
Abstract
Colorectal cancer (CRC) incidence and death rates are increasing among people under age 50 in the United States. In addition to promoting on-time screening for average-risk adults starting at age 45, CRC signs and symptoms may need timely assessment by a health care provider to rule out other conditions and identify a diagnosis. The objective of this study was to examine primary care providers’ (PCPs’) awareness of CRC-related symptoms and their diagnostic approaches for patients under age 50 using the 2023 DocStyles panel survey. This survey included 1490 PCPs practicing in the United States. A descriptive analysis was conducted to examine symptom awareness and referral practices. Log binomial regression was used to examine predictors of greater symptom awareness. Symptom awareness of early-onset CRC was highest for changes in bowel habits (79%) and lowest for abdominal pain (43%). Fewer obstetricians/gynecologists and physician assistants were aware of CRC signs and symptoms. Most PCPs would complete a workup and assess patients for family history of cancer for patients presenting with rectal bleeding/bloody stools, iron deficiency anemia, or changes in bowel habits. Around 45% of PCPs would refer patients with rectal bleeding/bloody stools to diagnostic colonoscopy or offer a stool-based screening test. Some PCPs may benefit from additional training on signs and symptoms of early-onset CRC and evidence-based guidelines for symptom assessment. These findings indicate that many PCPs prefer to complete a medical workup and assess for family history of cancer as first steps, and most would not immediately refer patients to diagnostic colonoscopy.
Colorectal cancer (CRC) incidence and death rates are increasing among people under age 50.1,2 In the United States, from 2017 through 2021, the incidence of CRC for people under age 50 years was 8.8 cases per 100,000, with the corresponding death rate as 1.8 cases per 100,000 over the 2018–2022 time period.1,2 In most states, incidence rates are rising among people under the age of 50 years. 1 Patients under age 50 years are more likely to be diagnosed at a later stage of disease and have high-grade histology compared with patients aged 50 and older, and they often receive their diagnosis after having symptoms, rather than through routine screening.3–5 Studies have found that primary care visits for potential CRC symptoms are common among patients with early-onset CRC in the year prior to their diagnosis.6–8
In the United States in 2022, 66% of all early-onset CRC patients aged <45 were diagnosed as late-stage. 9 Although overall survival is comparable between early-onset and late-onset CRC patients, late and long-term effects of treatment can be particularly challenging for younger cancer survivors who may also be planning or raising families, managing the financial burden of cancer, and building careers.10–13 In 2021, these surveillance trends over the past decade prompted the United States Preventive Services Task Force (USPSTF) to lower the recommended screening initiation age to 45 years for people at an average risk for CRC. 14 Around 16% of early-onset CRC patients have a genetic variant that increases risk for cancer. 15
CRC can present with noticeable symptoms such as changes in bowel habits, symptoms related to anemia such as fatigue or shortness of breath during physical activity, unexplained weight loss, abdominal pain, or bloody stools.6,8,16 Although many of these symptoms may be attributed to other causes and are not specific to CRC, some are deemed “red flag” symptoms and may need timely diagnostic referral for colonoscopy.8,17 Additionally, having more than one red flag symptom increases the odds of a CRC diagnosis in people under age 50. 8 Although a number of studies have described CRC symptoms and identified treatment delays, there is still a recognized need for enhanced provider recognition of symptoms and clear follow-up and referral pathways, along with on-time screening of patients at average CRC risk starting at age 45 years.17–19 Since 2004, early-onset CRC deaths rates have continued to rise in the United States, and symptom recognition and timely diagnostic follow-up are important for average-risk patients under age 45 who do not meet the criteria for routine screening.17,19,20
To date, few studies are available on primary care providers’ (PCPs’) knowledge of CRC signs and symptoms in younger patients and their approaches to diagnostic workup and referral in the United States health care system. The objective of this study was to assess PCP knowledge of CRC signs and symptoms and their diagnostic practices, which may help inform future provider-related interventions by identifying areas to strengthen clinical support. This study builds on prior work on awareness of CRC red flag symptoms by providing a contemporary analysis following the release of the 2021 USPSTF screening recommendations that lowered the starting age for CRC screening for people at average risk for CRC and raised awareness of early-onset CRC.14,21
Methods
Study sample
The current study used Porter Novelli’s fall 2023 DocStyles panel cross-sectional survey for its sample. DocStyles was conducted via M3 Global Research, a marketing research company that recruits health care providers to complete their surveys (https://styles.porternovelli.com/docstyles/). The panel included United States PCPs who actively see patients; were employed in an individual, group, or hospital practice; and have been practicing for at least 3 years. The panel was capped at 1000 primary care physicians (family practice or internal medicine), although additional specialties and clinical roles were recruited (eg, obstetrician/gynecologists [OB/GYNs], nurse practitioners) and capped at 250 survey participants per specialty type or clinical role. For the 2023 fall DocStyles panel, additional specialties and clinical roles included OB/GYNs, pediatricians, nurse practitioners, and physician assistants. Participation rates ranged from 60% to 79% per specialty or clinical role, with an overall participation rate of 70%. Pediatricians were excluded from this series of survey questions, given the rarity of CRC in children and adolescents. Additional methodological details are available at https://styles.porternovelli.com/docstyles/. This study was conducted to be consistent with applicable federal law and Centers for Disease Control and Prevention policy and was not subject to institutional review board approval per 45 C.F.R. part 46.102[l][2], 21 C.F.R. part 56; 42 U.S.C. §241[d]; 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.
