
Abstract
The National Association of School Nurses supports immunization to reduce the incidence of vaccine-preventable diseases. School nurses have the obligation to discern and understand vaccine strategies to aid in the advocacy and education of their school administrators, faculty, staff, students, and caregivers. Coronavirus disease 2019 (COVID-19) has spread to all continents, and the total number of those infected or immune through effective vaccination is well below the estimated need for herd immunity. To achieve herd immunity against the global outbreak of COVID-19, the rapid development of safe and effective vaccines is essential. Using multiple strategies and vaccine platforms to speed up the vaccine development process will inherently save more lives. Equipped with this knowledge of vaccine strategy, the school nurse can more aptly advocate for the use of the COVID-19 vaccines to move toward herd immunity in their communities.
At the time of writing (May 5, 2021), there have been 153 million cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) also known as coronavirus disease 2019 (COVID-19) with nearly 3.3 million deaths worldwide due to COVID-19. In the United States, we have exceeded 32 million confirmed cases with 577,172 deaths according to the Johns Hopkins University and Medicine Coronavirus Resource Center (Dong et al., 2020). For the latest statistics, access the Johns Hopkins webpage at coronavirus.jhu.edu.
Global Vaccine Strategy
The National Association of School Nurses (NASN, 2020) supports immunization to reduce the incidence of vaccine-preventable diseases. School nurses have the obligation to know and understand the vaccine strategies to aid in the education of their administrators, faculty, staff, students, and caregivers. COVID-19 has spread to all continents, and the total number of those infected or immune through effective vaccination is well below the estimated need for herd immunity (Triggle et al., 2021). To achieve herd immunity against the global outbreak of COVID-19, the rapid development of safe and effective vaccines is essential. In the past, with traditional or classical forms of vaccine development, it was not unusual for it to take years to develop a vaccine for a novel pathogen. Using multiple strategies and vaccine platforms to speed up the process will save more lives. Two main vaccine platforms are being used to develop COVID-19 vaccines, the classical and the next-generation platforms (Callaway, 2020; Thanh Le et al., 2020).
Classical Vaccines
