
Abstract

Oropouche virus (OROV) is an arthropod-borne orthobunyavirus in the family Peribunyaviridae. First identified in 1955 in Trinidad and Tobago, the primary vector is the biting midge Culicoides paraensis with additional mosquito vectors including Culex, Aedes, and Coquillettidia species. There are 2 recognized transmission cycles: the sylvatic cycle, where the virus circulates in wildlife and vector insects, and the urban cycle, where humans serve as amplifying hosts.1,2 Historically, OROV has been documented in Central and South America and the Caribbean.3,4
Multiple outbreaks have occurred in the past decade, including newly affected regions, such as Cuba, with over 10 000 cases reported in 2024. 5 Increased urbanization and expanding ecological niches contribute to rising cases.1,5 Its burden is likely underestimated due to limited testing availability and frequent misclassification as dengue, chikungunya, or Zika infections.5,6 In 2024, one-hundred ten travel-associated OROV cases were reported in the United States, including 2 neuroinvasive cases. 3
The incubation period is typically 3-10 days. Symptoms usually begin with abrupt onset of fever, headache, chills, and myalgia.4,6,7 Photophobia, dizziness, nausea, vomiting, and maculopapular rash can occur. Gastrointestinal involvement or hemorrhagic events such as epistaxis and petechiae are rare.6,7 Acute illness generally lasts 2-7 days, followed by a post-acute phase with prolonged fatigue and malaise.1,7
Neuroinvasive disease is reported in 4-5% of OROV infections. Recent data suggests neurologic involvement may be more frequent and heterogeneous than previously reported. Neurologic manifestations occur during both the acute phase and the post-infectious phase, ranging from headache to frank meningoencephalitis. 5
The most common neurologic symptom is severe, persistent, retro-orbital headache with photophobia, present in nearly 90% of cases. However, headache in this context is most likely a manifestation of systemic febrile illness rather than evidence of CNS invasion. Central nervous system involvement may present with meningoencephalitic features including confusion, altered consciousness, neck stiffness, dizziness or vertigo, nystagmus, diplopia, dysgeusia, and hearing loss. Both generalized and focal seizures have been reported. Cranial neuropathies and persistent neurologic deficits, including residual extremity weakness have been described. 5
Neuroimaging may be normal but can demonstrate focal cortical lesions on magnetic resonance imaging or computed tomography. Electroencephalography may show focal slowing. Cerebrospinal fluid (CSF) analysis typically reveals a lymphocytic pleocytosis, elevated protein and normal glucose in meningoencephalitis. Cytoalbuminologic dissociation has been reported in post-infectious neuropathies.3,5
Delayed immune-mediated neurologic syndromes have been documented. Guillain–Barré syndrome (GBS), specifically an acute axonal motor neuropathy phenotype, can develop approximately 10 days after laboratory-confirmed acute OROV infection. Electromyography and nerve conduction studies demonstrated acute axonal motor neuropathy 5
Vertical transmission risk is under investigation. Brazilian reports suggest placental infection and adverse pregnancy outcomes, including fetal death, miscarriage, and congenital anomalies such as microcephaly. 4 Miscarriages in infected women have been reported in the first and third trimester of gestation. In such cases, serial ultrasounds and close monitoring are recommended. Similar to Zika virus, pregnant women should be advised to avoid areas with known OROV circulation if able.4,5
Diagnosis initially relies on reverse transcription-polymerase chain reaction (RT-PCR) for viral nucleic acid detection in blood, serum, or tissue.1,7 Serologic assays become useful after the first week, with IgM appearing late in week 1 and IgG appearing subsequently, with neutralizing antibody titers demonstrating ≥4-fold rise between acute and convalescent specimens. In neuroinvasive disease, viral nucleic acid may be absent in CSF because of low viral loads, but OROV-specific IgM and/or neutralizing antibodies can often be detected about a week after onset.3,8 Formal CSF:serum antibody index calculations have not been systematically reported in OROV literature to date.
There are currently no specific antiviral therapies or vaccines for OROV infection.1,7 Post-OROV GBS can be treated with intravenous immunoglobulin or plasma exchange. Otherwise, treatment is supportive, with avoidance of aspirin and NSAIDs due to the risk of hemorrhagic complications in the context of a possible viral hemorrhagic fever. 4
Prevention relies on personal protective measures, including repellents, protective clothing, and fine-mesh netting that can block biting midges, which are much smaller than mosquitos and can cross standard screens. Daytime protection with tightly woven clothing is essential.1,7 Environmental control involves reducing breeding sites such as damp soil, decaying vegetation, and standing water near dwellings.
