
Abstract
The ongoing COVID-19 pandemic has been taxing to healthcare workers, no less for those serving on the front lines in schools. From initial school closures and online learning to gradual reopening with hybrid learning models, to full in-person learning, school nurse administrators provided guidance in collaboration with public health officials, based on evolving information. Infection control was at the forefront, while government and scientists partnered to quickly develop effective vaccines. Technology provided new virtual platforms for learning, conducting meetings, and socialization, while also being widely used to deliver information, misinformation, and disinformation. Challenges have been numerous, but school nurse administrators and school nurses in general, with a commitment to the health and safety of their populations, continue to adapt to the ever-changing demands. The journal’s Editorial Advisory Board interviewed five school nurse administrators, representative of diverse geographic locations, school population size, and employer models, to capture their reflections on school health leadership during the COVID-19 pandemic. History is deserving of their stories.
Keywords
In their article detailing pandemics throughout history, Piret and Boivin (2021) provide a table listing a timeline of pandemics. Our current pandemic, SARS-CoV-2, initially identified in Wuhan, China in December of 2019, thus commonly named COVID-19, was the fourth of this current century preceded by severe acute respiratory syndrome (SARS-CoV; 2002-2003), swine flu (H1N1; 2009-2010), and Middle East respiratory syndrome (MERS; 2015-ongoing). School nurses recall the H1N1 pandemic, and a past NASN School Nurse article highlights the crucial role of the school nurse, where early in the pandemic, Mary Pappas (2011) alerted health officials in New York City of an outbreak of symptoms occurring in her school. Carolyn Duff, past president of NASN, explains “the possibility of a pandemic is always on school nurses’ radar screens” (2020, p. 48), and she goes on to elaborate on a school nurse’s ability to be flexible with a pandemic response plan that is “reactive to new evidence and adaptive to new practice environments” (p. 48). Duff also reminds that enlistment of the Leadership principle from NASN’s Framework for 21st Century School Nursing™ (National Association of School Nurses, 2016) is central to school nurse pandemic response, as well as the Framework’s focus on the safety and health of students.
The Editorial Advisory Board (EAB) of the NASN School Nurse desired to capture and preserve for historical purposes, a description of the challenges and successes of school nurse leadership during the COVID-19 pandemic, hereafter referred to as COVID. More simply stated, we wanted to create a platform for school nurse administrators (SNAs) to tell their story. An invitation was placed on NASN’s SchoolNurseNet SNA discussion list in November 2021 specifying that participants must spend a minimum of 50% of their time in a managerial role and that they supervise a minimum of 10 school nurses. Over 40 SNAs responded to the invitation. Restrictions of article length required narrowing down the participants, and the EAB focused on diversity of geographical representation, student population size, and employment agency type. An online, supplemental file provides acknowledgements and photos of the SNA participants. Table 1 provides additional information, including the SNA name, job title, school name, demographics, and school health staffing.