Survey questions
Knowledge of potential CRC signs and symptoms was assessed through a multiple response option checklist of red flag signs and symptoms (changes in bowel habits, bloody stools, unexplained weight loss, iron deficiency anemia, abdominal pain, and rectal bleeding; Supplementary Appendix S1). This study assessed typical referral or follow-up practices (eg, colonoscopy or gastroenterology [GI] specialist referral) for patients under age 50 with signs or symptoms that commonly occur before an early-onset CRC diagnosis. These symptoms included rectal bleeding or bloody stools, iron deficiency anemia, or changes in bowel habits. This study did not assess abdominal pain as a standalone symptom, despite its association with early-onset CRC, because of its association with many other health conditions. PCPs completing the survey could select multiple follow-up steps from the response items provided. Additional questions included if the practice had any patients aged 18–49 years in their practice or not, the age at which CRC average-risk patients are recommended for screening initiation, and demographic (eg, medical specialty) and medical practice characteristics (eg, practice setting).
Data management and analysis
All analyses were conducted using SAS v9.4 (SAS Corporation, Cary, NC), and figures were produced in Microsoft Excel. A descriptive analysis was conducted, examining demographic and medical practice characteristics of survey respondents, their knowledge of potential CRC signs and symptoms, their typical referral practices for patients under age 50 with potential CRC symptoms, and screening practices for patients at average risk for CRC. The analysis was restricted to PCPs who reported seeing patients under age 50 (n = 1490). The analysis on awareness of potential signs and symptoms of CRC was limited to PCPs who did not answer “don’t know” to this multiple response option question (n = 1468). For the series of questions on follow-up care for patients presenting with potential CRC symptoms, this study further analyzed co-occurring follow-up steps for PCPs who indicated they would complete a workup (labs and physical).
Statistical testing was performed using χ2 tests with a P-value <0.05 considered statistically significant to compare providers who identified 4 or more potential CRC signs and symptoms (ie, above the median value) to those who identified fewer than 4 symptoms on provider characteristics and screening practices.
Multivariable log binomial models were developed that examined predictors of knowledge of CRC symptoms by demographic and clinical practice characteristics of PCPs. Adjusted prevalence ratios (APRs) on awareness of 4 or more CRC signs and symptoms (at or above the median value) were calculated, comparing survey respondents on various demographic and clinical practice characteristics. A backward elimination modeling approach was used to remove nonsignificant variables (P > 0.10) that were not identified as confounders.
Results
Demographic characteristics of PCPs answering the module
A total of 529 (36%) PCPs were family practitioners, followed by internists (n = 463, 31%), OBGYNs (n = 252, 17%), physician assistants (n = 125, 8%), and nurse practitioners (n = 121, 8%). The majority of PCPs (n = 1001, 67%) worked in group practice settings (Table 1). A total of 525 (35%) PCPs were under age 40, 544 (37%) resided in the South, and 731 (49%) provided care to 100 or more patients per week. Over half of PCPs (n = 780, 52%) practiced in a suburban setting, and about 29% reported that, on average, their patient population had an income of <$50,000 per year (n = 425). Most PCPs initiated CRC screening for average-risk patients at age 45 (n = 1078, 75%).
