
Abstract
School nurses are often the forward-facing health care practitioner for youth, simultaneously managing mental health and medical care for their students while also interacting with students’ families and navigating consequences of family dynamics, including health literacy, social support, and financial issues. Thus, it makes sense to train school nurses on how to best interact with and support adolescents diagnosed on the autism spectrum. Part one of this three-part series will include an overview of mental health diagnoses often co-occurring with autism, associated challenges for the autistic adolescent, and school nurse interventions that may be helpful. The second and third part of the series will address the medical health diagnoses, nursing interventions, and overall discussion on how to best care for autistic adolescents in the schools.
Keywords
Autism spectrum disorder (ASD) is characterized by persistent differences in social communication and behavior and repetitive patterns of behavior, interests, or activities, but co-occurring mental health diagnoses are also more common for adolescents with ASD than their non-ASD peers. These most frequently include attention deficit/hyperactivity disorder (ADHD) and mood disorders, such as anxiety and depression (Brookman-Frazee et al., 2018; Lai et al., 2019; Valicenti-McDermott et al., 2023). Challenges with daily functioning and social inclusion can impact the severity and prognosis of co-occurring mental health conditions for adolescents with autism, and targeted support in these areas will facilitate their overall well-being (McMaughan et al., 2023). Because autistic youth may not respond to mental health treatments in the same way as other youth, practitioners working with this population are most effective when possessing specialized knowledge of ASD. Moreover, learning the unique strengths, challenges, temperaments, and diagnostic profiles of individual students is necessary for implementing trauma-informed, tailored intervention (Brookman-Frazee et al., 2018).
School nurses are often the forward-facing health care practitioner for youth, simultaneously managing mental health and medical care for their students while also interacting with students’ families and navigating consequences of family dynamics, including health literacy, social support, and financial issues. Part one of this three-part series will include an overview of mental health diagnoses often co-occurring with autism, associated challenges for the autistic adolescent, and school nurse interventions that may be helpful. The second and third part of the series will address the medical health diagnoses, nursing interventions, and overall discussion on how to best care for autistic adolescents in the schools.
Changing Terminology
Terminology within the autism community continues to shift as autistic self-advocates, family members, clinicians, and researchers debate how language reflects identity, stigma, disability, and support needs. One debate involves the use of person-first language (e.g., “person with autism”) versus identity-first language (e.g., “autistic person”). Recent research suggests many autistic self-advocates increasingly prefer identity-first language because, like the deaf community, they view autism as an integral part of their identity and community belonging (Dwyer, 2022; Schuck et al., 2025; Smith et al., 2023; Taboas et al., 2023). Consequently, autism research and advocacy spaces have been increasingly shifting toward identity-first terminology (Zajic & Gudknecht, 2024). In contrast to self-advocates, many advocates and advocacy groups for those with autism and more intensive support needs continue to prefer person-first language, which emphasizes the individual beyond their disability.
Likewise, a growing controversy surrounds the diagnostic label of “autism spectrum disorder” and the proposed category of “profound autism.” Advocates and families of individuals with profound autism argue that the broad-spectrum framework obscures the needs of autistic people with co-occurring intellectual disabilities, minimal or no functional speech, and intensive lifelong support needs (Wiggins et al., 2026). As a result, some researchers and clinicians have advocated for a distinct diagnostic category to improve access to services, supports, and research attention focused on the unique needs of this population (Clarke et al., 2024; Wachtel et al., 2024; Wiggins et al., 2026).
Debates over terminology within the autism community reflect differences in the lived experiences of people with autism and within the broader autism community. School nurses should avoid making assumptions about preferred terminology and, instead, respectfully ask autistic students and their family members what language they prefer. Using an individual’s preferred terminology demonstrates cultural humility, supports collaborative relationships, and acknowledges the diversity of perspectives that exist across the autism community (Dwyer, 2022; Smith et al., 2023).
Common Challenges for Adolescents With Autism
Individuals with ASD may present a wide range of behaviors in healthcare settings that can vary depending on their cognitive profile, language abilities, sensory sensitivities, and level of support needs. Autism is defined by differences in social communication skills and restricted, repetitive behaviors, both of which can influence how patients respond to clinical environments and interactions (American Psychiatric Association, 2013). Social communication-related difficulties in autism are closely tied to differences in emotional and behavioral regulation and executive functioning (Demetriou et al., 2018). These challenges can influence how autistic patients respond to others in medical environments (R. Morris et al., 2019). For school nurses, understanding these underlying differences can support more accurate interpretation of student behavior and promote more compassionate care.