Classical vaccines are manufactured using conventional methods and are either virus based or protein based, with the development platforms using either whole inactivated virus, live attenuated virus, protein subunit, or virus-like particles. Table 1 provides a glossary of the terms used in the article.
Glossary of Terms
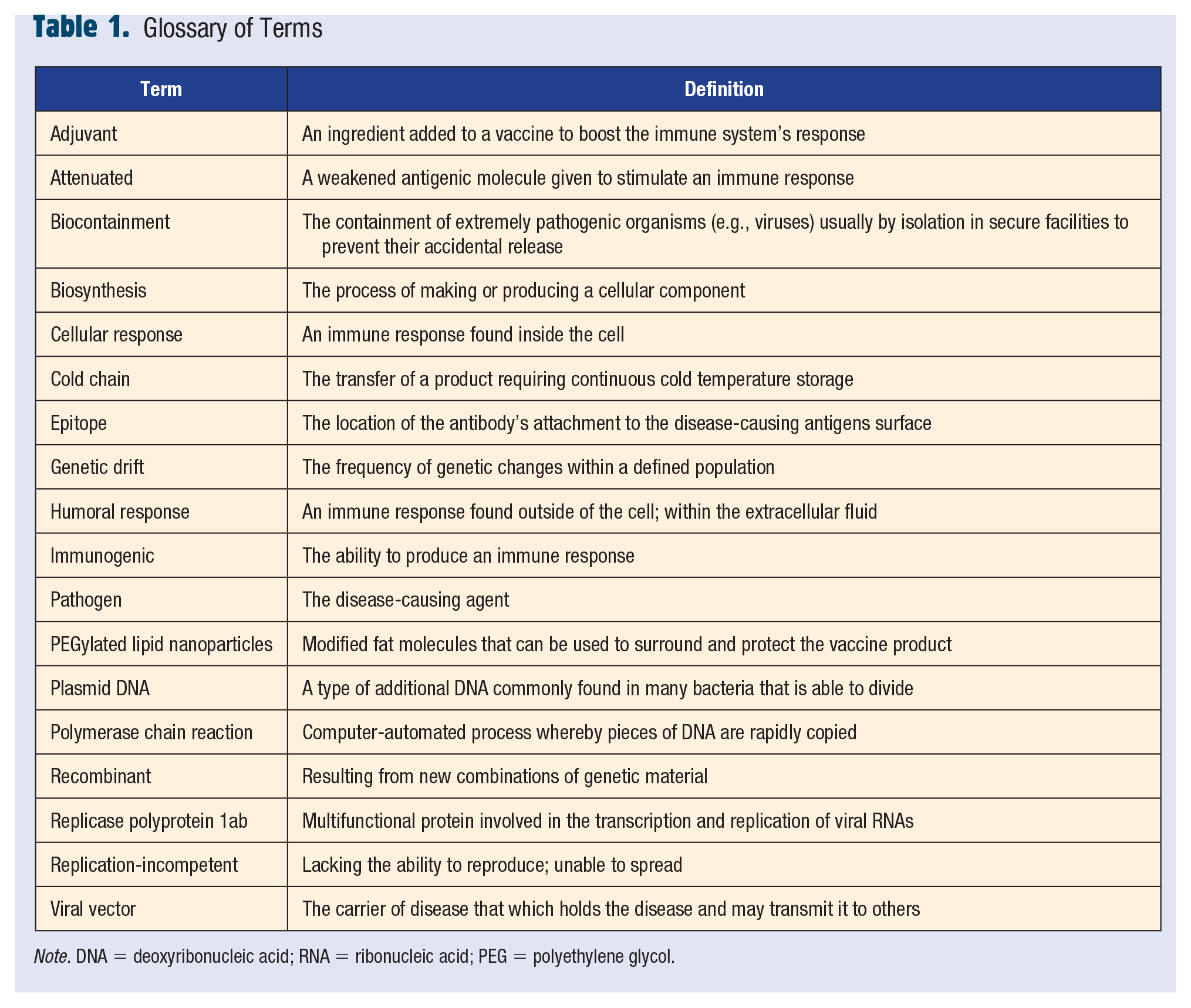
Note. DNA = deoxyribonucleic acid; RNA = ribonucleic acid; PEG = polyethylene glycol.
Inactivated Virus
Inactivated virus vaccines are made using traditional methods of vaccine development, starting with the live virus whose genetic material has been killed or destroyed, and therefore, cannot replicate and cause disease. The inactivated vaccine can be given to people with weakened immune systems (Chakraborty et al., 2021).
Live Attenuated Virus
The live attenuated vaccines are traditional or classical vaccines that use a weakened form of the virus (the actual pathogen) to stimulate an immune response. Although using a weakened form of the virus, immune responses are still triggered. However, the live attenuated vaccines may cause disease in people with weak immune systems and often require cold storage. With regard to COVID-19, there is a risk that a live attenuated COVID-19 vaccine could cause COVID-19 in an immunosuppressed person (Chakraborty et al., 2021).
Recombinant Protein Subunit or Virus-like Particle
Protein-based vaccines can be developed using viral protein subunits, but they require adjuvants to stimulate the immune system. Virus-like particles contain the structural proteins of the viral capsid. They do not contain the viral genome and critical nonstructural proteins (Karpiński et al., 2021). The adjuvant used in these types of vaccines is critical. Adjuvants stimulate pattern recognition receptors directly or indirectly to stimulate the immune system in the recipient. When two vaccines with the same antigenic preparation but different adjuvants were tested, the long-term immune response was much better in the vaccine with an enhanced adjuvant. This might become important if the COVID-19 pandemic persists for a longer period of time than expected (Lee et al., 2021; Strizova et al., 2021).
All traditional or classical platforms discussed thus far use well-established technology and pathways. These classical methods are used to develop many of the vaccines that we use today (Chakraborty et al., 2021; Strizova et al., 2021). Examples include
seasonal influenza (inactivated vaccine),
measles (live attenuated vaccine), and
hepatitis A (inactivated vaccine).