Demographic Characteristics of Survey Respondents (n = 1490), Fall DocStyles 2023
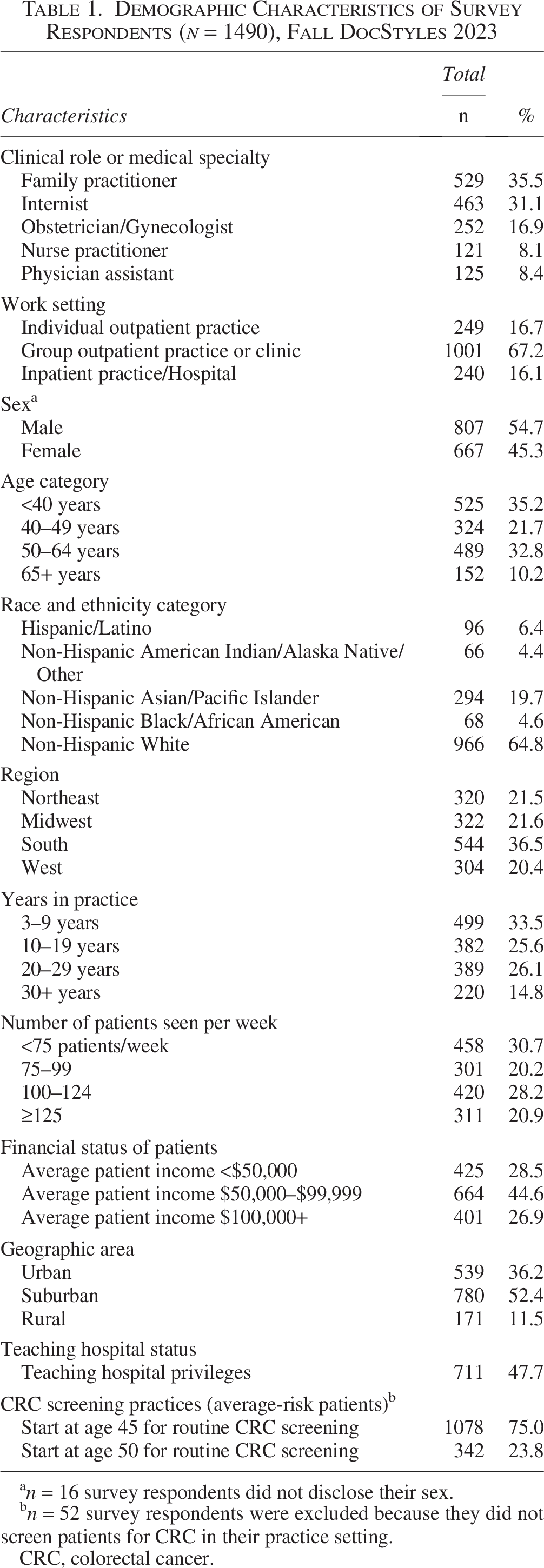
n = 16 survey respondents did not disclose their sex.
n = 52 survey respondents were excluded because they did not screen patients for CRC in their practice setting.
CRC, colorectal cancer.
Symptom awareness and typical follow-up care
Changes in bowel habits and bloody stools were the most frequently recognized CRC symptoms by PCPs (n = 1164, 79% and n = 1131, 77%, respectively; Figure 1). Only 632 PCPs (43%) recognized abdominal pain as a potential CRC symptom. For patients presenting with rectal bleeding or blood in the stool, PCPs indicated that their typical course of action would be to complete a workup (n = 1222, 82%) and assess for family history of cancer (n = 1131, 76%; Table 2). A total of 664 PCPs (45%) would refer patients to immediate diagnostic colonoscopy and 787 (53%) would offer a GI referral for further assessment. The typical follow-up for patients with iron deficiency anemia was completing a workup (n = 1380, 93%), followed by assessing for family history of CRC or related cancers (n = 