
Abstract
In order to provide holistic care, school nurses must be culturally competent by being sensitive to health disparities experienced by students in at-risk populations. Despite the growing acceptance toward gender and sexual minorities, LGBTQ youth remain an at-risk population in our communities and our schools. School nurses as well as school counselors, social workers, and psychologists can increase their cultural competence in caring for this group of students by increasing their understanding of appropriate terminology and risks associated with this vulnerable group. This article is Part 1 of a two-article series designed to increase school nurses’ abilities to advocate and care for LGBTQ youth in school settings. This first article provides information regarding proper terminology and current percentages of youth who identify as LGBTQ and concludes with implications for school nurses, including resources for nurses, school staff, and families.
Introduction
While school nurses are well aware that culturally competent care is an essential component of caring for children from a wide variety of geographic locations or religious identities, they may not routinely consider the need for cultural competence in caring for youth who identify as lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ). The same principles of cultural competence apply to this group of students and require school nurses to understand and use appropriate terminology describing these students as well as learn how the social environment these students live in impacts their health and well-being (Betancourt, Green, Carrillo, & Ananeh-Firempong, 2003). The purpose of this article is to provide nurses with epidemiologic data and terminology that describes the LGBTQ youth community, review the current legal and cultural environment for these students, and discuss implications of this information for school nurses.
The most recent Youth Risk Behavior Survey (Kann et al., 2016) indicates that 11.2% of high school students self-report being gay or lesbian (2%), bisexual (6%), or unsure of their own sexual identity (3.2%). In some urban areas, as few as 77.6% of students report identifying as heterosexual. Thus, school nurses are likely to encounter students who identify as LGBTQ. Data indicate that this group experiences multiple health disparities, including higher rates of depression, suicidal ideation, and suicidal attempts (Kann et al., 2016). One way to begin avoiding stereotyping this group and improving health outcomes is to understand and thus use appropriate identifying language.
LGBTQ Concepts, Terms, and Definitions
Understanding and use of appropriate terminology for LGBTQ youth is important so that school nurses communicate in a consistent and professional manner to students, faculty, and administration. This section expands on the context of the terms found in Table 1 that are acceptable to use when working with LGBTQ youth. In order to reflect the diversity of identities that exists within the LGBTQ community, this article uses the terms gender and sexual minorities, LGBTQ, and queer interchangeably. For clarification purposes, sexual minority denotes individuals who may harbor same-sex attractions, engage in same-sex sexual behaviors, or identify as lesbian, gay, bisexual, queer, or questioning (Kann et al., 2016). On the other hand, gender minority refers to individuals whose gender identity or expression does not conform to the cultural norms associated with their sex at birth (Collier, van Beusekom, Bos, & Sandfort, 2013; National Institutes of Health [NIH], 2013). Finally, the term queer is largely used as an umbrella term as it aptly demonstrates the diversity and fluidity of sexual orientation and gender identity (Human Rights Campaign, 2016). Although sexuality and gender identity are frequently conflated, they are actually two separate, unrelated topics that are unpredictive of each other (American Psychological Association [APA], 2014).