One common challenge for individuals with autism involves difficulty interpreting social cues and engaging in reciprocal conversation. Research indicates that many individuals with autism have difficulty reading facial expressions, tone of voice, and body language which are critical for understanding social intent and expectations (Che & Zhou, 2025). In interactions with autistic students who are verbally fluent and without intellectual disability, this may present as limited eye contact, atypical conversational patterns, difficulty initiating or maintaining conversation, or literal interpretation of questions. It is important to recognize that these behaviors are not indicative of disinterest or noncompliance but rather reflect divergent information processing styles and social interaction patterns as reported by adults with autism (Sterrett et al., 2024). For autistic students who are minimally verbal and/or have a co-occurring intellectual disability, healthcare encounters can be particularly challenging. These students may use nonverbal methods (e.g., gestures, facial expressions, behavior changes, or augmentative and alternative communication strategies) to express needs, discomfort, or pain. In a review of pain communication in children with autism, nonverbal behaviors differed substantially from those of neurotypical children, often leading to misinterpretation by clinicians who are unfamiliar with such presentations (Johnson et al., 2023). Recognizing these communication differences can reduce misinterpretation and frustration during school nurse interactions.
Across the spectrum of autism, students may display self-stimulatory behaviors (“stimming”) such as hand flapping, rocking, pacing, tapping, or repetitive vocalizations during stressful or sensory-intensive situations. These repetitive behaviors are part of the core diagnostic criteria of autism and serve important self-regulatory functions, helping individuals manage sensory input, anxiety, or overwhelming environmental stimuli (I. F. Morris et al., 2025). Rather than viewing all repetitive behaviors as disruptive, it is clinically valuable to recognize that stimming can increase self-efficacy and coping under stress (e.g., being unable to stim during an exam may reduce a patient’s ability to manage anxiety and behavior). Listening to families and caregivers about the meaning of specific stimming behaviors and communication attempts is essential as families often have deep insight into what a particular stim indicates (e.g., excitement, stress, pain, boredom). Without this contextual knowledge, school nurses may misinterpret these behaviors as disruptive and noncompliant.
Emotional and behavioral challenges further influence social experiences for autistic individuals, particularly in unfamiliar and stressful environments such as hospitals, clinics, and school nurse offices. In these settings, they may struggle to identify others’ emotional cues or to regulate their own emotional responses which can lead to withdrawal, emotional distress, and behavioral escalation (Cai et al., 2018). Nurses may observe that autistic students become overstimulated in environments where social and sensory demands are high, such as waiting areas or shared clinic spaces. Understanding these student behaviors can help school nurses respond with greater sensitivity and empathy and anticipate situations that may increase distress.
Autistic individuals also experience challenges with executive function that frequently impact their behavior and social communication (Demetriou et al., 2018). Executive functions, such as planning, working memory, cognitive flexibility, and inhibitory control, are essential for navigating dynamic social situations such as those common in healthcare settings (Demetriou et al., 2018). In school healthcare settings, these challenges may appear as difficulty shifting attention, challenges with following multistep directions, difficulty remembering detailed information about their medical history, or lack of impulse control during interactions with family and staff. When viewed through this lens, behaviors that may otherwise appear purposefully oppositional or inattentive can be understood as neurologically based differences in executive function and support trauma-informed, patient-centered nursing care.
Attention Deficit/Hyperactivity Disorder
Scientific understanding of how ASD and ADHD co-occur is still evolving, with brain research suggesting that their co-occurrence (sometimes informally referred to as AuDHD, a combination of “Autism” and “ADHD”) may be a distinct disorder with more significant impairments than either diagnosis alone (Chantiluke et al., 2014; Yerys et al., 2009). However, ASD and ADHD are currently listed as distinct neurodevelopmental disorders in the Diagnostic and Statistical Manual of Mental Disorders, revised 5th edition (DSM-5; American Psychiatric Association, 2022) associated, in part, with executive functioning challenges that may present as limited ability to plan and complete tasks, to switch between tasks, and inhibit behavioral impulses. While ASD is typically diagnosed in early childhood, ADHD often goes undiagnosed until more restrictive and demanding educational environments are encountered (Hours et al., 2022). Most adolescents diagnosed with ASD will also be diagnosed with ADHD, although the same is not true for those originally diagnosed with ADHD (). Identifying and treating ADHD in individuals with ASD is critical because pharmacological and behavioral interventions have been successful in treating ADHD and can provide significant relief for some symptoms and challenging behaviors. Still, a clinician’s nuanced understanding of the patient’s diagnostic profile is necessary because not all symptoms overlap, and some ASD-related symptoms are worsened by stimulant medications prescribed for ADHD.