974, 65%), and screening for CRC using a noninvasive stool test (eg, fecal immunochemical test [FIT]; n = 794, 53%). Only 362 PCPs (24%) would refer patients to an immediate diagnostic colonoscopy. For patients who report changes in bowel habits, 1240 PCPs (83%) would complete a workup as the next step, 923 (62%) would assess for a family history of CRC or related cancers, and 678 (46%) would refer patients to a gastroenterologist. Only 209 PCPs (14%) would refer patients to an immediate diagnostic colonoscopy, and 467 (31%) would advise patients to monitor their symptoms and return for a follow-up visit if they persist.
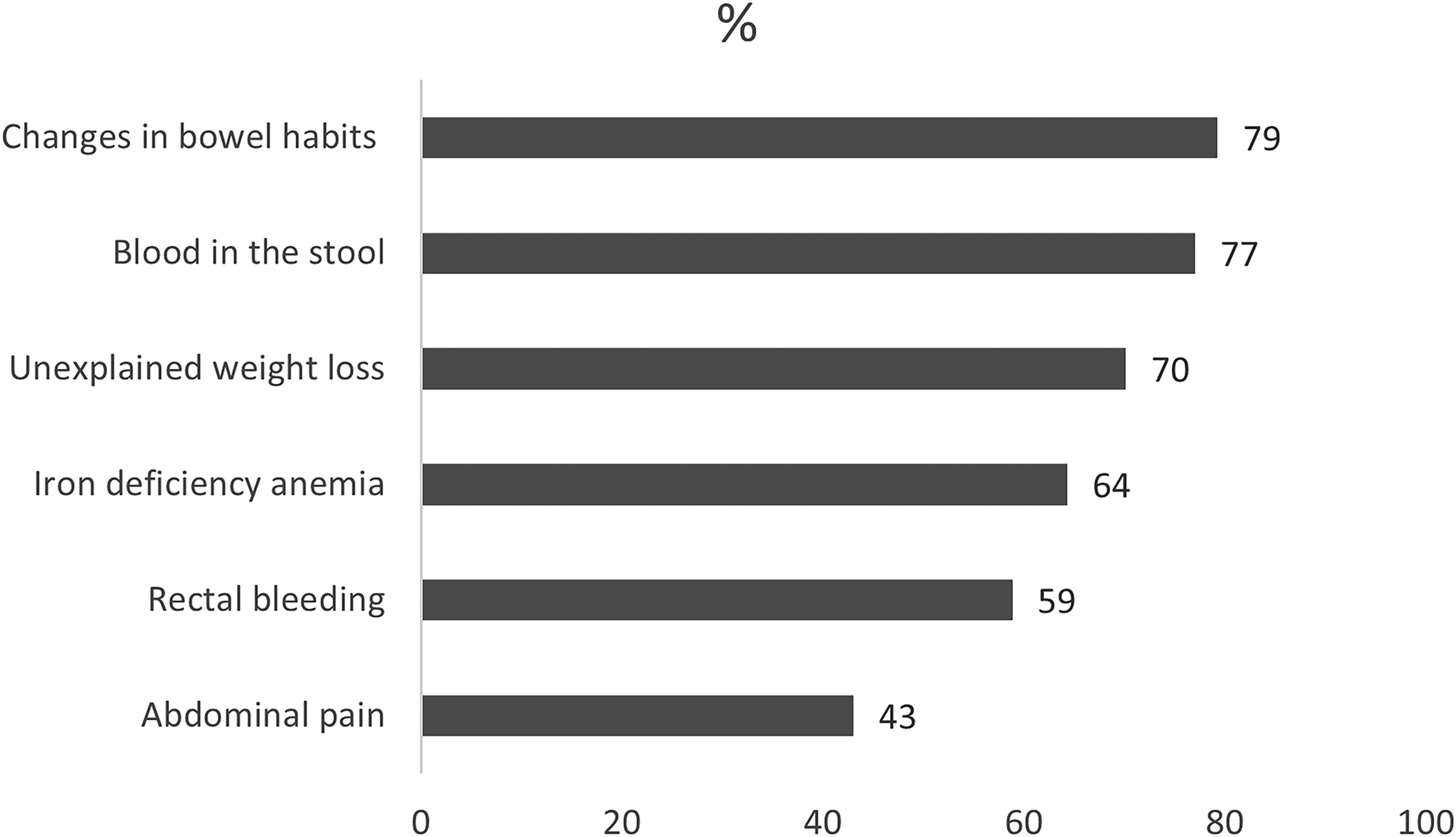
Recognition of potential colorectal cancer signs or symptoms in patients under age 50 years, DocStyles 2023 (n = 1468). Note: Survey respondents who answered “don’t know” were excluded from the analysis (n = 22).
Typical Follow-Up Care for Patients Under Age 50 Years with Potential Colorectal Cancer Signs or Symptoms (n = 1490), Fall DocStyles 2023
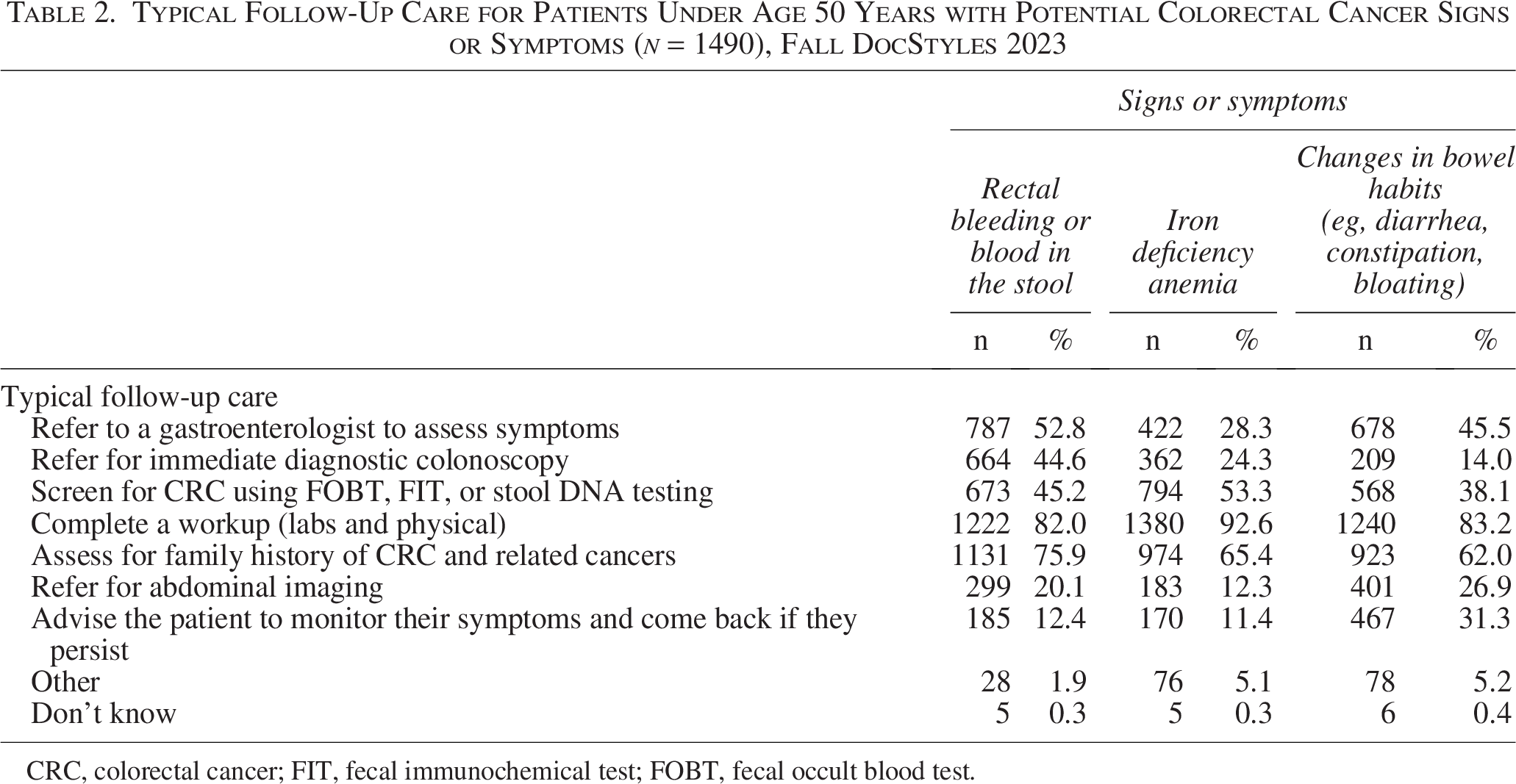
CRC, colorectal cancer; FIT, fecal immunochemical test; FOBT, fecal occult blood test.
