
Abstract
NASN conducted a needs assessment to learn about the cultural competence skills needed by school nurses. The purpose of this article is to describe the results of the needs assessment and describe actions taken to address cultural competency needs for the U.S. school nurse workforce.

School nursing has a long history of addressing the cultural and social determinants impacting the health of students, families, and communities (California Institute Nursing Health Care, 2013; Loftin, Hartin, Branson, & Reyes, 2013). A person’s culture (beliefs and values) influences their understanding and treatment of their health. The influence of culture in the context of health care delivery in the United States continues to be critical as minorities are projected to comprise 57% of the U.S. population by 2060 (Loftin et al., 2013).
Yet, a review of the school nursing literature produced limited descriptive and correlational studies that focus on cultural competency and school nursing (McNaughton, Cowell, & Fogg, 2014; Muennich Cowell, McNaughton, & Ailey, 2000). NASN conducted an assessment in the fall of 2012 to learn about the cultural competence skills needed by school nurses. The purpose of this article is to describe the results of the needs assessment and the actions taken to address the identified cultural competency needs for the U.S. school nurse workforce.
Methods
In the fall of 2012, a cultural competence needs assessment questionnaire specifically designed for school nurses was executed with the goal of investigating the current practice and any gaps related to cultural competency among U.S. school nurses. The survey was created to measure the self-awareness (knowledge) and practice (skills) of school nurses and the availability of culturally appropriate resources and determine gaps for future educational programs. The majority of the assessment questions (21) came, with permission, from the National Center for Cultural Competence (NCCC) for self-assessment (NCCC, n.d.-a) and policy assessment (NCCC, n.d.