
Abstract
Prior work has shown that persons with disabilities have higher rates of poor cardiovascular outcomes than persons without disabilities. Little research has evaluated this relationship in persons with single and dual sensory loss. This study aimed to examine the association between single and dual sensory loss and cardiovascular disease (CVD). Data were obtained from 2021 Behavioral Risk Factor Surveillance System, a representative household survey of 234,394 noninstitutionalized civilian adults. The independent variable was sensory loss (neither, vision loss only, hearing loss only, both vision and hearing loss). The outcomes were self-reported angina/coronary heart disease, stroke, heart attack, and CVD (composite variable). Covariates were sex, age, race/ethnicity, education, employment, marital status, insurance, income, metropolitan status, body mass index, blood pressure, cholesterol, diabetes, depression, exercise, fruit and vegetable intake, smoking, and alcohol risk. Weighted multivariable logistic regression was used to evaluate the relationship between sensory loss and CVD, adjusting for covariates. In weighted and fully adjusted models, persons with vision loss only, hearing loss only, and dual sensory loss had increased odds of heart attack, stroke, angina/coronary heart disease, and CVD in comparison with persons without sensory loss. Additional research is needed to examine the underlying mechanisms influencing increased risk for CVD in persons with sensory loss. Initiatives are needed that aim to reduce the burden of CVD among persons with single and dual sensory loss.
The Centers for Disease Control and Prevention (CDC) reports that approximately 15.4% of persons had difficulty hearing and 18.8% had difficulty seeing between 2019 and 2023 in the United States. 1 Projections indicate that the proportion of persons with hearing or vision loss will increase exponentially in the United States by 2050.2,3 Cardiovascular disease (CVD) is the leading cause of morbidity and mortality in the United States, with its impact projected to increase over time. 4 CVD has well-documented prognostic implications for vision and hearing loss. Sensory loss is associated with a range of poor health behaviors and outcomes such as reduced engagement in health promoting behaviors, morbidity, and mortality.5,6 Conversely, compromised cardiovascular functioning often leads to inhibited sensorial functioning.7,8 Mechanisms through which sensory loss and CVD influence each other are complex and include reduced health-promoting behaviors, limited CVD knowledge, as well as systemic, biological, and physiological factors.5,6,9,10
Research has found that sensory loss is associated with an increased likelihood of having risk factors for CVD (eg, smoking status, physical inactivity, alcohol intake, obesity, depression, insufficient fruit and vegetable intake, hypertension, high cholesterol), CVD, cardiac events, and CVD-related mortality.11–13 One recent study found that persons with single or dual sensory loss were significantly more likely to develop CVD (24% increased risk for vision loss only, 20% for hearing loss only, and 35% for dual sensory loss). 13 Also, a 10-year study found that men with untreated hearing loss had higher rates of CVD, stroke, and CVD-related death compared with those without hearing loss. 14
Prior research on sensory loss and CVD has primarily focused on single sensory loss (hearing or vision loss separately) with little assessment of dual sensory loss (both hearing and vision) loss. Studies focused on the relationship between single sensory loss and CVD have often focused on middle-aged and older adults, a single cardiac outcome, were drawn from clinical or specialty settings, or were not conducted in the United States (eg,11–13). This study seeks to understand the influence of sensory loss on several CVD outcomes in a US adult sample, giving insights for the burden of this CVD among persons with sensory loss across the United States.
Dual sensory loss is common, and the proportion of persons with dual sensory loss is increasing in the United States, particularly among older adults. 15 Dual sensory loss is associated with worse physical and psychosocial well-being in comparison with a single sensory deficit. 16 Research indicates that the number of sensory impairments increases the likelihood of poor health outcomes in a graded fashion. 5 Persons with dual sensory loss are unable to engage in sensory substitution (in which one sensory system compensates for a deficit in the other) to support regular functioning. Most research on the health impact of dual sensory loss has focused on cognitive impairment or mortality.17,18 Research is needed to investigate the relationship between dual sensory loss and CVD.