LGBTQ Concepts, Terms, and Definitions
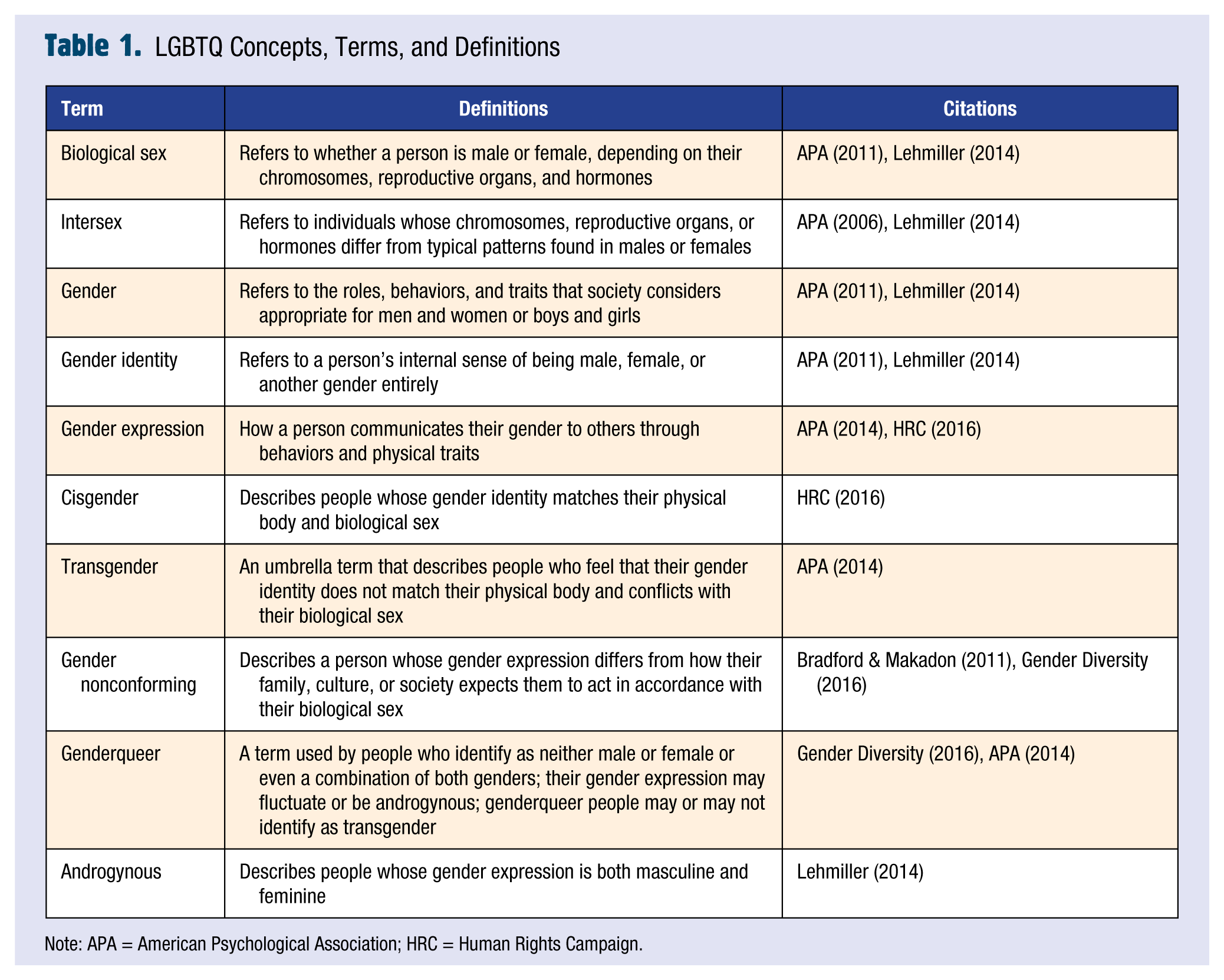
Note: APA = American Psychological Association; HRC = Human Rights Campaign.
The terms in the table are not meant to be exhaustive lists, and in many cases, individuals’ gender identities and sexual orientations will not easily fit into the prescribed categories. Moreover, youths—just like adults—have varying perspectives on the centrality of their gender and sexual orientation to their identity. Each individual uniquely experiences their gender and sexuality in ways that cannot always be perfectly described through labels. School nurses can help ease the social burden on queer youths by helping them identify their feelings, using language that affirms their identity and creates an environment where queer youths can safely express themselves without fear of judgment or retribution.
Correctly using these terms not only requires practice but also patience and empathy toward queer children and adolescents. School nurses can best serve these youths by asking which terms feel most comfortable to them and which ones they should eschew in order to avoid unintentional misunderstanding and degradation. Misuses of these terms, even if done so accidentally, can recreate prejudices and invalidate the experiences of gender and sexual minority youths, who may already be feeling isolated as a result of their identity. Proper usage of these terms coupled with compassion reaffirms children’s experiences and can leave an indelible mark on youths who merely seek understanding and acceptance.
Sexuality Concepts and Terms
Children, long before they identify with a particular sexual orientation, have sexual feelings (Kellogg, 2010; National Child Traumatic Stress Network, 2009). Often, gender nonconformity in childhood is seen as a harbinger of future homosexual feelings and attraction. However, childhood gender nonconformity may be related or unrelated to one’s sexual identity later in life (American Academy of Pediatrics, 2015). Moreover, the growing liberalization of gender norms and repudiation of gender stereotypes have enabled children to express themselves in ways that may have once been seen as incongruent with their assigned gender at birth. One’s sexuality is separate from one’s gender identity and expression. Sexual orientation refers to one’s physical, emotional, and romantic attraction to others, which can include people of the opposite sex, same sex, or both sexes (APA, 2008; Lehmiller, 2014). In comparison, gender identity refers to a person’s internal sense of being male, female, or another gender entirely (APA, 2014; Lehmiller, 2014).