Next-Generation Vaccines
The next-generation or newer platforms include the use of viral vectors and nucleic acids (RNA or DNA; Chakraborty et al., 2021; Lee et al., 2021). The next-generation vaccines do not require the actual viral particle and are manufactured solely from the code or sequence of the antigenic viral proteins. In other words, the material present in the vaccine contains the protein-coding sequence. The introduction of the sequence into our bodies directs the biosynthesis within the cell and stimulates an immune response.
Live Attenuated Viral Vector
Live viral vector vaccines use a modified version of a different virus as a vector to deliver payload in the form of instructions to the cell. The instructions are in the form of genetic material (a gene sequence) to a cell. The vaccine does not cause infection with either COVID-19 or the virus that is used as a cell delivery mechanism, because the live viral vector is attenuated. Scientists have learned how to create this genetic material in a lab. With regard to COVID-19, the code they deliver is the sequence of a location on the COVID-19 genome. By delivering this sequence to the cell, the cell can then learn to recognize the COVID-19 sequence and mount an immune response to that snippet of sequence. Although this type of vaccine can induce strong cellular and humoral response, there is a risk of inflammatory adverse reactions. If not properly attenuated, there is a potential risk of infection (Chakraborty et al., 2021; Karpiński et al., 2021).
On February 27, 2021, the U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the Janssen COVID-19 (Ad.26.COV2.S) vaccine, and this became the third vaccine approved for the U.S. market (Oliver et al., 2021). This vaccine is a single-dose recombinant, replication-incompetent adenovirus serotype 26 (Ad26) vector vaccine, encoding the stabilized prefusion spike glycoprotein of COVID-19. This is the first viral vector vaccine for COVID-19 in the United States. Because the adenovirus is replication-incompetent, it is considered safe; so the Advisory Committee on Immunization Practices issued an interim recommendation for use of the Janssen COVID-19 vaccine in persons aged ≥18 years for the prevention of COVID-19 1 day after the FDA gave the green light for EUA (Lee et al., 2021; Oliver et al., 2021). In April 2021, the FDA Advisory Committee reconvened to pause the vaccine due to six rare and life-threatening cases of cerebral venous sinus thrombosis correlated to the vaccine. After investigation, the Centers for Disease Control and Prevention (CDC, 2021a) recommended the use of the Janssen COVID-19 vaccine to resume.
Nucleic Acids (mRNA or DNA)
DNA vaccine technology involves the direct introduction of plasmid DNA, usually of bacterial origin. The plasmid DNA contains the gene encoding the specific antigen that is able to elicit an immune response. In this case, the antigen is usually a part of the spike protein of COVID-19. Because these vaccines use plasmid to introduce the DNA sequence, they are referred to as plasmid DNA vaccines (Strizova et al., 2021). One advantage of this type of nucleic acid DNA vaccine is it can be stored and delivered efficiently without a cold chain. DNA vaccines do not generate antivector immunity since they do not require a viral vector. They also do not cause off-target acquired immunity to DNA in the recipient of the vaccine. The bacterial plasmid that is used to deliver the sequence may require biocontainment safety procedures, but it is relatively easy to manufacture (Chakraborty et al., 2021; Fomsgaard & Liu, 2021; Lee et al., 2021; World Health Organization, 2020).
Messenger ribonucleic acid (mRNA) is a single-stranded molecule of RNA that corresponds to the genetic sequence of a gene and is read by a ribosome in the process of synthesizing a protein. It is the only biological molecule that can recapitulate, on its own, all the characteristics of life. It has been used in vaccine development in the past, just not in a man-made synthetic form. Live attenuated mRNA has been given in the mumps, measles, and rubella (MMR) vaccine by delivering live attenuated vaccine with mRNA in its natural state within the attenuated viruses. Now scientists have learned to synthesize mRNA, so we do not need to take the risk of handling live COVID-19. Synthesized mRNA vaccine technology or nucleoside-modified messenger RNA (modRNA) appears to be the most promising way to counteract emerging infectious diseases (Pascolo, 2021; Roncati & Corsi, 2021).