Additional follow-up steps reported among PCPs completing a workup
The vast majority of PCPs who reported following up with a workup (labs and physical) also assessed for family history of CRC in all 3 sign/symptom-based scenarios, from 944 (68%) for iron deficiency anemia to 1025 (84%) for rectal bleeding/bloody stools (Figure 2). For symptoms such as bloody stools or changes in bowel habits, workups often included GI referral as well (n = 614, 50% and n = 523, 42%, respectively). However, among PCPs who would conduct a workup, use of stool-based tests was notable in all 3 sign/symptom-based scenarios, from a low of 519 (42%) among patients with changes in bowel habits to 756 (55%) when patients presented with iron deficiency anemia. Referral for diagnostic colonoscopy was only common for patients with rectal bleeding or bloody stools among PCPs who would complete a workup (n = 547, 45%).
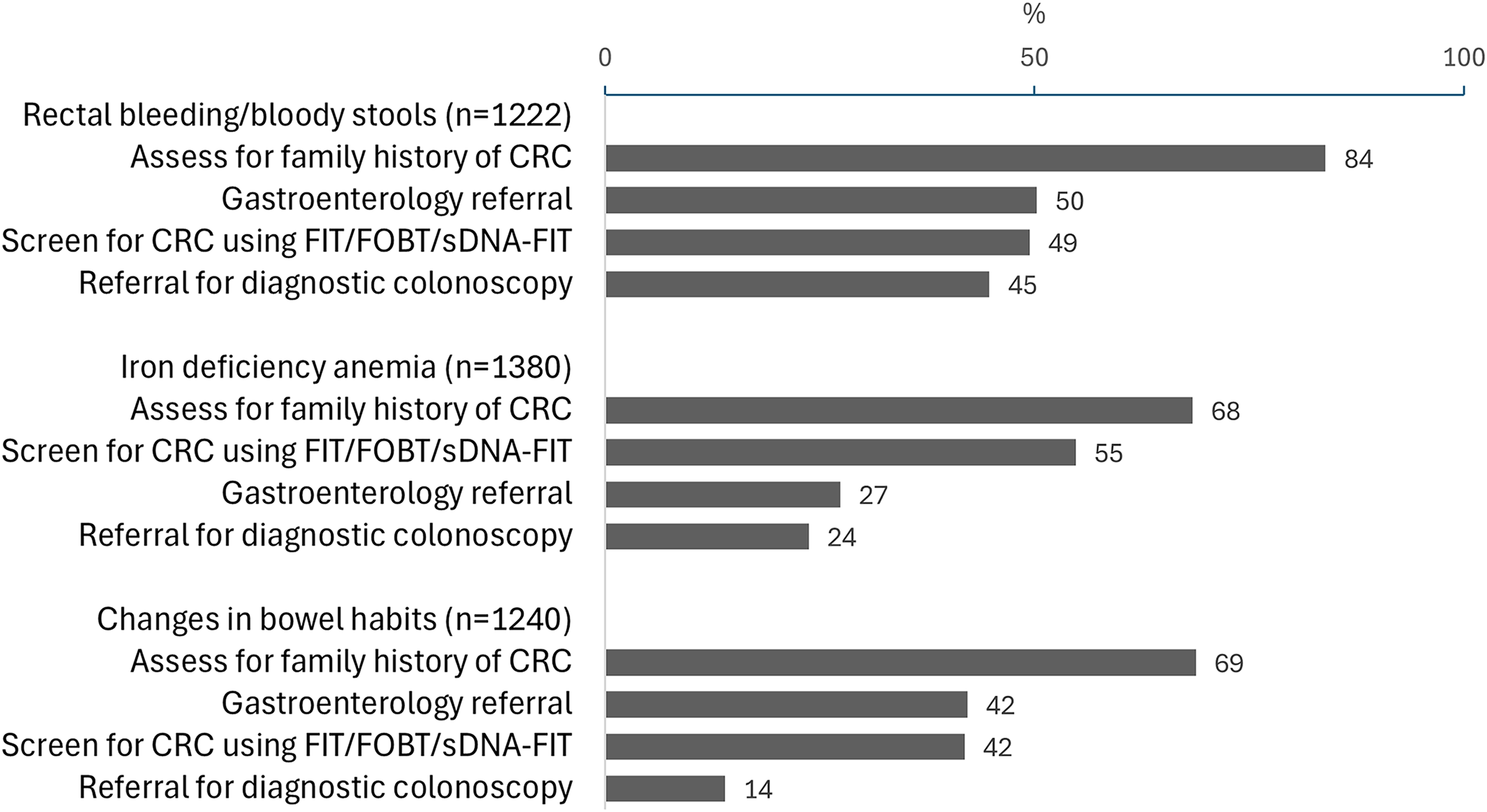
Percentage of PCPs completing a workup among patients aged <50 years with colorectal cancer-related signs or symptoms by their typical follow-up practices. FIT, fecal immunochemical test; FOBT, fecal occult blood test; PCP, primary care provider; sDNA–FIT, multitarget stool DNA testing.