In general, many people are uncomfortable with ambiguity and naturally sort things into recognizable categories that have distinct patterns. However, sexuality is fluid, overflowing categories and transcending cultural norms. For example, the Youth Risk Behavior Surveillance Survey found that both hetero- and homosexual youth report sexual encounters with both same and opposite gender individuals (Kann et al., 2016). Instances such as these should not be perceived as an inability of others to firmly state an attraction or as evidence that queer individuals can somehow be “converted” to heterosexuality. Rather, they should serve as reminders that a single label cannot possibly encapsulate a person’s entire sexual experience. Indeed, 9.2% of youth self-identify as bisexual or unsure of their sexual identity (Kann et al., 2016). Ultimately, identities mean different things to different people, and in the tumultuous development phases of childhood, it is normal for youths to question their sexuality and explore their sexual feelings.
Gender Identity Concepts and Terms
As soon as they are born, children are automatically categorized as either male or female based on their physical characteristics, specifically their genitalia and chromosomes. These innate markers determine an individual’s biological sex (APA, 2011; Lehmiller, 2014). For approximately 1 in 2,000 newborns, over 60 different conditions may make this question of boy or girl difficult to answer. In these infants, chromosomes, gonads, internal sex organs, genitals, or some combination thereof differs from the prescribed patterns of male or female (American Academy of Pediatrics, 2014; APA, 2006; Lehmiller, 2014). The complex treatments and ethical issues related to care of these children are beyond the scope of this article, but school nurses should note the existence of these children and follow the same respectful guidance in care for LGBTQ individuals.
Once a child’s biological sex is determined, gender stereotypes are instantly applied and expected to come to fruition. According to cultural norms, only two genders exist, specifically boy and girl, which correspond to one’s biological sex, respectively, male or female. In turn, this division causes certain characteristics to be prescribed as either masculine or feminine. Subsequently, most parents envision their child’s future in gendered ways. For instance, while boys are expected to thrive in rough-and-tumble play, girls are pressured to engage in sophisticated pursuits, such as the arts and humanities. This socialization is reinforced throughout early childhood as youths continue to gravitate toward gender-specific clothing, toys, and activities. In sum, these observable mannerisms and preferences form an individual’s gender expression, or the way in which one presents their gender through their physical appearance and outward behaviors (APA, 2014; Human Rights Campaign, 2016).
Traditionally, one’s gender expression has been constrained by culturally acceptable traits for males and females; however, attitudes have shifted toward recognizing gender roles as inaccurate and constricting as most individuals display a range of historically masculine and feminine behaviors. Similarly, just because some characteristics are considered to be masculine or feminine does not mean that they are mutually exclusive. As such, instead of imagining gender roles on a spectrum, with one end designating masculine expressions and the opposite end representing feminine expressions, it is useful to imagine the concept of gender as either a galaxy or a universe; just as there are an infinite number of stars in space, there are also an infinite number of ways in which one can express their gender identity. Questioning one’s gender and changing one’s gender expression is also quite common. As with sexual identity, it is perfectly normal for a child to frequently change their gender presentation as the concept of gender is more fluid than society typically recognizes (American Academy of Pediatrics, 2015).
Most people’s gender identity correlates with their biological sex (APA, 2014; Lehmiller, 2014). These individuals may be described as being cisgender, meaning that the gender they feel they are on the inside overlaps with their gender expression and their assigned sex at birth (Human Rights Campaign, 2016). Nevertheless, some individuals feel a dissonance between the gender they truly are on the inside and the gender others perceive them to be based on the body they were born into. These individuals may identify as transgender, genderqueer, or gender nonconforming (APA, 2014). Identification as transgender is more common in young adults than in older adults, with approximately 0.7% of 18- to 24-year-olds self-reporting this identity (Flores, Herman, Gates, & Brown, 2016). Although these identities may seem abstract at first, there has been a growing acceptance within the medical and psychological communities of gender dysphoria as a normal variation in how some people experience their bodies and gender (NIH, 2013).