By using modRNA, it is possible to bypass the transcription process directly. The modRNA or mRNA can start the translation phase to produce the target protein inside human cells and stimulate the adaptive immune response to the spike protein on COVID-19. It is not necessary for the mRNA to enter the cell nucleus. The advantages of mRNA vaccine are they have no risk of infection for recipients or manufacturers from the COVID-19 or from a viral vector. Also, mRNA vaccine evokes both humoral and cellular immunity. Although mRNA is better in many ways, it is more fragile at room temperature, which requires cold-chain distribution. To remedy the issue with cold-chain storage, a thermostable mRNA vaccine has been developed. Because of easy degradation by ribonucleases, it is incorporated into PEGylated (PEG = polyethylene glycol) lipid nanoparticles. PEGylated nanoparticles are used in other medications and have been known to trigger hypersensitivity reactions (Roncati & Corsi, 2021).
In December 2020, the U.S. FDA issued an EUA to allow Pfizer–BioNTech–Fosun to begin distribution of the two-dose injection Comirnaty, the first modRNA vaccine in the United States. On December 18, 2020, the Moderna COVID-19 vaccine (code name: mRNA-1273) also received emergency authorization by the U.S. FDA, which is also a two-dose injection. It is the first time in history that a vaccine has been developed in less than 1 year from the description of an emerging infectious disease through the release of the COVID-19 genome sequence in January 2020 to EUA approval in December 2020. The rapid release of both mRNA vaccines was made possible by careful planning of every stage of vaccine development. Rapid development was made possible by financial investment upfront so that all the required trial phases could be completed in record time. For more discussion regarding the development of mRNA vaccines, refer to our previous article (Gordon et al., 2021). The mRNA technology is the golden child of science because the methods used to develop the vaccine are applicable to the development of other disease therapies in the future. Table 2 provides a summary of the characteristics of classical and next-generation vaccines with examples.
Characteristics of Vaccine Platforms With Examples
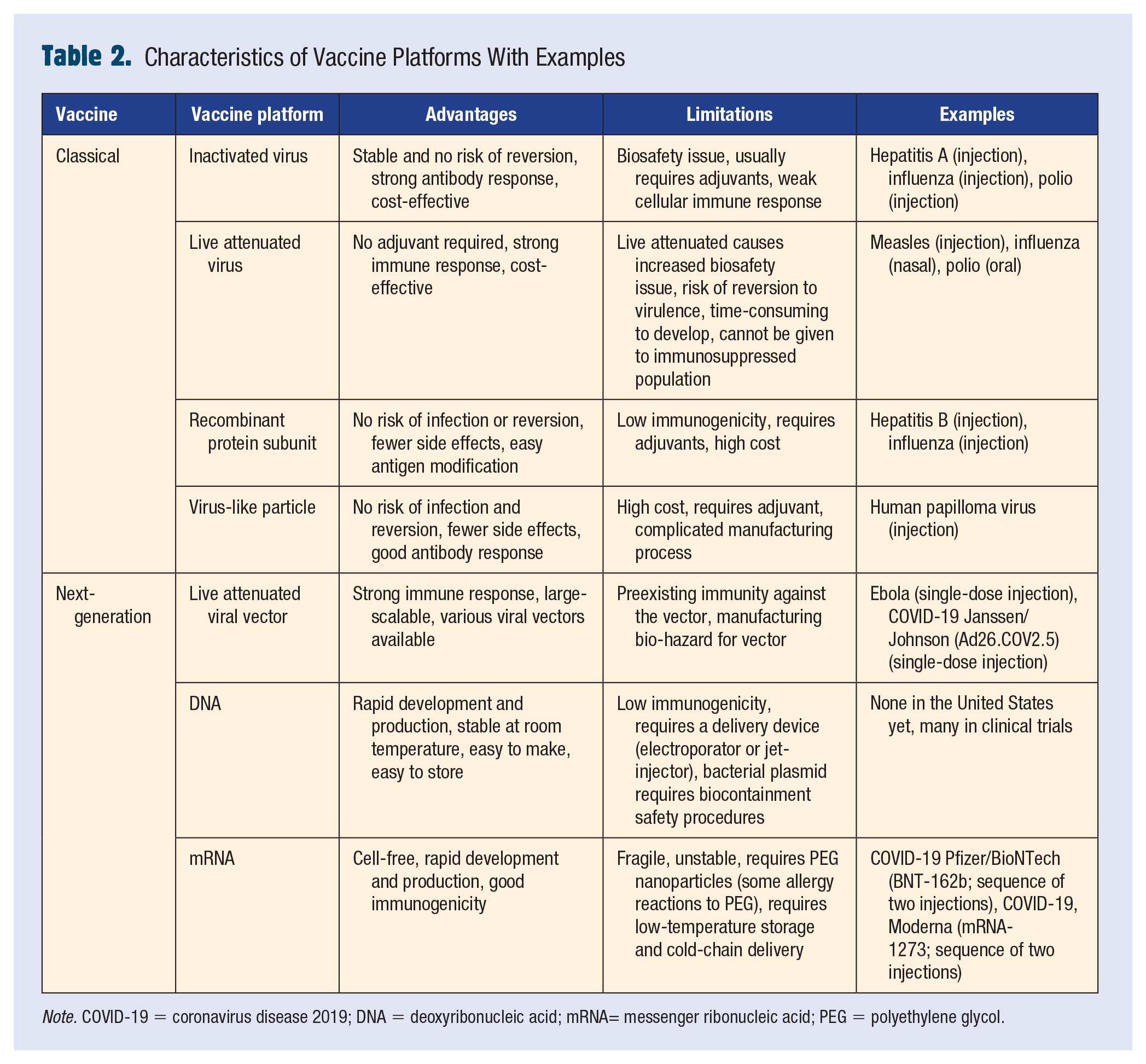