Behavioral interventions for executive functioning (EF) issues are most effective when customized to symptoms and unique underlying causes. For example, an adolescent with a primary ASD diagnosis may present with selective attention resulting in hyperfocus, whereas an adolescent with a primary ADHD diagnosis may present with limited capacity for focus (Hours et al., 2022). Both students may find it challenging to pay attention in a classroom setting, but with dissimilar origins. Regardless of formal diagnoses, many EF challenges in an educational setting can be treated with external aids, modifications to the environment, and/or academic accommodations. Adolescents with EF challenges may benefit from external aids such as checklists, calendars, and alarms. Moreover, restructuring the classroom environment with alternative seating or movement options during classroom activities or test-taking, as well as extended time for test-taking, can make a significant difference in student success. Adolescents with ASD, along with their guardians/caregivers, have noted that their capacity for EF can vary widely depending on context, motivation, and level of anxiety regarding the skill. Thus, given that a student’s EF capacity can be highly nuanced, student and parental input is necessary for effective intervention (Kenny et al., 2024). It is important to note that the gap in EF abilities between students with ASD and those without typically becomes most pronounced in adolescence when students are preparing to enter adulthood and task expectations become more salient (Rosenthal et al., 2013).
The school nurse should be included in an autistic adolescent’s individualized education program (IEP) conferences in collaboration with guardians/caregivers, teachers, administrators, school psychologists, etc., as this multidisciplinary approach is effective in properly managing care, especially when ADHD or other mental health disorders are co-occurring. IEP conferences present a school nurse with opportunities to ask questions about the student, including triggers, needs, coping skills, comorbidities, and medications. As stated above, ADHD in adolescents with autism can look very different than in an adolescent who does not have ASD. The most effective treatment plans will be personalized and can include a variety of medications. Within a multidisciplinary team, the school nurse is uniquely qualified to monitor behaviors, medication effectiveness, and side effects and can become central to consistent, effective care.
Mood Disorders
The common co-occurrence of mood disorders with ASD also requires attention, particularly as internalizing symptoms (such as anxiety and depression) can be both the cause and effect of challenging behaviors, functional limitations, and social isolation (McMaughan et al., 2023). For example, ASD-related sensory sensitivity may lead to a student’s limited capacity to rapidly switch tasks, and a demand to switch tasks may cause the student significant anxiety. If unaddressed, this anxiety can lead to increased emotion dysregulation and an emotional outburst, resulting in additional functional impairment, followed by even more anxiety and perhaps placement in a more restrictive and sensory-challenging environment and estrangement from their peers (Brookman-Frazee et al., 2018). Emotional outbursts indicate an unmet need that the adolescent is struggling to identify or communicate, and showing genuine interest in the student’s unmet need will go a long way in helping to assist them (Plumb, 2025). Effective intervention includes modeling emotion regulation and matching communication style, which often requires using direct language, asking direct questions, and allowing extra time for verbal processing. A student with ASD who is emotionally dysregulated will need time to self-soothe, as they will be too overstimulated to listen and respond. Reducing sensory stimulation by providing privacy and sensory tools, dimming the lights, or sitting in silence can be helpful. When the student is ready to communicate, they may prefer text messaging or visual imagery (Plumb, 2025). Following emotional outbursts, an adolescent with ASD may also experience depressive symptoms that present as aggression toward oneself or others and further feed into social and academic impairment (Gardiner & Iarocci, 2018; Hours et al., 2022).
The internalized nature of anxiety and depression presents a unique challenge for adolescents with ASD, many of whom struggle with internal body cues (interoception) and social communication. It may be difficult for a school nurse to identify whether an autistic student is experiencing irregular mood fluctuations when the student is already in a “world of their own” or speaks in monotone. Moreover, hormonal fluctuations naturally occurring during puberty can contribute to mood instability and irritability, and transitioning into adulthood can be especially anxiety-inducing for students with ASD who are often aware of their social and academic challenges. Internalizing symptoms such as anxiety and depression are generally associated with withdrawal, somatic issues, low self-esteem, negative thinking, and social difficulties (Joshi et al., 2010). Cognitive behavioral therapy can be helpful in challenging negative or self-defeating thoughts, though not as effective for some ASD youth as for their non-ASD peers (Brookman-Frazee et al., 2018). School staff can help a student with ASD increase body and emotion awareness by learning their unique triggers and self-soothing techniques, with the help of guardians and caregivers, and gently noting when the student displays physical cues to their emotional state, for example, frowning, clenched fists, extra stimming. Email or text templates or specific visual cues can be developed for the adolescent to use when struggling to communicate needs and practicing role-play scenarios can help the student build communication skills to advocate for themselves (Plumb, 2025).