-b). The Multicultural Awareness, Knowledge, and Skills Survey (MAKSS) provided the expert questions to assess three foci: awareness/knowledge, practice/skills, and resources by school nurses to interact with clients (D’Andrea, Daniels, & Heck, 1991). Eleven demographic questions identified the school nurses’ sex, race, ethnicity, age, level of education, number of years working as a school nurse, national certification, state certification, membership in NASN, languages spoken other than English, and cultural competency training within the last five years. The assessment survey was reviewed by several nursing experts and piloted among a small group of school nurses from diverse backgrounds before it was disseminated to the target population. The survey was sent to about 15,000 NASN members via list serves, website, weekly digests, and membership blasts, and local nurses were encouraged to share the survey with their non-NASN colleagues.
Results
The needs assessment was answered by 2,645 school nurses with 1,951 respondents identifying themselves as members of NASN. Demographically, 93.6% of the respondents identified themselves as Caucasian/White, 4.4% Black/African American, 1.4% Asian, 1.3% Native American/American Indian/Native Alaskan, and less than 1% Native Hawaiian/other Pacific Islander. The far majority (96.3%) identified themselves as non-Hispanic; 99% were female, with the majority between the ages of 45 and 64 years of age.
Familiarity With Population
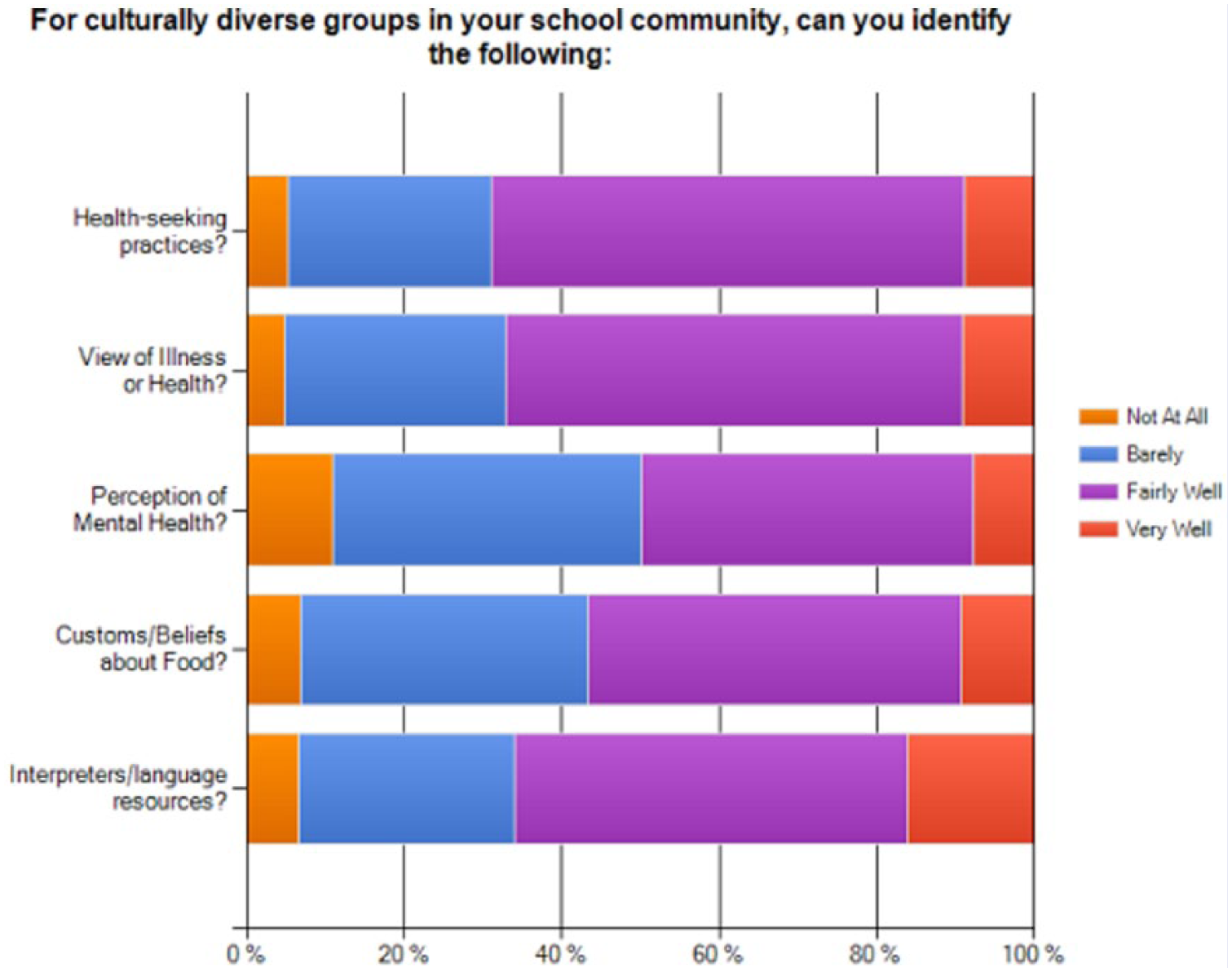
Overall, school nurse respondents were familiar at least fairly well with the demographics (78% of respondents), languages spoken (81%), religion (67%), and social strengths (51%) of the populations they served. The majority of respondents (81.3%) indicated they could describe health disparities in their specific populations. Respondents were also able to describe various social determinants of health that impact their school community: 83% could describe social environment (e.g., discrimination, educational attainment, income), 82.8% could describe physical environment (e.g., housing, transportation), and 85.7% could describe health services (e.g., access, quality of health care services, health insurance status). Figure 1 illustrates other cultural practices their population practiced.