Predictors of greater sign/symptom awareness by demographic and clinical practice characteristics
A total of 841 (57%) of PCPs identified at least 4 signs or symptoms of early-onset CRC. A lower percentage of OB/GYNs (n = 125, 50%) and physician assistants (n = 57, 48%) identified 4 or more potential CRC symptoms compared with other types of PCPs (Table 3). A higher percentage of PCPs aged 65 and older could identify at least 4 CRC symptoms (n = 100, 67%). PCPs who saw more than 125 patients a week also identified more CRC symptoms (n = 192, 62%). After adjusting for demographic and practice-based characteristics, identification of 4 or more CRC-related symptoms was significantly lower among physician assistants (APR = 0.80, 95% confidence interval [CI]: [0.65, 0.99]) and OB/GYNs (APR = 0.83, 95% CI: [0.72, 0.96]) than internists. PCPs aged 65 and older were significantly more likely (APR = 1.17, 95% CI: [1.02, 1.34]) to identify CRC signs/symptoms compared with PCPs aged 50–64 years. Identification of 4 or more CRC-related symptoms was significantly higher among PCPs seeing an average of 125 or more patients per week (APR = 1.17, 95% CI: [1.03, 1.33]) compared with PCPs seeing <75 patients per week.
Recognition of Greater Than the Median Number of Colorectal Cancer-Related Signs and Symptoms by Demographic and Clinical Characteristics, Fall DocStyles 2023 (n = 1468)
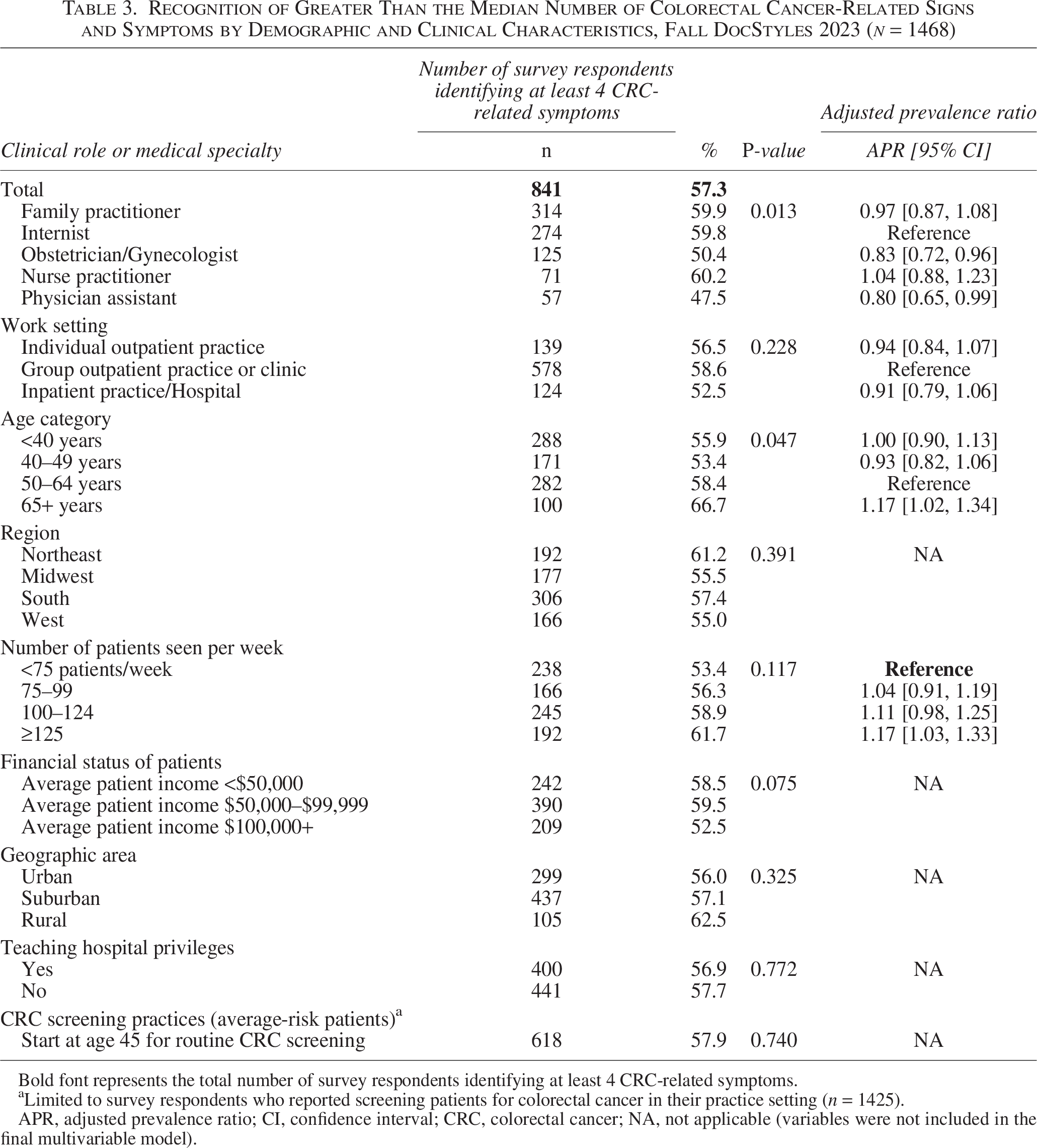
Bold font represents the total number of survey respondents identifying at least 4 CRC-related symptoms.
Limited to survey respondents who reported screening patients for colorectal cancer in their practice setting (n = 1425).
APR, adjusted prevalence ratio; CI, confidence interval; CRC, colorectal cancer; NA, not applicable (variables were not included in the final multivariable model).
Discussion
In this large, nationally representative panel of PCPs practicing in the United States, PCPs could identify a median of 4 signs/symptoms from a predefined list of 6 CRC-related signs/symptoms. Awareness was higher for more colon or rectal-specific symptoms, such as changes in bowel habits or blood in the stool, rather than symptoms reflective of many other conditions, such as abdominal pain. PCPs with more experience and patient load were more likely to recognize symptoms, along with those specializing in internal medicine or family medicine.
In this study, 45% of PCPs would refer patients to diagnostic colonoscopy to further assess rectal bleeding or bloody stools, but only 24% would refer patients presenting with iron deficiency anemia to diagnostic colonoscopy. These referral rates are lower compared with those found in a Colorado study reporting a majority of PCPs (72%) would refer patients to diagnostic colonoscopy for iron deficiency anemia, with slightly over half doing the same for hematochezia (ie, bright red blood in the stool). 21 In another study using clinical vignettes of patients with iron deficiency anemia, bidirectional endoscopy to identify intestinal bleeding was underused, and while 77% of survey respondents would follow up with endoscopy for a 35-year-old man, <20% would for a 35-year-old woman with iron deficiency anemia. 