With proper education, school nurses can recognize signs of stress and allow the autistic adolescent time to de-escalate in a private area. Being able to recognize these cues early is important in preventing a meltdown, especially in front of peers. The nurse’s office should be a safe and supportive place for a student with autism (Autism Speaks, 2025a). Allowing the student to tour the nurse’s office and other safe spaces at the beginning of each school year provides reassurance. School nurses can also build trust with the autistic student by allowing them regularly scheduled time in the nurse’s office, providing the student with undivided attention and a predictable environment in which they feel comfortable. Students with autism thrive with structure, so scheduling a regular time to meet with the student in private to communicate concerns will be beneficial. During these meetings, communication tools can aid clear communication and alleviate frustration. Adolescence is a challenging time for most teenagers because of a multitude of physical, emotional, and situational changes, and even more so for a person with autism. The neurodivergent characteristics of autism often make navigating these new circumstances and emotions even more challenging. Peer support is a protective factor, and the need for positive peer interaction in adolescence must not be overlooked. As with most adolescents, it is developmentally appropriate for autistic teenagers to want to form significant connections outside of their families of origin, but they often struggle to form skills or confidence to do so on their own (Autism Speaks, 2025a; Verkooijen et al., 2026).
Other Disorders
Significant symptoms overlap with mental health disorders and ASD has led to debate about whether some co-occurring disorders are distinct or merely part of a spectrum of symptoms. Co-diagnosis of ASD and obsessive-compulsive disorder (OCD) illustrates this debate and highlights the complexity and nuance of differential diagnosis. Whereas repetitive behaviors (stimming) can be self-soothing and even pleasurable for an adolescent with ASD, the type of repetitive behaviors associated with OCD, by definition, will cause the adolescent significant distress (Aymerich et al., 2024; Dell’Osso et al., 2024; Joshi et al., 2010). Similarly, whereas some youth with ASD may experience sensory overload and refuse to complete tasks, those diagnosed with oppositional defiance disorder have been deemed willfully hostile with malicious intent (Kildahl et al., 2021; Newson et al., 2003). In either case, as previously discussed, identifying the underlying cause of challenging behaviors and treating the symptoms allows for more trauma-informed and effective intervention (Brookman-Frazee et al, 2018).
Sleep disorders, such as insomnia, are also quite frequently co-diagnosed with ASD and have been bidirectionally linked to increased anxiety, maladaptive behaviors, and rigidity, compounding difficulties in daily functioning and social interaction (Passarini et al., 2025; Vargas et al., 2025). Gender dysphoria, or incongruence between assigned gender and experienced gender, is three times more likely to be diagnosed for adolescents with ASD than their neurotypical peers, and ASD youth who identify as transgender or gender diverse are also more likely to experience anxiety and depression in part because of additional difficulty in conforming to societal norms (Kahn et al., 2023). Gender-affirming care can help alleviate these common mood-related comorbidities and includes using the adolescent’s chosen name and pronouns and supporting their gender identity development to establish a safe treatment environment (Hadland et al., 2023). Regardless of specific co-occurring diagnoses, systemic support for ASD youth that recognizes their unique talents and dignity and worth as individuals helps to reduce social isolation and stigma and promotes well-being and success. Due to the contributing reasons discussed throughout, it is difficult for adolescents with autism to effectively communicate and read peer interactions. Creating a small group environment with trusted adults in a safe space for autistic adolescents can allow students to practice social skills in a controlled and more predictable environment. These small groups help adolescents to develop social skills that allow them to navigate social interactions more effectively as well as build communication skills and confidence (Rising Above ABA, 2024). The school nurse can play a vital role in these small groups by educating students with autism about the physical and emotional changes they may experience during puberty as well as understanding gender dysmorphia and how to address it. Providing pictures or videos for better understanding and communication is also important for this education.
Finally, medication management is another essential role of the school nurse when working with autistic adolescents who often require a regimen of medications to treat ADHD, anxiety, depression, OCD, etc. (Autism Speaks, 2025b). As the adolescent develops and grows, the school nurse should assess for signs that medications may need adjustment, as well as monitoring for side effects. Effective daily communication with staff who work closely with the student as well as the student and guardians/caregivers can help identify emerging needs and plan for personalized intervention. Table 1 provides a summary of interventions when working with students on the spectrum.