School Demographics and Staffing (Largest to Smallest Student Population)
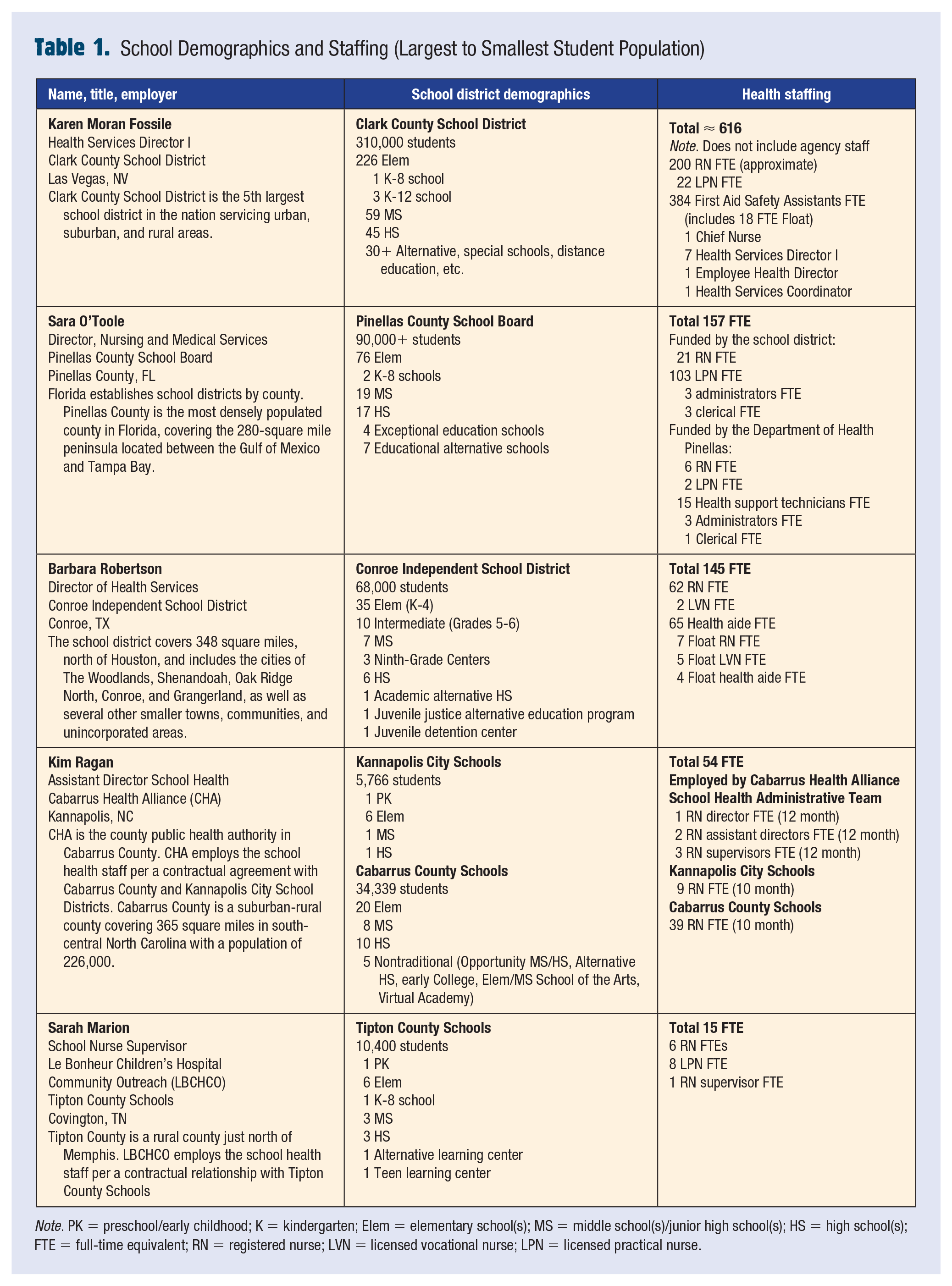
Note. PK = preschool/early childhood; K = kindergarten; Elem = elementary school(s); MS = middle school(s)/junior high school(s); HS = high school(s); FTE = full-time equivalent; RN = registered nurse; LVN = licensed vocational nurse; LPN = licensed practical nurse.
In addition to demographic and school health staffing data, participants were asked five questions. Interestingly, the participants submitted their responses late 2021 through early 2022, coinciding with the third wave of the pandemic. The EAB is thankful for all of those who expressed an interest in sharing their stories, and we encourage SNAs to take time to answer these questions for your community, and in so doing capture the historical significance of school nursing during this remarkable time in history.
1.
staff at schools including school nurses, specialized procedure nurses, and contracted agency nurses,
several committees (Policy and Procedure, School Nurse Advisory Board, Employee Engagement Committee) with in-person meetings once per month, and
First Aid Safety Assistant training and New School Nurse training.
In addition, I participated in nurse administration meetings every other week and assisted with interviews of school nurse candidates and agency nurses (three separate agencies). Some of the rural schools were reopened in a hybrid model (three elementary schools, one middle school, and one high school) in August of 2020, while the rest of our school district remained closed providing distance education. Parents of students at the three rural schools were asked to review health symptoms confirming their child was free of symptoms prior to the student entering the building each day. We began holding virtual meetings to determine who needed to be quarantined on confirmation of a COVID positive student or staff member. All of our committee meetings remained virtual.
In March 2021, all elementary schools reopened in a hybrid model, with half the students attending Mondays and Tuesdays, the other half attending Thursdays and Fridays, and Wednesdays reserved for cleaning. Parents and guardians also had the option to keep their child in distance education. In April 2021, all elementary schools converted to a typical 5-day model, and secondary schools reopened in the hybrid model in order to social distance due to space. Each school was required to have both a sick and well room, and all sick and well rooms were supplied with ionization filter systems. All nurses were Fit-tested for N95 masks following Occupational Safety and Health Administration guidelines, as well as the First Aid Safety Assistant at each school and at least two health office backups. We interviewed and hired many agency nurses placing them at schools to assist in the sick rooms. Following guidance from our local health department, we developed policies and procedures to guide the transition to full in-person learning. There were many facets of this process:
Additional hours were devoted to training, coordination of services, meetings, contact tracing, data collection, and staff education.
