
Abstract
This article is the second part of a two-part series on mental health in school-age children. The focus of this article is on mental health assessment in the school setting, including the use of screening tools, with a review of common medications prescribed for youth with anxiety and depression. Students with mental health conditions frequently seek refuge in the school health office, many times for psychosomatic complaints such as stomach ache, headache, nausea, and fatigue. School nurses need to be adept to assess mental health and intervene as necessary.
Keywords
This article is the second part of a two-part series on mental health in school-age children. The first article in the series provided a background of common mental health conditions, common symptoms, underlying complaints, along with a discussion and list of helpful resources for multiple audiences. The focus of this article is mental health assessment of individual students in the school setting, including the use of screening tools, with a review of common medications prescribed for youth with anxiety and depression.
Students with mental health conditions frequently seek refuge in the school health office, many times for psychosomatic complaints such as stomach ache, headache, nausea, and fatigue (Wigert et al., 2019). As noted in Part 1, during the coronavirus disease 2019 (COVID-19) pandemic, school nurses noted an increase in students experiencing mental health problems. School nurses need to be adept to assess mental health and intervene as necessary. The school nurse must make professional decisions about the level of assessment required when youth present to the school health office in mental distress. Early identification of children with mental health disorders by screening and referring leads to improved outcomes. Mental health emergencies such as substantial distress, a suicidal conversation, or act require a rapid, focused assessment and prompt intervention. The school nurse should complete a basic mental health assessment if the situation is not emergent. In emergent situations, such as expressing a plan to hurt themselves or others, an immediate referral is needed.
Mental Health Assessment
A mental health assessment consists of appearance, affect, speech, thinking, cognition, and judgment (Tolley, 2019). Much of the assessment can be completed through a general overview of the student, beginning with observing how the student is dressed and groomed. Students who appear disheveled, with poor hygiene, and not dressed age appropriately should be of concern to the school nurse, and it may be a result of depression or anxiety (Norris et al., 2016; Walter et al., 2020). General observations of psychomotor behavior can also be a sign of depression (e.g., slowed movements and responses) or anxiety (e.g., pressured speech, picking at self or clothing, or restlessness; Jarvis, 2020). The school nurse should focus on students who are expressing substantial needs or worries, or are communicating about sad topics and death. A mental health exam should include physical considerations. Vital signs may indicate anxiety (tachycardia and elevated blood pressure) or hypovolemia related to poor intake or self-induced vomiting (Jarvis, 2020). Changes in appetite and weight are part of the diagnostic criteria for depression (Tolley, 2019). Assessment also includes checking for signs of self-harm behavior, such as linear scars from cutting and annular lesions from burn marks (Burton, 2019). Basic first-aid measures can be applied while the rest of the assessment continues and the school nurse begins to decide what referral resources are indicated for the student.
School climate is an essential part of the assessment. This type of assessment will help the school nurse understand the level of stigma or support that a student with mental health conditions receives at their school. School climate has varying definitions but includes respect, fairness in policies, and relationships with teachers and staff (Colvin et al., 2019). Table 1 is a quick reference guide for school nurses to assess children in the school health office for depression and anxiety.