22 Patients experiencing changes in bowel habits (67% referral rate) or abdominal pain (61% referral rate) were less frequently referred to diagnostic colonoscopy compared with patients with unexplained weight loss (84% referral rate) in another study, although the vast majority of all patients received some type of CRC workup (77%). 23
For symptoms that often occur in CRC, PCPs in this study indicated they typically follow up with lab or physical examinations or assess for family history of CRC or related cancers, and less than half would do a GI referral in all scenarios. Referral practices also varied for the 3 signs/symptoms assessed. Nearly 30% of PCPs indicated they would advise patients experiencing changes in bowel habits to monitor their symptoms. For patients experiencing these symptoms, fewer PCPs (62%) reported they would assess patients for family history of cancer compared with patients experiencing other symptoms, although most would complete a physical workup. This may be a missed opportunity to identify patients at increased risk for CRC based on family history of cancer, because genetic variants that increase CRC risk are more common among people diagnosed with early-onset CRC compared with older patients, and having a family history of CRC is an important risk factor.24–26
Studies have found that nearly half of CRC patients initially present with blood in the stool or abdominal pain, and around 27% present with altered bowel habits. 16 Given that CRC patients aged <50 are more likely to present at a later stage at diagnosis, some major medical organizations recommend diagnostic colonoscopy for patients presenting with lower gastrointestinal tract bleeding or iron deficiency anemia.27,28 The current study’s findings suggest that PCPs may prefer to take a more measured approach when presented with patients with CRC red flag symptoms, such as conducting a workup and assessing family history of cancer before considering a diagnostic colonoscopy or GI referral based on a single sign or symptom. These findings align with a study that examined follow-up testing after the appearance of symptoms using claims data and found that other tests, such as fecal occult blood test (FOBT)/FIT or cross-sectional imaging, were often conducted first before diagnostic colonoscopy. 29 This approach may reflect a desire to rule out other conditions first before following up with GI or colonoscopy referral. However, we found that a minority of PCPs would follow up with a stool-based test. Given that we focused on patients under age 50, some PCPs may have a preference to offer a noninvasive test to unscreened patients aged 45 and older. Although this study did not assess colonoscopy availability, limited accessibility to colonoscopy may continue to exist in some rural geographic areas of the United States.30,31 Therefore, some PCPs may prefer to make colonoscopy referrals as a final step.