Staff education involved explaining the three points of service for delivery of first aid or medications.
° First point of service was the classroom—complete Basic First Aid in the classroom with consideration if medication can be given in the classroom or right outside in the hall.
° Second point of service was the well room or health office for completion of diabetes management.
° The third point of service was the sick room where students exhibiting signs and symptoms of COVID-19 were sent for evaluation.
We established a triage form for questions to consider when sending a student to the sick or well room. This included a phone call being placed to an established person who advised the teacher on which room to send the student.
The regular school year ended on May 26, 2021; however, on June 1, 2021, every school offered June acceleration programs using COVID-related Elementary and Secondary School Emergency Relief Funds. Most of our school nurses were not on contract. Thus, we needed to offer incentives to work the month of June. Further complicating the strain on our work force, our Extended School Year Program started on July 1, 2021, running through July 27, 2021. With new school nurses reporting on July 28, 2021, and the returning school nurses starting back on August 4, 2021, there was no break for planning or respite for the nursing administrators prior to students beginning classes on August 9, 2021.
We started the 2021-2022 school year with COVID and contact tracing as our major responsibilities. As administrators, we also covered Saturdays and Sundays for isolation and quarantine calls and were working 50 to 60 hours per week. We were not able to perform any other duties but COVID-related activities. Virtual meetings were set in 15-minute increments, and some days that is what you did almost the entire day. It was exhausting. Mandatory vison and hearing screening was halted at this time.
Once school opened in August 2020, the pace seemed to level out until early November. In early November 2020, we noticed a steady increase in COVID positive cases in the district and community. This increase continued throughout the winter holidays and January 2021, which again meant working long hours on the contact tracing process with the health department. I oversaw the daily reports of positive cases in the district, which were reported to both district leadership and the public. Beginning in February 2021, the case count began to slowly decrease, and levelled out by early March. We saw a slight increase after spring break, but cases then declined until the end of the school year.
COVID cases were low over the summer, and we were hopeful going into the opening of the 2021-2022 school year—then Delta hit. With the arrival of the Delta variant, we once again experienced a huge spike in cases, and opened the school year much like the 2020-2021 school year, with almost the same challenges as previous, but all students now attended in person. August and September 2021 were challenging months, as the State of Florida enacted some rules that directly affected contact tracing and quarantine in schools.
I was fortunate to be a part of our district’s medical advisory team . . . comprised of the county health department director, the head of our local children’s hospital Infectious Disease Department, the medical director for our local Federally Qualified Health Center, local pediatricians, and school district leadership. (Sara O’Toole)
As we returned to school fall of 2021, we were quickly inundated with the Delta variant. COVID fatigue, vaccine hesitancy, and optional mask usage contributed to unprecedented case counts and pushed our nurses to the brink of exhaustion. Between managing our COVID response with my departmental duties, my workload once again returned to 12+ hours per day. After a couple of very difficult months, by late November 2021 we began experiencing some of our lowest case counts in more than a year. With the reduction in COVID-related issues, we were able to refocus our energies on student screenings for vision, hearing, and spinal, provide professional learning opportunities for our nurses, as well as give nurses a chance to catch their breath and prepare for whatever may come their way the remainder of the 2021-2022 school year. I remain confident we will be ready.
By midyear, I was working more hours as the schools moved to A/B hybrid learning necessitating additional training and weekly virtual meetings to keep the school nurses current on all things COVID; to assist our administration team with interviewing, hiring, and orienting new school nurses; and to keep parent letters and educational materials updated to reflect the current public health guidance. I also had to help cover schools during a temporary nurse vacancy and leave. In addition, I fielded frequent questions from the nurses, parents, and school staff regarding COVID via phone and emails; worked large, community-based, drive-through COVID vaccine clinics at an area event center; and coordinated the pilot program for rapid antigen testing in select schools which included ordering and delivering testing supplies and developing and conducting training sessions for the nurses. I also aggregated school-based testing data to share during the weekly school leaders’ meetings. The administrative team was very busy with “all things COVID.” We were trying to stay abreast of current COVID guidance, keeping our school nurses updated on the changes, trying to acknowledge and validate their fears while promoting multilayered mitigation strategies to help keep them safe, and providing the nurses a safe space to express their frustrations and concerns as they were often caught between public opinion and enforcing the public health guidelines.