Note. COVID-19 = coronavirus disease 2019; DNA = deoxyribonucleic acid; mRNA= messenger ribonucleic acid; PEG = polyethylene glycol.
Non-COVID-19 Vaccinations Yield Trained Immunity
A recent study at Mayo clinic found that recent vaccination for polio, HIB (hemophilus influenza type B), MMR, varicella, PCV13 (pneumococcal conjugate), geriatric flu, and hepatitis A/hepatitis B lowers the rates of COVID-19 infection. The study included 137,037 individuals who received COVID-19 polymerase chain reaction tests. Through stratified analysis, the researchers also found significantly lower COVID-19 rates among Black individuals who had recently taken the PCV13 vaccine (Pawlowski et al., 2021). A retrospective single-center cohort review at the University of Florida healthcare system found that individuals who tested positive for COVID-19 and had not received the influenza vaccine had a 3.29 greater odds of intensive care unit admission when compared with those who were vaccinated for influenza. Apparently, giving the influenza vaccine decreased morbidity and mortality not only from flu but also from moderate to severe COVID-19. These studies suggest that patients who have been vaccinated may have a more “primed” pool of natural killer cells (Yang et al., 2021).
Universal Vaccine
If COVID-19 mutations continue, and the present vaccines do not change, eventually the vaccines will fail (CDC, 2021g). So, how can scientists create a “failure proof” vaccine? Scientists must target an area the virus cannot mutate (Böttcher & Nagler, 2021; Lawton, 2021). When an antibody binds to a protein, it is not binding to the full length of the protein. Instead, it is binding to a segment of that protein known as an epitope. Sharmin and Islam (2014) found an epitope utilizing directed RNA polymerase protein called WDYPKCDRA that is highly immunogenic and 100% conserved among all available human coronavirus strains. Highly conserved regions of the COVID-19 genome are areas that are essential for the survival of the virus, so these areas are less likely to mutate with success. Targeting a highly conserved region, or epitope, that is immunogenic could provide protection against all coronaviruses. If successful, this targeting strategy to a mutation reluctant epitope would allow scientists to create a “universal vaccine” for all coronaviruses (Sarwar et al., 2020; Sharmin & Islam, 2014).