School Nurses Knowledge Of Their School Community
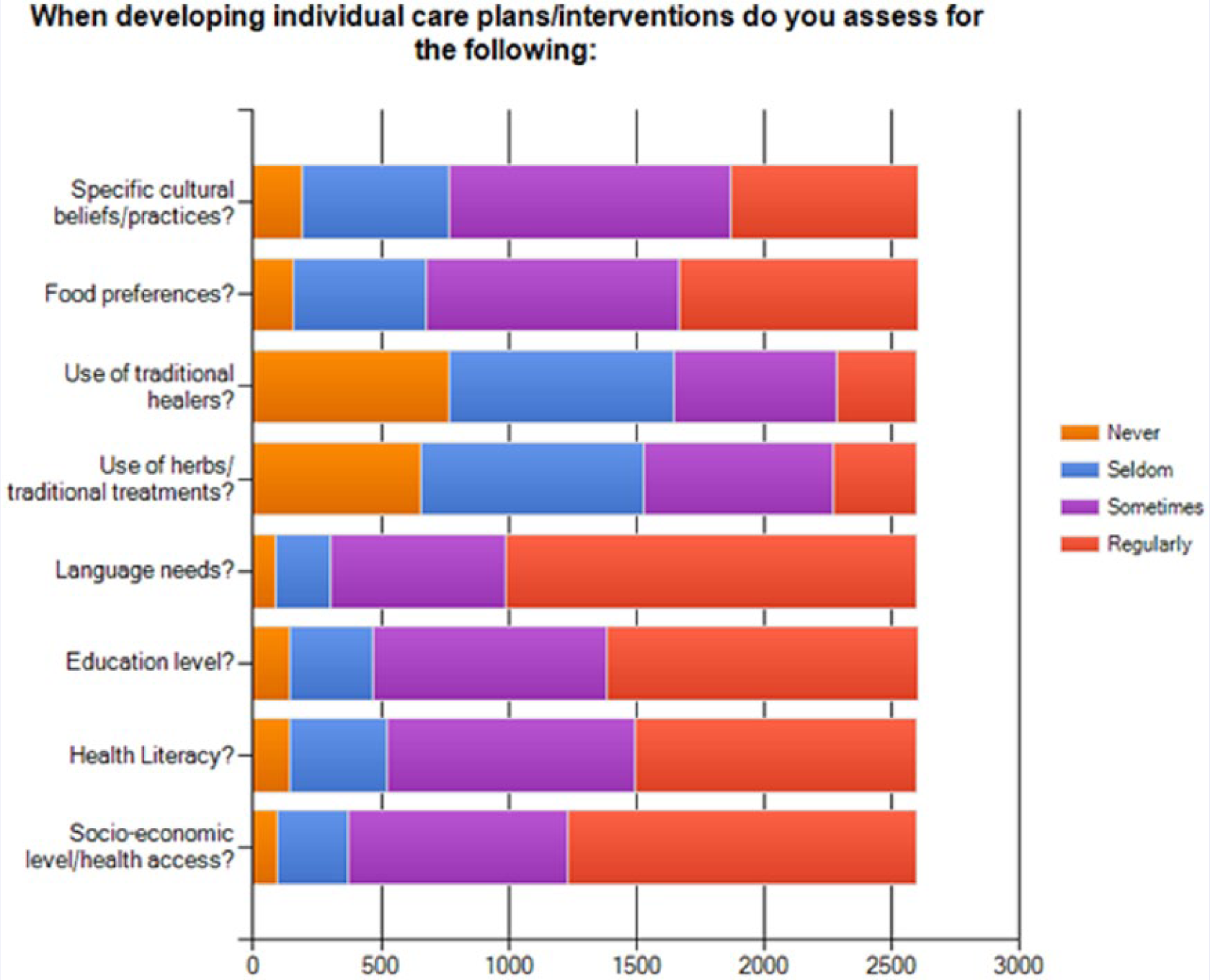
When asked about specific cultural beliefs and practices of their populations, the answers varied. Over half (64.3%) of respondents indicated they seldom or never assessed or addressed the use of traditional healers, and 58.8% of respondents did not assess or provide appropriate intervention regarding herbs/traditional treatments (see Figure 2 for further results).
School Nurses Culturally Appropriate Assessment Activities
Challenges to Providing Culturally Competent Care
Although school nurse respondents indicated they knew their population well and often assessed for cultural needs, the majority (approximately 95%) indicated barriers existed in being able to provide the care they would like. In order of importance, three themes emerged from the narrative responses as the greatest challenges to providing culturally competent care: language/communication, lack of resources, and work-related restraints. Specific results from the themes are further discussed.
Language/Communication
Respondents reported language and the ability to communicate in the parent’s language as the biggest barriers in providing culturally competent care in schools. Language was considered by 88.2% of respondents when developing individual care plans/interventions, but only 39.1% of respondents were able to ensure that all notices and communications to parents were written in their language of origin, and only 59.6% of respondents indicated the regular use of interpreters and bilingual/multilingual staff.