By the end of the 2020-2021 school year, the students were back to 100% in-person learning, community vaccine clinics were being held 2 to 3 times per week, the number of calls and emails increased, and the weekly meetings continued. We thought that if we could just make it through the school year our team would finally get a chance to rest and recover, and then we learned about the second chance summer school programs.
As administrators, we also covered Saturdays and Sundays for isolation and quarantine calls and were working 50-60 hours per week. We were not able to perform any other duties but COVID-related activities. Virtual meetings were set in 15-minute increments, and some days that is what you did almost the entire day. It was exhausting. (Karen Moran Fossile)
By midyear, our processes were in place and my focus transitioned to data collection and staffing challenges. I spent around 8 hours a week organizing the data being sent in by the school nurses. We had several staffing challenges both COVID-related and unrelated. This led to direct patient care dominating my time for much of the winter months. By the end of the school year, COVID cases had dropped in our area. We were able to complete our end-of-year duties much like other “normal” school years.
The beginning of the 2021-2022 school year was similar to the beginning of the prior school year in that once again procedures were changing, and I was again researching, planning, and updating procedures to correspond to new data and guidelines.
Looking back, I would be more intentional about staying ahead of the curve on the constantly changing COVID guidance and providing a safe platform for each of my direct report nurses to vent and express their concerns without fear of judgement. (Kim Ragan) Many times, it felt like we would put a practice in place and the next day guidelines would change, specifically regarding quarantine management. (Sarah Marion)
We found virtual options were not as conducive to learning for instruction on skills such as the screening training or when delivering a large amount of critical content. (Barbara Robertson)
Looking back, we should have centralized Covid operations before the start of the 2021-2022 school year to reduce the burden and stress on our schools. (Karen Moran Fossile) I think that the biggest challenge I have faced throughout this pandemic was finding my voice and using it to provide truth and facts even with other people who have different opinions. (Sara O’Toole)
Regarding health screenings, our district has been fortunate to have a screening team that has conducted our mandatory screenings. The 2020-2021 school year was challenging, as we had students learning in-person but also students learning virtually. Students were allowed to return to brick-and-mortar school at any time last year. As a team, we looked at the in-person enrollment numbers in every school and used the screening team where they would have the most impact—the schools with larger numbers of in-person students. We tweaked our screening procedures to ensure social distancing and safety. We spent more time at the larger schools so not to rush through the students and to prevent students congregating together for long periods of time. For smaller schools, who did not receive the screening team, the school nurses oversaw the screenings, completing them at their own pace and spreading the screenings out over the course of many months.
Rather than a challenge to be solved, this professional duty requires ongoing flexibility, adaptability, and relevant knowledge to make the best decisions possible. While working closely with our local healthcare entities and health department, I also collaborate with my nurse advisory team and local nurse leader colleagues, stay abreast of ever-changing guidance, and use current resources provided by Texas School Nurses Organization (TSNO) and NASN. An outstanding team of administrators supports me, so I am never alone in my efforts to protect our students, employees, and communities.
If I could do anything different, it would probably be to make myself take more time for a break from trying to protect everyone. As nurses, we often give all we have to help our patients, which can leave nothing in reserve, mentally or physically, for ourselves. I am working on acknowledging this and taking steps to care for myself so I can continue to care for others.
During the 2020-2021 school year, we placed a priority on vision screenings for students in the required grades. After weathering the increased COVID cases in the fall semester, our nurses worked tirelessly to conduct screenings in a safe manner and identify students who needed referrals and/or assistance prior to the end of the school year. This current school year, 2021-2022, we are well on our way to meeting our goal of completing vision and hearing screenings for all required grades along with those who may have been missed last school year. Additionally, this school year, our district provided each nurse with a one-year membership to NASN, which will not only support their nursing practice but also make available the VSP Global Sight for Students gift certificates, so they can provide vision assistance for their students in need.
