well-demarcated and spherical (termed “snowball” lesions). 4 Leptomeningeal enhancement is common. In the present patient, MRI demonstrated multiple diffusion-restricting T2 hyperintense lesions involving the pons, basal ganglia, corpus callosum, and subcortical white matter, with interval progression on serial imaging.
Criteria have been proposed and revised to improve the sensitivity and specificity of diagnosis.1,5 Our patient had probable Susac syndrome, with unequivocal clinical or paraclinical involvement of 2 of the 3 classically affected organs. Despite her subjective visual symptoms, fluorescein angiography to definitively assess for branch retinal artery occlusions could not be safely performed during pregnancy. However, SD-OCT, posited as a complementary tool for the detection of retinal ischemia in Susac syndrome, 6 demonstrated no evidence of abnormalities.
The literature regarding Susac syndrome is predominantly comprised of case reports and small series.3,6,7 Accordingly, epidemiologic data for this condition remain incomplete, although studies have estimated an annual incidence of 0.024 to 1.3 per 100,000 people.3,8 Clinical manifestations typically arise in the third or fourth decades of life and more commonly in women. 8 The relationship between Susac syndrome and pregnancy remains poorly understood. 7 Pregnancy has been posited as a risk factor for relapse, with hormonal fluctuations potentially playing a role in disease pathogenesis. Indeed, there is a relatively large number of cases diagnosed in the intrapartum or postpartum period. 9 However, prior observational data may be confounded by publication bias, and the lack of expansive, systematic registries may result in underreporting of cases among patients in remission and without adverse outcomes during pregnancy. 9 Further work is needed to clarify the pathophysiological mechanisms underlying the relapse and remission of the disease.
One of the principal differential diagnoses of Susac syndrome is primary CNS vasculitis. While the negative cerebral angiogram reduced suspicion for a large- or medium-vessel vasculitis, a small-vessel vasculitis could not be definitively excluded given the limited resolution of angiography. 10 However, involvement of the corpus callosum and absence of microhemorrhages are both uncommon in primary CNS vasculitis, prompting reconsideration of alternative diagnoses.11,12 Moreover, the presence of central corpus callosal “snowball” lesions is highly suggestive of Susac syndrome. 4
Immunomodulation is the mainstay of therapy, with choice of treatment predicated on disease severity.1,13 First-line acute treatment is comprised of high-dose intravenous methylprednisolone, IVIG, and/or plasma exchange. A prolonged corticosteroid taper over months and/or maintenance IVIG are often utilized to prevent relapses. Oral agents, such as mycophenolate mofetil and azathioprine, may be employed, although it generally takes months to exert their full immunosuppressant properties. In cases of severe or refractory disease, intravenous pulse cyclophosphamide or rituximab may be used. Pregnancy precludes most of these medications. 9 Therefore, we elected to treat with high-dose IV corticosteroids followed by a 5-day course of IVIG, 14 both of which were well-tolerated by the patient. Rituximab is planned for long-term immunotherapy following delivery because it is considered relatively safe while breastfeeding. 15
This case highlights the diagnostic and therapeutic challenges of Susac syndrome during pregnancy, where standard evaluation and immunosuppressive regimens may be constrained. Multidisciplinary discussion and careful postpartum planning will be necessary to guide definitive management and reduce risk of disease progression or relapse.
Footnotes
Ethical Considerations
Consent to publish was obtained from the patient. IRB approval was not required, and ethical guidelines as outlined in the Declaration of Helsinki were followed.
Author Contributions
All authors contributed to the conception and design of the article; drafting of the paper; revising it critically for intellectual content; the final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.