Understanding the circumstances that lead to the use of stool-based tests for triage or diagnostic purposes may inform future interventions on appropriate clinical follow-up for patients presenting with potential CRC-related symptoms. Currently, stool-based tests are recommended by the USPSTF and other major medical organizations only for screening of asymptomatic average-risk patients.5,14,32,33 In one study, 22% of patients receiving a multitarget stool DNA test were inappropriately tested because they had one or more contraindications for this test, including having a colonoscopy within the past 10 years, a significant family history of CRC, or potential CRC-related symptoms. 34
There is evidence that quantitative FIT calibrated to a lower detection threshold may help triage patients needing diagnostic colonoscopy by outperforming referrals based on symptom assessment alone. 35 The Association of Coloproctology of Great Britain and Ireland and the British Society of Gastroenterology have produced joint guidance on the management of patients with CRC symptoms by incorporating quantitative FIT results as a triage tool for urgent diagnostic colonoscopy.36,37 Another initiative is the use of timed diagnostic pathways (ie, Faster Diagnosis Standard) to ensure patients are not lost to follow-up and receive either a diagnosis or follow-up until resolution of symptoms. 38 This approach could be helpful in U.S. settings with fewer resources and isolated rural areas where accessing diagnostic colonoscopy may be more challenging, and adding additional strain on endoscopists may increase wait times for other patients needing immediate diagnostic colonoscopy. The current study’s findings may also be influenced by the increasing use of FIT over the past several years, rather than colonoscopy for routine screening and patient preferences for noninvasive stool tests.39–42 Additionally, trends in CRC screening prevalence show that recent increases in screening may have been driven by the use of sDNA/FIT, and although most PCPs and specialists still have a preference for colonoscopy, many recognize that stool-based tests are ideal for patients reluctant to undergo colonoscopy as a screening test.43,44
Clinical decision support and refined risk assessment tools may help clinicians decide on appropriate diagnostic colonoscopy referral or the most appropriate personalized CRC screening initiation age based on polygenic risk scores, personal risk factors, or biomarkers.45–47 The best approach to addressing early-onset CRC may be offering tailored screening to patients at increased risk based on family history of cancer and risk assessment algorithms, and ensuring that patients who do have symptoms are followed up with the appropriate diagnostic testing in a timely manner, while minimizing the number of patients lost to follow-up in the process. 17 Some researchers have proposed frameworks to address early-onset CRC through timely diagnosis by increasing awareness among young adults, proposing symptom triage and risk-adapted diagnostic pathways, increasing the collection of cancer family history, increasing health care provider awareness, and advancing EHR tools, machine learning algorithms, and artificial intelligence to support health care providers in evidence-based decision making.17,19
Some medical specialties, such as OB/GYNs, may benefit from educational outreach on early-onset CRC, given that many OB/GYNs function as PCPs to women of childbearing age. Partnering with medical organizations that represent these clinicians to deliver continuing medical education credits may help to raise awareness on appropriate evidence-based strategies to manage patients with potential symptoms of early-onset CRC.
The current study had several limitations. First, questions were included on a panel survey and not a population-based sample. The sample tended to be younger than practicing PCPs in the United States, but other demographic characteristics were similar. 48 Second, the self-reported responses could be influenced by social desirability bias. Third, there was limited survey space to ask in-depth questions using clinical vignettes that included a patient’s detailed history. With this information, it is possible that patients presenting with a constellation of symptoms or having a family history of cancer may warrant GI referral or diagnostic colonoscopy by PCPs. However, this study had a large sample of PCPs from across the United States, including those practicing in rural areas and in different types of practice settings. Although the current study’s questions were not cognitively tested, subject matter experts in survey design reviewed the questions during the survey development period.
In conclusion, this study found that awareness of most CRC-related signs and symptoms was fairly high among PCPs, but opportunities exist to increase sign and symptom awareness among OB/GYNs and physician assistants, and PCPs with less experience or patient load. Additionally, PCPs may benefit from additional training or implementation of clinical decision support tools to increase appropriate referral and follow-up when CRC-related symptoms occur. Assessing the current state of awareness for early-onset CRC and evidence-based practices around risk assessment and on-time screening may help to inform cancer control efforts.
Authors’ Contributions
J.S.T.: Conceptualization, data curation, formal analysis, writing—original draft, and writing—review and editing. M.C.P.: Conceptualization and writing—review and editing. S.M.C.K. and D.A.J.: Writing—review and editing.
Footnotes
Acknowledgments
The findings and conclusions in this research are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
The authors have no funding sources to report.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.