If I could do anything different, it would probably be to make myself take more time for a break from trying to protect everyone. (Barbara Robertson)
Looking back, I would be more intentional about staying ahead of the curve on the constantly changing COVID guidance and providing a safe platform for each of my direct report nurses to vent and express their concerns without fear of judgement. Regarding preventive screenings, our nurses did not conduct mass screenings during the 2020-2021 school year. They conducted hearing and vision screenings for evaluations and as concerns were presented.
Our state suspended mandatory health screenings for the 2020-2021 year, instead making them recommended. When COVID cases decreased toward the end of the second semester, I was able to take a few days to visit each school to assist with as many screenings as we could complete. While we did not have time to complete as many as previous years, we were still able to screen several grades during a year with so many other added responsibilities.
They took every change in stride, helped us figure out better ways to work, advocated for themselves and their students, and provided a calm voice of reason for so many of our families and staff. (Sara O’Toole) . . . we were able to implement . . . protocols which prevented any major COVID outbreaks within the school system. We did not have to close down any schools during the 2020-2021 school year . . . (Sarah Marion) I am most proud of how our School Nurse team stepped up to the COVID challenge and being part of hundreds of staff and volunteers working long hours, during all types of weather, to hold large scale vaccine clinics, having fun, with smiles on our faces, and working collaboratively with multidisciplinary teams, and developing new relationships with community partners. (Kim Ragan) Telling people what to do is easy, leading people is harder. . . . Our district has shown that together we can do hard things well. (Barbara Robertson)
Conclusion
There is no doubt that the pandemic thrust school nursing into the spotlight. Initially, when schools were closed to slow the spread of disease, school nurses served as navigators between public health and education institutions to assist in establishing and implementing mitigating factors, magnifying both the role and workload of SNAs and school nurses. Additionally, SNAs and school nurses demonstrated an ability to quickly pivot as they responded to ongoing, evolving information, all the while assisting the school community in deciphering between factual and nonfactual information. Public health measures were at times met with resistance, more so as the pandemic lengthened in time from weeks to months, then to years. Thank you SNAs and school nurses for your commitment in promoting the health of our students, staff, and communities. We encourage all of you to take the time to tell your story. It is a story of challenges, collaboration, respect, resiliency, trust, and passion.■
Supplemental Material
sj-pdf-1-nas-10.1177_1942602X221084069 – Supplemental material for Leading During a Pandemic: A School Nurse Administrator Roundtable
Supplemental material, sj-pdf-1-nas-10.1177_1942602X221084069 for Leading During a Pandemic: A School Nurse Administrator Roundtable by Cynthia A. Galemore, Sarah Marion, Karen Moran Fossile, Sara O’Toole, Kim Ragan and Barbara Robertson in NASN School Nurse
Footnotes
Supplemental Material
Supplemental material for this article is available online.
Cynthia served as the Director of Health Services for Olathe Public Schools from 1995 until her retirement in 2017. Cynthia is a former NASN Director and has served as the editor of the journal since 2010.
Sarah is a nurse supervisor for Le Bonheur Children’s Hospital Community Outreach, working in the Tipton County School system. Her first profession was teaching before she made the switch to nursing. She began her nursing career at the children’s hospital before transitioning to the hospital’s community division to merge her professions as a school nurse.
Karen has 17 years of school nursing experience in the Clark County School District in Las Vegas. Since 2013, she has been part of the Nursing Administration overseeing about 35 school nurses and 60 schools. Karen began her nursing career in Philadelphia working at St. Christopher’s Hospital for Children for 22 years in various roles from staff nurse to management.
Sara has worked at Pinellas County Schools for 11 years, first as a school nurse then in administration for the past 8 years. She is a member of the Florida Association of School Nurses and has collaborated with the State of Florida on various school nursing projects and initiatives.
Kim has 25 years of school nurse experience having worked in North Carolina, Minnesota, and Grand Cayman, British West Indies. For the past 17 years, she has worked in Cabarrus County as a member of the School Health Administrative team at the Cabarrus Health Alliance (CHA). CHA is the county public health authority providing school nurse services to 40,000+ students in the county’s two public school districts. She is currently a Master’s in Public Health Leadership candidate at the University of North Carolina at Chapel Hill. As a public health nurse Kim works as a liaison between the Local Education Agencies and the Public Health COVID department.
Barbara has worked in Conroe ISD for 17 years, 10 years as a school nurse, and the past 7 years in administration as Coordinator and now Director of Health Services. She is an active member of the Greater Houston Area School Nurse Leadership Group where she collaborates with area school nurse administrators on best practices for student health and safety.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.