Mental Health Assessment
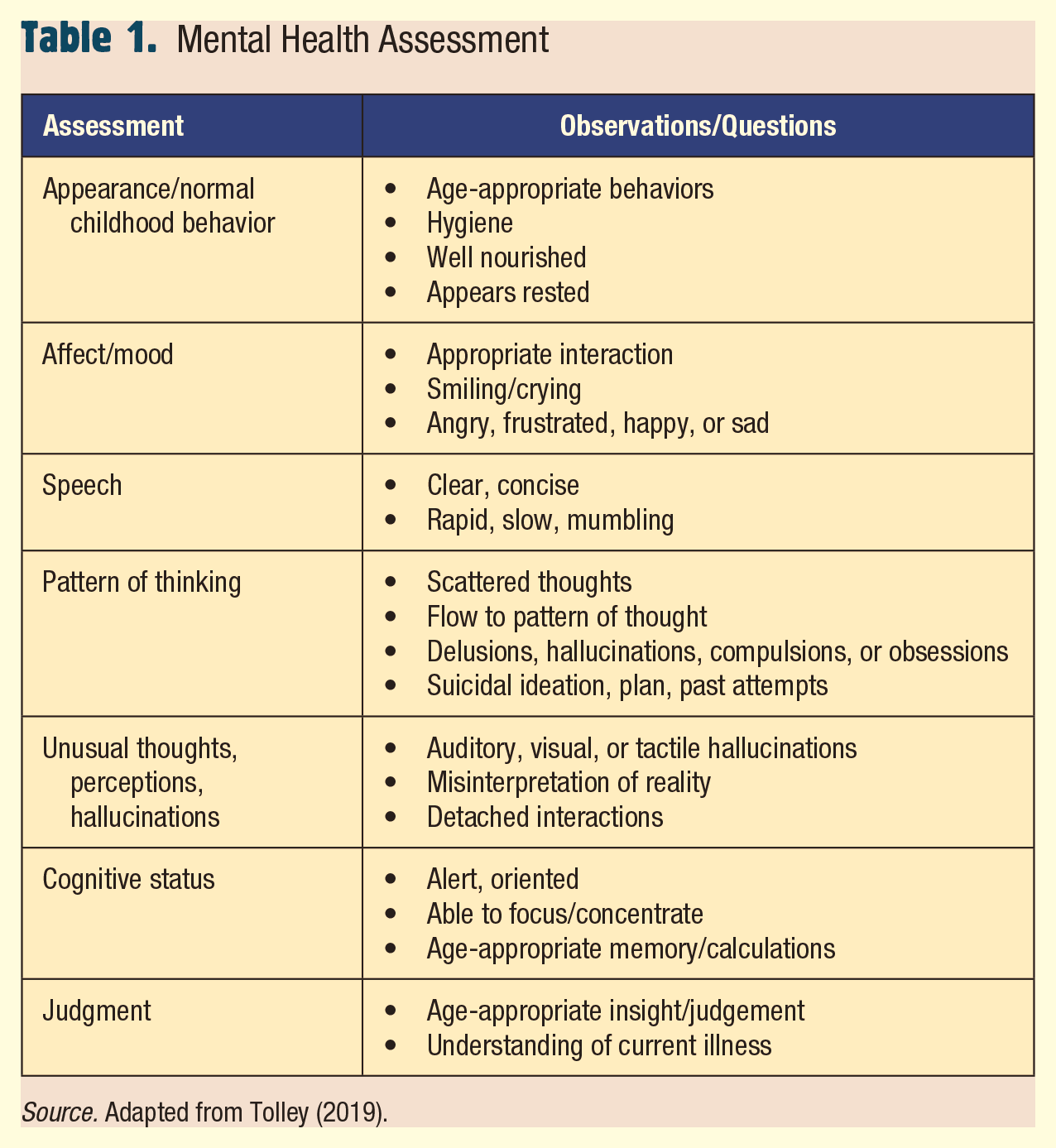
Source. Adapted from Tolley (2019).
Screening Tools
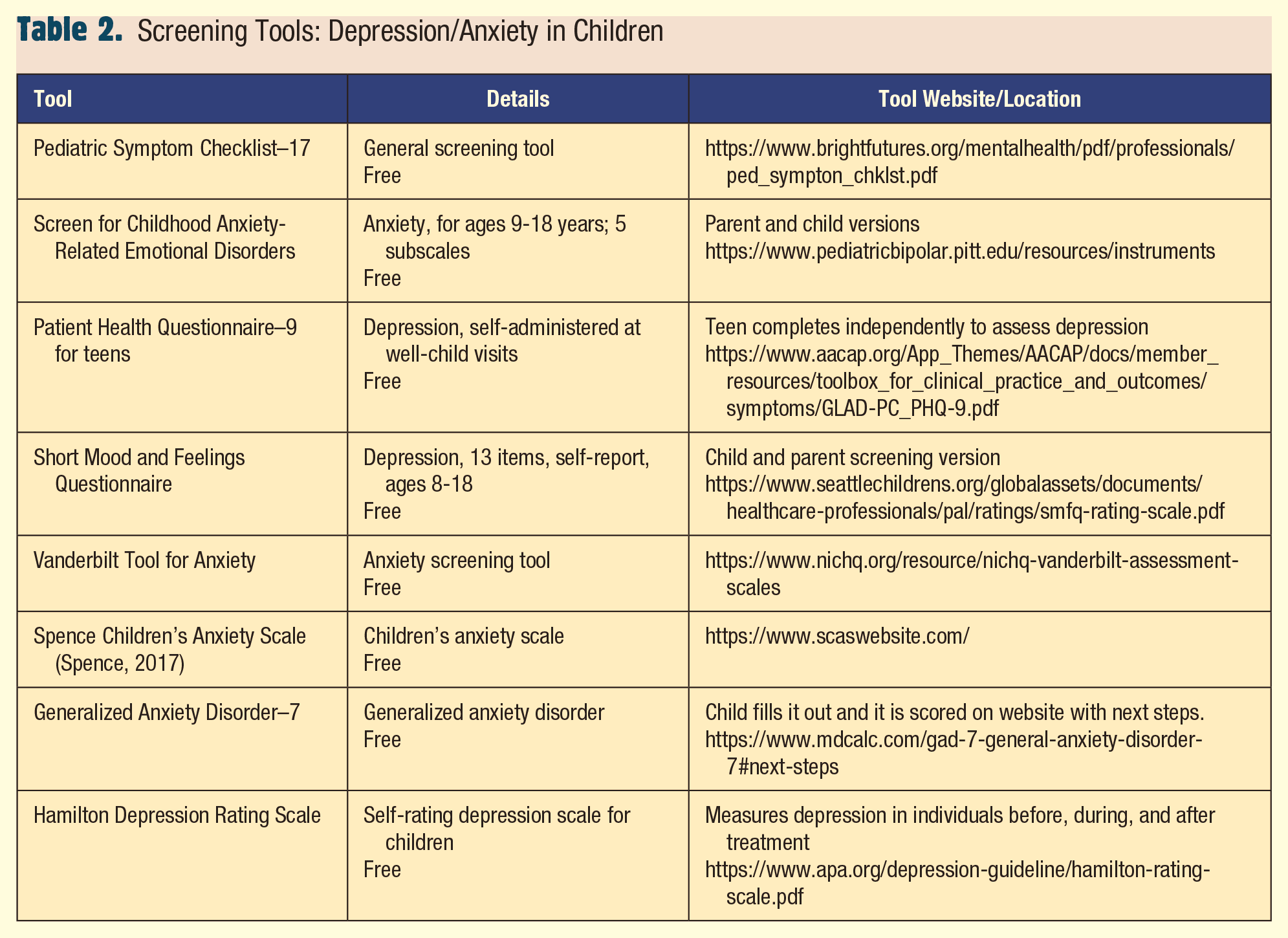
The U.S. Preventive Task Force (USPSTF) recommends that children 12 to 18 years of age be screened for major depressive disorders; the American Academy of Pediatrics (AAP) recommends an annual self-report screening tool be used at well-care visits (Selph & McDonagh, 2019). There are a variety of free screening tools for both depression and anxiety (Table 2). Schools are beginning to consider adolescent mental health screenings considering that many students are not seen regularly for primary care. District and parental approval are required for school-wide screening of adolescents, though school nurses will find screening tools appropriate for individual student assessments (Law et al., 2017). Screening tools should be scored promptly to identify emergent situations, such as suicidal thoughts.
Screening Tools: Depression/Anxiety in Children
Treatments
Effective treatments for depression and anxiety include interpersonal therapy, cognitive behavior therapy (CBT), and medications (Dawson, 2018; Walter et al., 2020). Children with mild depression or anxiety may be treated initially with psychotherapy along with close observation. CBT is the recommended therapy for both conditions. Initiating medication may be needed if there is no significant improvement in 4 to 6 weeks (Dawson, 2018; Walter et al., 2020). The combination of medication and talk therapies have better efficacy (Cheung et al., 2018; Walter et al., 2020).
Alternative Treatments
Nonpharmacological therapies for depression and anxiety may decrease symptoms and should be considered in cases of mild anxiety and depression and as a supplement to more severe symptomatology. Maintaining a healthy lifestyle through good nutrition, regular physical activity, and adequate sleep can help decrease symptoms (Hosker et al., 2019). A patient-centered treatment plan should be developed (Cheung et al., 2018; Walter et al., 2020). Behavior therapy, including child or family therapy, can also be included in the treatment plan. This will result in improved behavior, helping children manage symptoms by slowly exposing them to their fears (Centers for Disease Control and Prevention, 2020).
Play therapy may be used to treat depression in children, generally under the age of 12 years (Kids Mental Health Informational Portal, n.d.). Toys are used to encourage children to express themselves through play in a safe environment (Kids Mental Health Informational Portal, n.d.). Art therapy is another method that therapists use to encourage children to express themselves through drawings (Kids Mental Health Informational Portal, n.d.). Animal-assisted therapy may reduce stress and foster social interaction in children; horses and dogs are the most commonly employed animals (Kids Mental Health Informational Portal, n.d.).