7
Those concerned about OROV exposure should seek evaluation from public health agencies or infectious disease clinicians. Updated guidance is available from health ministries, CDC, PAHO, and WHO (Figure 1). OROV human disease cases reported by country. Previous is defined as human disease cases of Oropouche last reported prior to 2024. Recent is defined as human disease cases of Oropouche identified during 2024 to 2025. Courtesy of U.S. Centers for disease control and prevention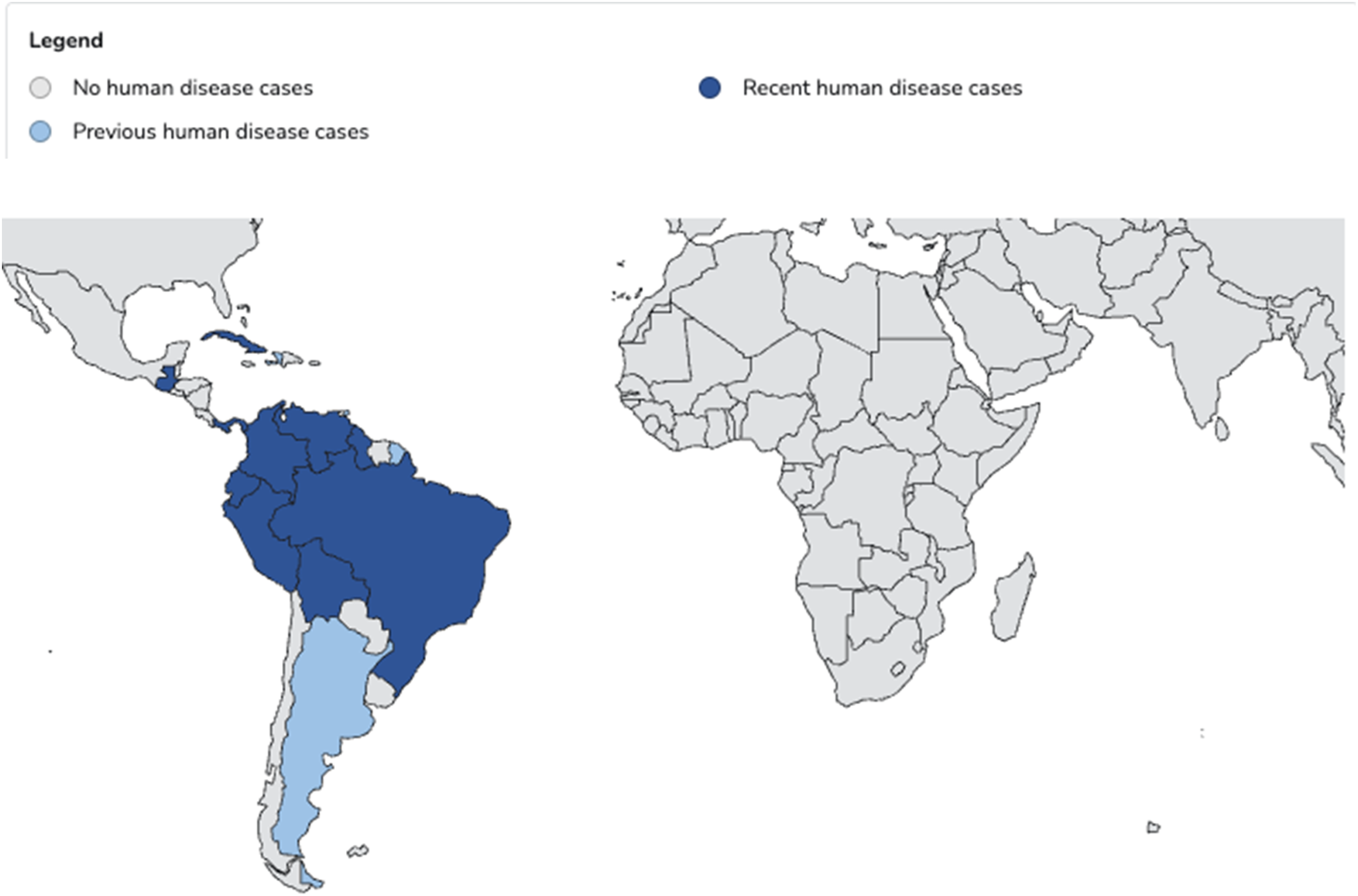
Footnotes
Declaration of Conflicting Interests
Mary Benson-Gallanis and Lakshmi Chauhan have no disclosures to report related to this work. Daniel M. Pastula has no disclosures directly related to this work. Outside of this work he reports consulting fees from Valneva and Pfizer, as well medicolegal consulting fees. Amanda L. Piquet has no disclosures directly related to this work. Outside of this work she reports institutional support from Genentech, the University of Colorado, and the Rocky Mountain MS Center, and royalties from Springer Nature for editorial services, consulting fees from Alexion and Genentech/Roche, honoraria from Medlink for a medical article. Kenneth L Tyler receives research funding from the Department of Veterans Affairs for studies with the flavivirus West Nile. Outside of this work he reports funding from the NINDS for studies related to EV-D68 neuropathogenesis.