Resources
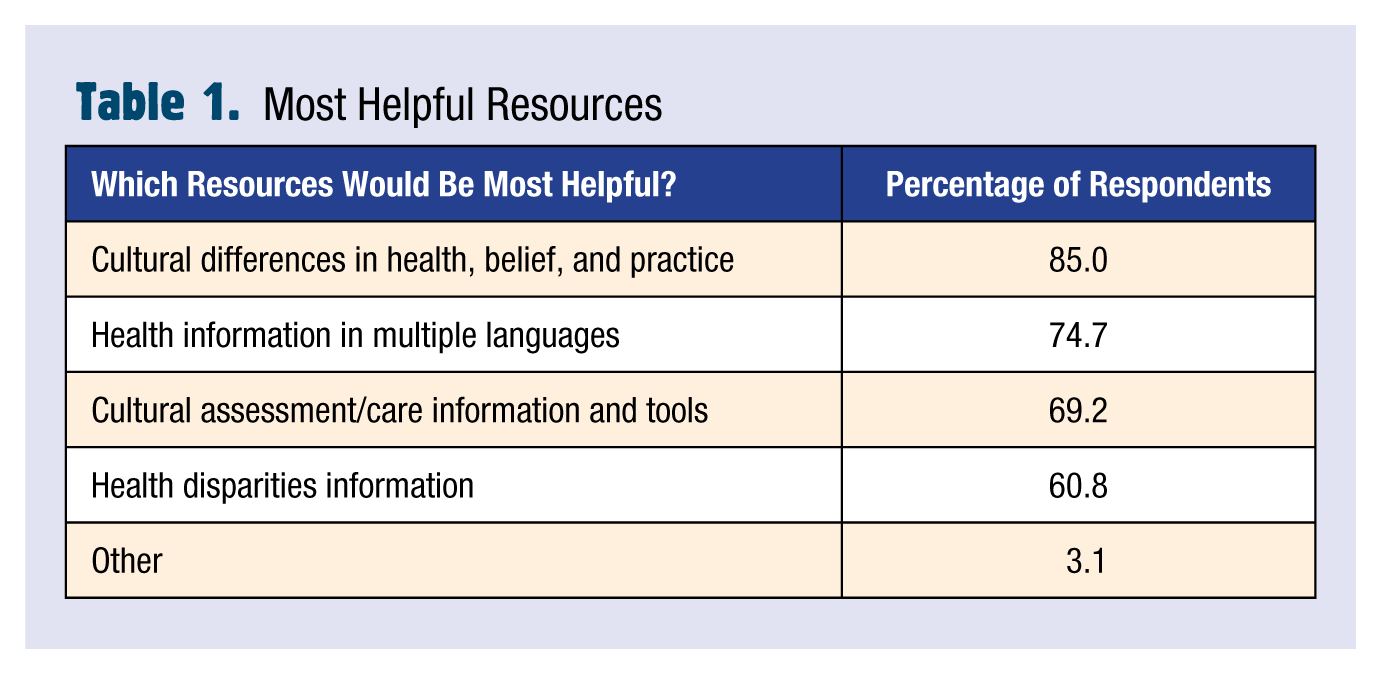
In the assessment, 85.9% of the respondents indicated materials specific to school nursing and cultural competency were needed. Respondents indicated the most helpful information needed was material to identify cultural differences in health beliefs and practice (85% of respondents), health resources in multiple languages (74.6%), cultural assessment tools (69.3%), and information about health disparities (60.8%). Responses included recommendations to ensure that all written communications be written in parents’ language of origin due to the identified inconsistency in access of bilingual/multilingual staff/interpreters. The narrative responses also described a lack of transportation, interpreters, and funding as resource barriers.
Work Force Issues
School nurses’ narrative responses identified work issues such as “lack of administrative support,” “lack of information sharing with educational staff and co-workers,” and “time constraints” barriers to providing culturally competent care.