While the term transgender may be the most recognizable and the term used in national survey data, just as there are many different ways of being a man or a woman, there are also many different ways of being transgender. For example, some transgender individuals seek to find a balance between the gender they really are on the inside and the gender the world perceives them to be by socially transitioning. For some, this may mean changing their pronouns, names, and physiognomy through nonmedical means. Meanwhile, others may opt for medical treatments such as hormone therapy or surgery.
In comparison, the term genderqueer describes a person whose gender identity and expression do not neatly fit into the narrow, easily defined categories of male or female. Genderqueer individuals may identify as neither female nor male or even a combination of both genders. Their gender expression may fluctuate often, or they may choose more androgynous presentations. Typically, genderqueer individuals reject the dichotomy of male and female and in doing so take a political stance against society’s rigid gender binary definitions (APA, 2014; Gender Diversity, 2016).
Thus, as transgender and gender-nonconforming children age and as their feelings about their identity become more acute, navigating their schools and communities can become progressively harder as they are continually forced to reconcile who they really are on the inside with how others perceive them. Transgender and gender-nonconforming youths and their families face unique challenges, such as transitioning socially, explaining themselves to others, and living as authentically as possible in environments that may be inhospitable toward their true identity. See Table 2 for a synopsis of the gender identity terminology.
Gender Identity Concepts and Terms
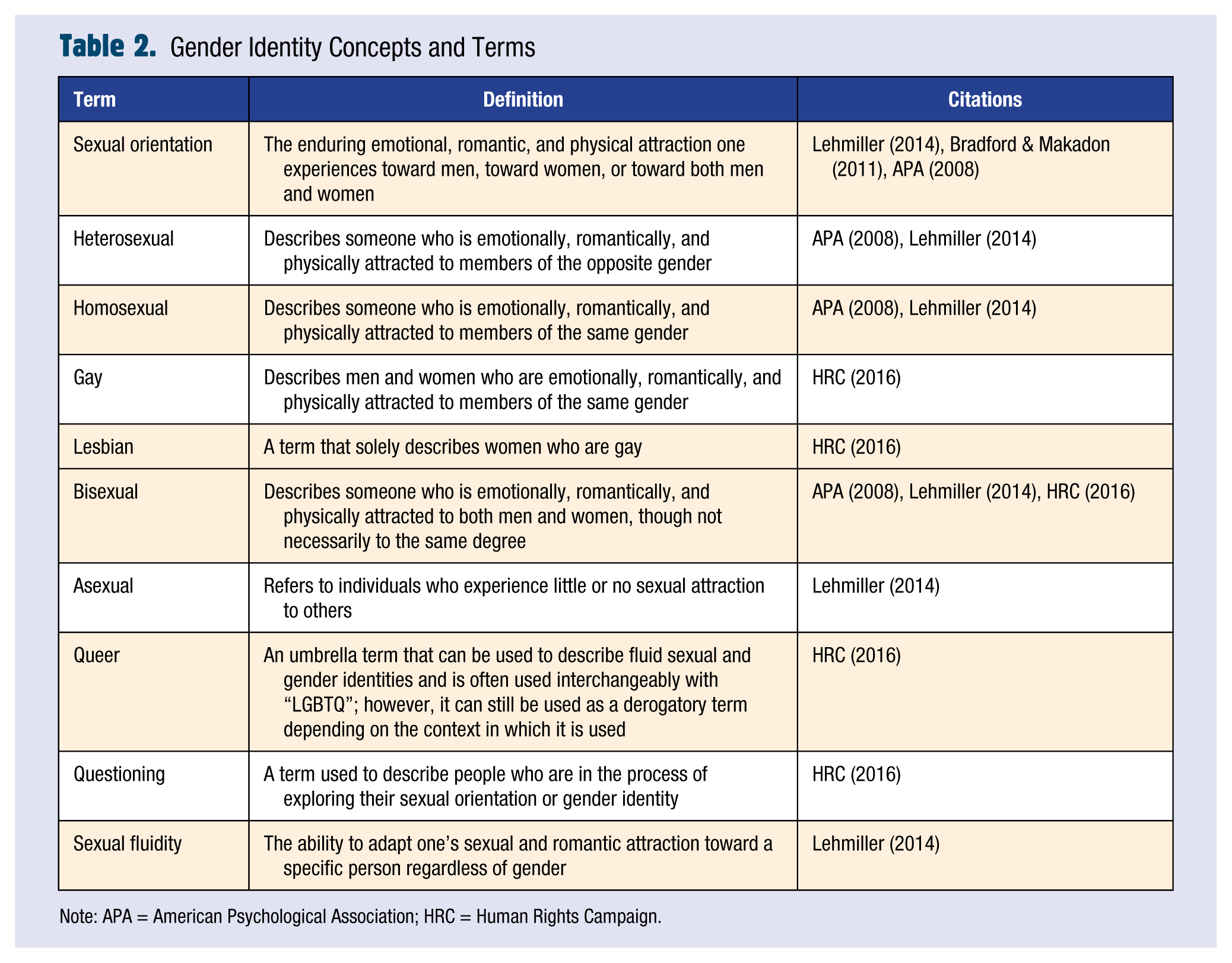
Note: APA = American Psychological Association; HRC = Human Rights Campaign.