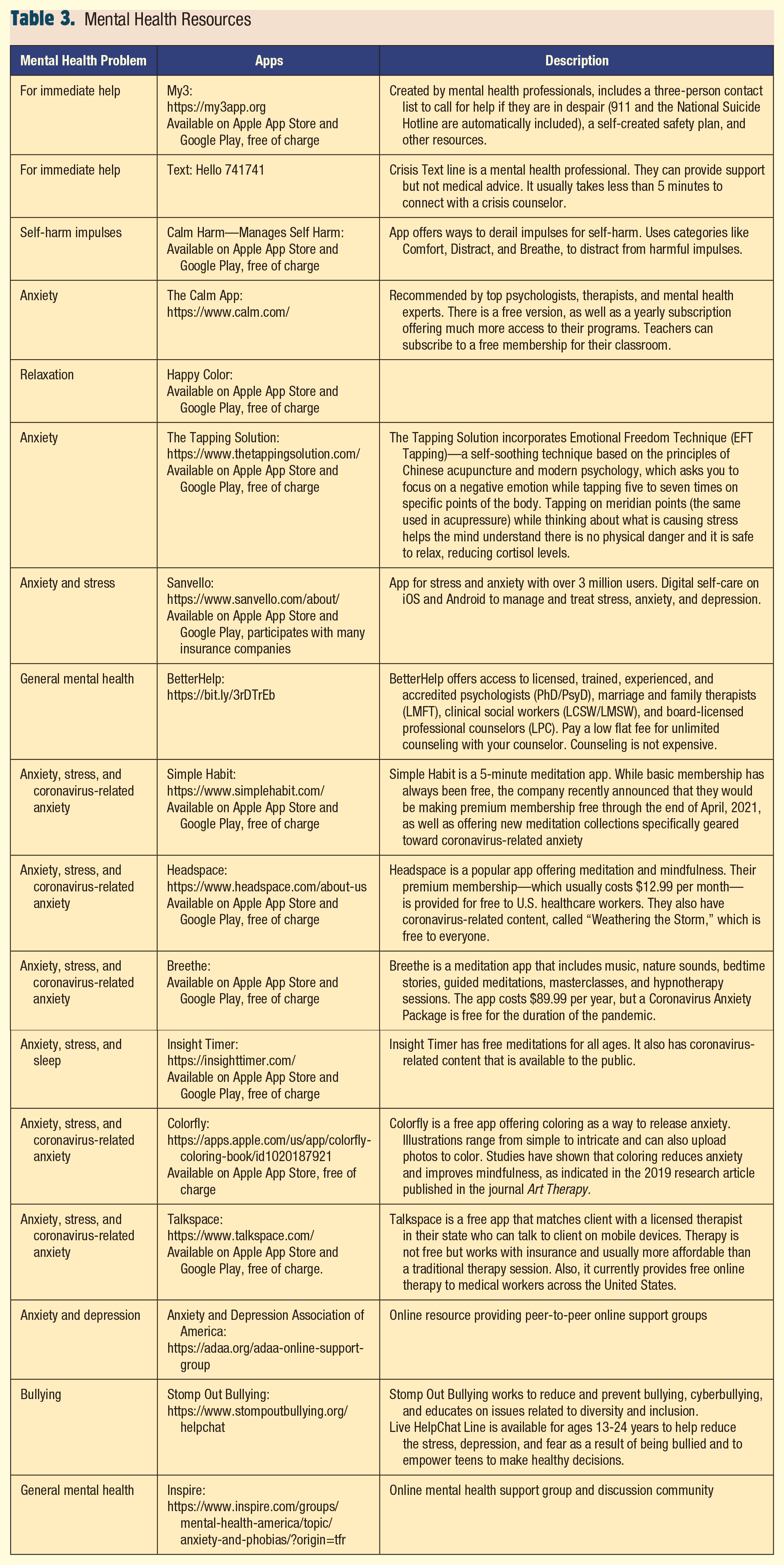
Mindfulness can teach kids to focus on the present moment, shifting the focus away from worrying about the past or future (Muggeo & Ginsburg, 2019). Guided imagery or breathing techniques may be used. Interventions to calm students such as providing a quiet place to rest, quiet music, or cool packs may be helpful (Muggeo & Ginsburg, 2019). Making time to talk with students about their anxiety and involving the school counselor may also be helpful (Muggeo & Ginsburg, 2019). It may also help train them to deal with future stresses. See Table 3 for free alternative intervention apps.