School Nurse Interventions for Students with Autism
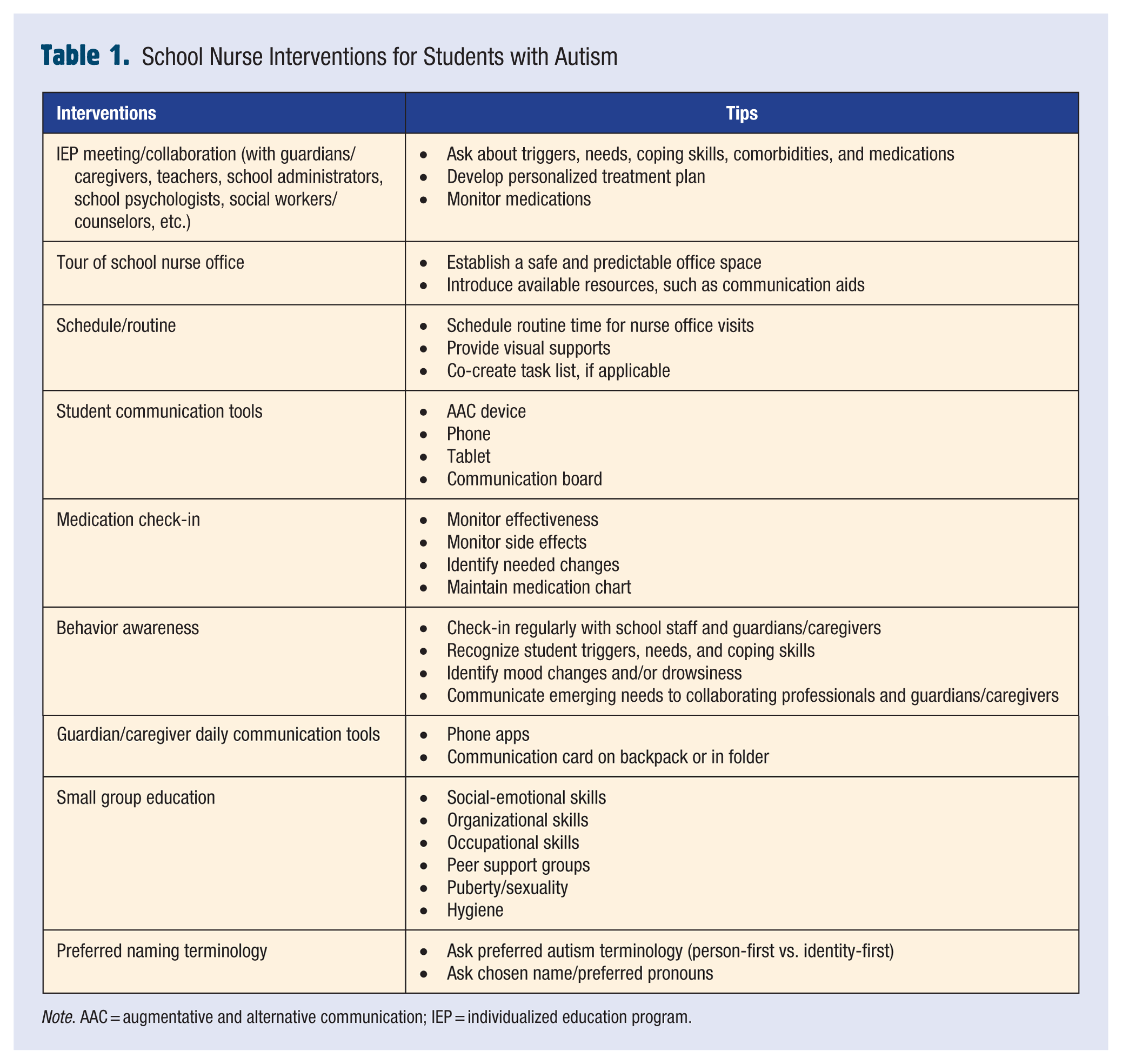
Note. AAC = augmentative and alternative communication; IEP = individualized education program.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval Statement
This article adheres to NASN’s established ethical standards. Ethical approval was not required as the work did not involve human participants, animal subjects, or sensitive data.
Dr. Jonel Thaller, PhD, MSW, CHW/CRS is an associate professor of Social Work in the College of Health
Dr. Constance McIntosh is a professor in the School of Nursing in the College of Health.
Mrs. Janelle Wendel, MSN, RN is an associate clinical lecturer in the School of Nursing in the College of Health.
Dr. Lindsey Ogle is an assistant professor of Special Education.