Yuan et al. (2020) also found a conserved cryptic epitope in the receptor-binding domains of the COVID-19 viral genome by analyzing the crystal structure of CR3022. CR3022 is a neutralizing antibody previously isolated from a convalescent severe acute respiratory syndrome (SARS) patient. Clearly, monitoring novel sequence divergence is very important in the development of effective COVID-19 vaccines and potentially a universal vaccine for all coronaviruses in the future (CDC, 2021g; Lawton, 2021). This coronavirus outbreak continues to pose an enormous global risk, and scientists are racing to find conserved epitopes that can guide a structure-based vaccine design (Majid et al., 2021; Sharmin & Islam, 2014; Yuan et al., 2020).
Connections to the Framework
As the development of effective COVID-19 vaccines continues, school nurses will provide information and education to administrators, faculty, staff, students, and caregivers to encourage vaccination and transition the populace to herd immunity. As trusted frontline community providers, school nurses have a rich history of planning and providing vaccination clinics in schools (Park et al., 2021). In conjunction with the NASN’s Framework for 21st Century School Nursing Practice (NASN, 2016), the school nurse’s role in explaining vaccinations, advocating for vaccination, and planning and providing vaccinations relates to the Framework’s Community/Public Health principle with a focus on the risk reduction component. In addition, school nurses participate in health and wellness data collection and dissemination, which includes vaccination statistics, to support public health data collection and research under the Framework’s Quality Improvement principle. Last, school nurses practice nursing using evidence-based practice, including evidence for vaccination, under the Framework’s Standards of Practice principle.
Key Things to Know
COVID-19 vaccines are safe and effective (CDC, 2021b).
You may have side effects after vaccination, but these are normal (CDC, 2021f).
It typically takes 2 weeks after vaccination for the body to build protection (immunity) against the virus that causes COVID-19. You are not fully vaccinated until 2 weeks after the second dose of a two-dose vaccine or 2 weeks after a one-dose vaccine.
COVID-19 vaccines are more widely accessible. Everyone 16 years and older is now eligible for a COVID-19 vaccination (CDC, 2021c).
People who have been fully vaccinated can start to do some things that they had stopped doing because of the pandemic (CDC, 2021h).
COVID-19 vaccines will not alter your DNA; understand the myths and facts surrounding the vaccines (CDC, 2021e).
Discuss the COVID-19 vaccines with your friends and family using empathy, open-ended questions, concern, and advocacy (CDC, 2021d).
Equipped with this knowledge of vaccine strategy, the school nurse can more aptly educate and advocate for the use of the COVID-19 vaccines to move toward herd immunity in their communities.
In Summary
There is historical evidence that pandemics have devastated populations throughout the world in the past, and it will certainly happen again in the future (Makarov et al., 2020; Stefano, 2021). Pandemics are not new events, and neither are the aftereffects of a pandemic, such as COVID-19, “long-hauler” syndrome. There is documented historical evidence that the “Russian influenza” epidemic that started in St. Petersburg in 1889 also caused similar longer term symptoms of “neuralgia, neurasthenia, neuritis, and nerve exhaustion” (Honigsbaum & Krishnan, 2020). Global warming and close contact between humans and animal vectors will cause crossovers of a zoonotic disease (Yokota et al., 2021). The progress that has been made in vaccine development, implementation of sound public health strategy, and an empowering agency that will utilize scientific evidence to protect the public have raised hope for the American people and the world. Equipped with this new knowledge of vaccine strategy, the school nurse can more aptly advocate for the use of the COVID-19 vaccines to move toward herd immunity in their communities. ■
Footnotes
Elizabeth is a clinical associate professor at the University of Alabama in Huntsville, College of Nursing. Elizabeth serves as a nurse practitioner at a local primary care practice.
Mark is a clinical associate professor as well as the RN-BSN and Dual Nursing Programs Coordinator at the University of Alabama in Huntsville, College of Nursing.
Jenny has been a pediatric registered nurse for more than 20 years. Jenny is currently enrolled in the Family Nurse Practitioner Program at the University of Alabama in Huntsville, College of Nursing.