Cultural Competence Training
The majority (95%) of school nurse respondents reported having had none to little cultural competency (CC) training as reported by attendance to CC workshops, training, or conferences within the last five years. Interestingly, those respondents indicating five or more CC trainings reported increased (a) confidence with levels of awareness; (b) ability to assess cultural beliefs, practices, and needs; (c) ability to use culturally adapted health promotion/disease prevention interventions; (d) use of appropriate health literacy and language resources; and (e) the ability to intervene in instances of cultural insensitivity/bias.
Nearly 86% of the school nurse respondents identified a need for accessible and school nurse–specific cultural competency education and training. Table 1 outlines the type of materials wanted. The respondents preferred web-based training (link) (65.9%) as opposed to face-to-face training (22.8%) or webinar (11.3%). Other strategies proposed by the respondents included: the creation of a web-link to direct school nurses to cultural resources, a resource hub with a drop box for sharing of information, the development of a cultural school nurse listserv, and the postings of educational forums, including opportunities to learn another language.
Most Helpful Resources
Actions Taken
The demographics of the respondents reflect the lack of diversity of school nurses and further support the need for skills in working with populations different than their own (Maughan & Barrows, 2013). NASN reviewed the results of the assessment, which were used to develop a website (http://nasn.org/ToolsResources/CulturalCompetency). The site provides much of the resources requested by school nurses and includes information on particular cultures, cultural and language resources for school nurses, and a sample assessment tool that can be used to assess the needs of the family.
Assessing specific family needs and incorporating such beliefs and practices is an important skill for school nurses. Nurses should not assume everyone from a specific culture holds similar beliefs and practices. Therefore, assessing for individual needs is still very important and should be part of the regular training received by school nurses, beyond what is found on the website.
In addition to the assessment is the need to know how to incorporate cultural beliefs and preferences into care plan interventions (Airhihenburwa, Ford, & Iwellunmor, 2014). School nurses may not be aware of the strong association between traditional medicine, food choices, colors, and the correlation among all these factors with folk theories (e.g., hot and cold theory) (Sanchez-Birkhead, Kennedy, Callister, & Miyamoto, 2011). These differences may be crucial in the adherence of care plans for immigrant and less acculturated immigrant families (Whitman, Davis, & Terry, 2010).
NASN also facilitated several breakouts on cultural competency at their annual conferences, one of which was a preconference that was taped in 2015 so that others may view it (and earn continuing nursing education credit). NASN is working with other agencies to develop an additional webinar that specifically addresses how the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (National CLAS Standards) relate to school nursing.
Language was identified as the greatest barrier for school nurses, which is understandable because language barriers can prevent school nurses from engaging with students and families whose primary language is not English regarding information that make a difference in student safety, attendance, and academic achievement (Whitman et al., 2010). The U.S. Department of Education’s Office of Civil Rights (2015) reinforces language services must be provided by districts to students and their families who have limited English proficiency. School nurses need to advocate in their school district for availability of such services.
The website, preconference, and upcoming webinar do not meet all the needs and barriers identified, but it is a start. Cultural competency is a journey—a website and training is not enough. School nurses should seek additional opportunities to enhance their skills regarding culture.
Conclusion
Through greater cultural knowledge, awareness, and skill, school nurses deconstruct the barriers to health care resources, unlock the path to academic achievement, and in turn nurture environments that produce healthy communities and open pathways for students into higher education. Inadvertently, the impetus to increase cultural knowledge and communication provides a strong basis to diversify a future school nurse workforce by (a) creating partnerships with diverse students and their families today and (b) optimizing the realization of potential nursing careers among our culturally diverse students. School nurses can change the landscape of health in the nation by providing appropriate, cultural care themselves while also outreaching to the next generation of nurses to ensure a more diverse nursing workforce. ■
Footnotes
Dr Matza is the School of Nursing’s community health clinical resource faculty. Her research focus is on cultural diversity and health and serves as a member of NASN’s Cultural Competency Advisory Board.
Erin is the Director of Research at NASN. Before that she served as the Coordinator of International Affairs for the College of Nursing at Brigham Young University in UT, where she also coordinated the global health nursing program.
Beth is a clinical instructor in the School of Nursing and is involved in the professional development of nurses in the Caribbean and Africa. She worked on this project as part of her public health nursing leadership practicum with NASN in Fall Semester 2012.