Historical Perspective
It is difficult to overstate the progress the LGBTQ community has made toward full political and social equality just within the past decade. As of 2016, 55% of American adults currently support same-sex marriage; comparatively, in 2006, 55% of U.S. adults opposed same-sex marriage (Pew Research Center, 2016). Since 2004, when Massachusetts became the first state to legalize marriage equality, support for same-sex marriage steadily increased until June 2015 when the United States Supreme Court officially legalized marriage equality nationwide.
Legal recognition and social support for the LGBTQ community has not been limited to only lesbian and gay couples. The states of Vermont, California, New Jersey, Illinois, and Oregon, along with the District of Columbia, have banned the use of so-called “conversion therapy” on minors, which the American Psychiatric Association (2000) has attributed to depression, self-harm, and suicide. Moreover, Medicare and certain state and private insurers now cover transgender-specific medical care, including hormone therapy and gender-confirmation surgeries. Finally, although they are still a minority, LGBTQ characters are more common and portrayed more positively than ever before in television shows and movies (Bond, 2015).
LGBTQ youths continue to face stark challenges within their academic and local communities as a result of both verbal and physical harassment (Human Rights Campaign, 2014). It is difficult to overemphasize the profound psychological consequences LGBTQ youths face when they are made to feel ashamed of their identities or are forced to hide who they truly are (Cooper & Blumenfeld, 2011; Hatzenbuehler, 2011; LeVasseur, Kelvin, & Grosskopf, 2013; Robinson & Espelage, 2011). Part 2 of this series explores these consequences in detail. Prior to addressing such consequences, school nurses have the opportunity to create and enhance safe spaces by utilizing appropriate langue for queer youths as they frequently serve as confidants to students and are often confronted with questions pertaining to sexuality.
Role of the School Nurse
Students may view the school nurse’s office as a place of refuge and solace, where they can privately disclose their feelings as well as ask personal questions they may be too fearful or embarrassed to share with another adult. Even if gender and sexual minority youths do not yet possess the language to fully express their identities, they typically have enough self-awareness to know that their feelings and experiences differ from those of their peers. School nurses can provide a nonjudgmental and private place for youth to discuss their thoughts and feelings and ask questions. School nurses should use appropriate language that affirms student identity and creates an environment where queer youths can safely express themselves without fear of judgment or retribution.
Nurses can provide basic information for youth regarding terminology and using national statistics, reassure youth either coming out or questioning that they are indeed not alone. Questioning one’s sexual and gender identity is a normal part of creating an adult identity, and nurses can aid in that process by supportive listening or providing referrals to counseling.