Mental Health Resources
Medications
Children with moderate/severe depression require prompt medication and psychological treatment, including close monitoring for suicidal thoughts (Cheung et al., 2018). Medications should be started at half the recommended dose and increased slowly over 6 to 8 weeks with careful monitoring for adverse effects (Dawson, 2018). Fluoxetine is the only antidepressant that can be stopped abruptly. Once symptoms of depression have been in remission for 6 to 9 months, the medication may be slowly discontinued over 2 to 3 months (Dawson, 2018). However, according to the GLAD-PC (Guidelines for Adolescent Depression in Primary Care) guidelines, medication should be continued for a full year following symptom resolution (Zuckerbrot et al., 2018). The first line treatment for depression in youth is selective serotonin reuptake inhibitors (SSRI); however, serotonin–norepinephrine reuptake inhibitors (SNRI) have also been found to be effective (Cheung et al., 2018). See Supplemental Table, available online, providing a comprehensive list of medications, including common side effects and concerns with dose adjustments.
SSRIs and SNRIs may be prescribed and are first-line treatments for anxiety (Walter et al., 2020). When treating children for anxiety, follow-up visits every 2 to 4 weeks are recommended to monitor the effects of medication. Once therapy is optimized, it is recommended to continue at maintenance doses for a year, and then taper slowly (Zuckerbrot et al., 2018).
Both SSRIs and SNRIs can cause serotonin syndrome if combined with other serotonergic medications such as triptans. Symptoms are wide-ranging and include mental status changes and neuromuscular and autonomic hyperactivity. Elevated blood pressure and pulse along with sweating, confusion, vomiting, and diarrhea may be noted. If untreated, serotonin syndrome can cause seizures; so immediate referral is necessary (Walter et al., 2020).
Implications for School Nurses
Students with mental health conditions frequently seek refuge in the school health office. Therefore, school nurses need to feel adept to assess and intervene with students as necessary. School nurses are positioned to help students with mental health conditions and their parents/caregivers navigate the healthcare system. School nurses can act as a support system and educate teachers, administration, parents, and students regarding signs and symptoms of youth struggling with mental health conditions. School nurses can advocate for students being treated for depression or anxiety by educating parents and teachers about the need for close symptom monitoring, especially during early treatment and medication dosing adjustments. Overall, school nurses need to support student academic success by promoting mental health in schools (National Association of School Nurses, 2018). ■
Supplemental Material
sj-docx-1-nas-10.1177_1942602X211011662 – Supplemental material for Mental Health Assessment of the Frequent Visitor-Part 2: Assessment and Interventions
Supplemental material, sj-docx-1-nas-10.1177_1942602X211011662 for Mental Health Assessment of the Frequent Visitor-Part 2: Assessment and Interventions by Tracy Perron, Tami Jakubowski, Cathy Razzi and Connie Kartoz in NASN School Nurse
Footnotes
Perron is an associate professor at The College of New Jersey. She is a certified school nurse and a certified nurse educator. She is a Johnson & Johnson School Health Leadership Fellow. She has an extensive background in community health and public health nursing. Her research interests include bullying among school-age children, school health, and childhood obesity.
Tami Jakubowski is an associate professor at The College of New Jersey, where she teaches pediatric nursing in both the undergraduate and graduate (FNP) programs. Tami has almost 30 years’ experience as a pediatric nurse practitioner, including pediatric primary and acute care. Her research interests include childhood obesity prevention, pediatric health promotion, and enhancing clinical learning environments. Tami is a Johnson & Johnson School Health fellow.
Cathy Razzi is an assistant professor at Gwynedd Mercy University. She teaches undergraduate nursing courses across the curriculum, including health assessment and genomics in nursing. Her research interests include issues affecting students, service learning, interprofessional education, transition to practice, novice nurses, and healthy work environments. She has presented and published on her incivility project, which was completed to fulfill requirements for her DNP at The University of Alabama in Huntsville.
Kartoz is a certified family nurse practitioner, with experience in primary care, rheumatology, care of older adults, adherence, and intergenerational relationships.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.