Additional use of correct language involves school nurses empowering queer youths by asking their preferred names, pronouns, and identity markers. Similarly, unless required in a health assessment, school nurses
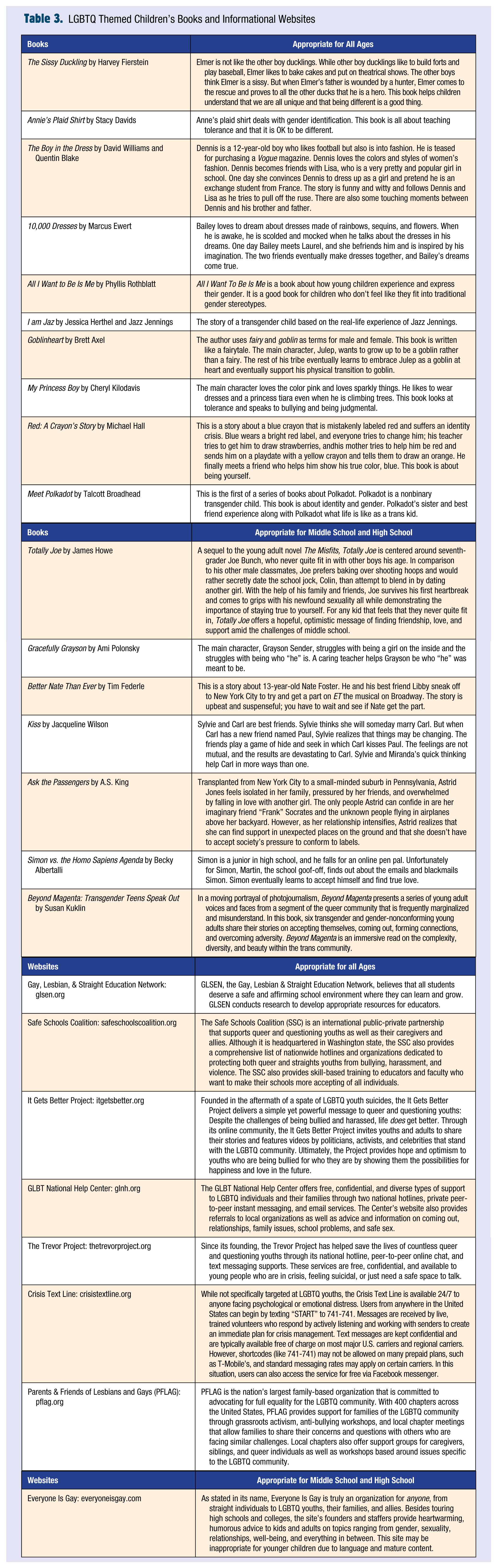
Providing thoughtful and respectful book and movie recommendations (Table 3) can provide a way for youth to share in LGBTQ stories and help them build their own sexual and gender identities. As part of working toward cultural competence, nurses can also read and watch these media as a way of increasing understanding of a variety of perspectives for the LGBTQ community. Reading and viewing may provide students, nurses, faculty, and administrators with a platform to discuss issues without having to refer to specific students.
LGBTQ Themed Children’s Books and Informational Websites
As youths are especially vulnerable to anti-LGBTQ messages in school environments, student feelings may also come to include loneliness, self-hatred, and a diminished sense of self-worth (Vaccaro, August, & Kennedy, 2012). Subsequently, these attitudes can become manifested in reactive behaviors, such as chronic absenteeism, psychosomatic symptoms, substance abuse, and acute anxiety and depression (NIH, 2013). Part 2 of this series addresses these health disparities and provides further implications for the role of the school nurse in reducing these disparities.
Finally, although this article largely aims to assist nurses in their interactions with gender and sexual minority youths, nurses can also use this newfound knowledge to educate not only their colleagues but also students and their families. The keywords, phrases, and resources enumerated in this article can and should be shared with youths and their caregivers to encourage discussions, clarify misinformation, and provide support in times that can be both confusing and isolating. Doing so can help children and their families embrace identity exploration and find solidarity in local and national organizations.
Conclusion
To create a healthier, safer environment for all students, school nurses can shape attitudes and ideologies, ameliorate prejudices, dissuade or embrace differences, and create negative or positive spaces for the entire school community. Using appropriate terminology and following anti-discrimination laws reduces stereotyping and use of potentially hurtful slang terms. Throughout these challenges, school nurses can play a multifaceted role by acting as advocates for gender and sexual minority youths as well as educators in promoting practices that affirm the experiences of LGBTQ children and their families. In doing so, nurses will have the profound opportunity to leave an indelible mark on countless youths and contribute to the establishment of a more just and safe school environment. ■
Footnotes
Acknowledgements
The Authors thank Carole Kenner for her guidance and support in the development of this article.
Dr. Tracy Perron is a registered nurse with over 25 years of experience. She has extensive experience in community health, school health, and public health. Dr. Perron has done research on bullying in school age children and is a Johnson and Johnson School Nurse Fellow.
Dr. Connie is a certified family nurse practitioner with experience in primary care, rheumatology, care of older adults, adherence, and intergenerational relationships.
Chaya is currently a third-year nursing student at the College of New Jersey.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.