This study assessed the relationship between single and dual sensory loss and CVD outcomes. We used data from the United States, the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative dataset of adults. We hypothesized that single and dual sensory loss would be associated with greater risk for coronary heart disease/angina, stroke, heart attack, and a composite measure of CVD. Findings from this study can inform policy, program, and intervention development and modification to improve CVD outcomes among persons with single and dual sensory loss.
Methods
Sample
This secondary cross-sectional study used data from the 2021 BRFSS. The BRFSS is administered yearly in English and Spanish by the CDC and state health agencies. In 2021, the overall response rate was 44.7%. Only 234,394 participants met study inclusion criteria by providing complete responses on sensory loss, cardiovascular outcomes, and select covariates.
Measures
Cardiovascular outcomes
CVD is defined as having one or more of the following cardiovascular outcomes: heart attack, stroke, or angina/coronary heart disease. 19 To measure this, respondents were asked to identify if they had ever been diagnosed with a heart attack, angina/coronary heart disease, or stroke. Responses to these questions were yes and no.
Sensory loss
Hearing loss was defined by the question, “Are you deaf or do you have serious difficulty hearing?” Vision loss was defined by the question, “Are you blind or do you have difficulty seeing?” Responses to both were yes and no. These questions were combined to create 4 mutually exclusive responses of neither, vision loss only, hearing loss only, and both.
Demographics
Race/ethnicity, sex, age, educational level, employment status, marital status, health insurance status, income level, and metropolitan status were included as demographics. Race/ethnicity was recoded into 5 groups: non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic other, and non-Hispanic multiracial. Sex was dichotomized as male and female. Age was categorized into 6 categories: 18–24, 25–34, 35–44, 45–54, 55–64, and 65 or older. Educational level was categorized into the following categories: did not graduate high school, graduated high school, attended college or technical school, and graduated college or technical school. Employment status was dichotomized as not employed and employed. Marital status was dichotomized as ever been married and never been married. Health insurance status was dichotomized as either having insurance or not having insurance. Income level was categorized into less than $15,000, $15,000–$24,999, $25,000–$34,999, $35,000–$44,999, $50,000–$99,999, $100,000–$199,999, and $200,000 or more. Metropolitan status was dichotomized as rural and urban.
Cardiovascular risk factors
Cardiovascular risk factors included in the present study include body mass index (BMI), high blood pressure, high cholesterol, diabetes, and depression. BMI was measured in kg/m2 and categorized as underweight (<1850), normal weight (1850–2499), overweight (2500–2999), and obese (3000 or more). Respondents were asked if they had ever been told they had high blood pressure, high cholesterol, diabetes, and depressive disorder. Responses were categorized as yes and no.
Health behaviors
Health behaviors included physical activity, smoking status, insufficient fruit intake, insufficient vegetable intake, and drinking status. Physical activity was assessed by asking if respondents had engaged in it in the past 30 days. Responses were yes and no. Smoking status was a provided calculated variable by BRFSS with responses recoded as never and ever smoker (everyday, someday, and former). Insufficient fruit and vegetable intake were dichotomized as 5 or more servings [sufficient] and 4 or fewer servings [insufficient]. The variables for alcohol risk status and heavy drinking status by sex were combined to form a 3-category variable indicating not a heavy drinking, male heavy drinking (14 or more drinks per week), and female heavy drinking (7 or more drinks per week).
Data analysis
Statistical analyses were completed in IBM® SPSS 26.0. Due to the complex design of the BRFSS datasets, the SPSS complex samples add-on module was employed with the appropriate design and survey weights. These survey weights adjust for unequal probability of selection, nonresponse bias, and post-stratification of the US adult population to produce representative estimates even when cell sizes are small. Due to skewed distributions across categories of sensory loss, particularly low prevalence of dual sensory loss, weighted multivariable logistic regression was employed for all analyses. Confidence intervals (CIs) were provided for all adjusted odds ratios (AORs) to allow readers to assess precision of estimates across subgroups. Design-adjusted chi-square (χ2) was used to compare study variables with sensory loss status. Multivariable logistic regression was used to determine the association between sensory loss and heart attack, stroke, angina/coronary heart disease, and CVD. The percentage of participants diagnosed with the specific cardiovascular outcome by sensory loss status was calculated.
Results
Bivariate analysis
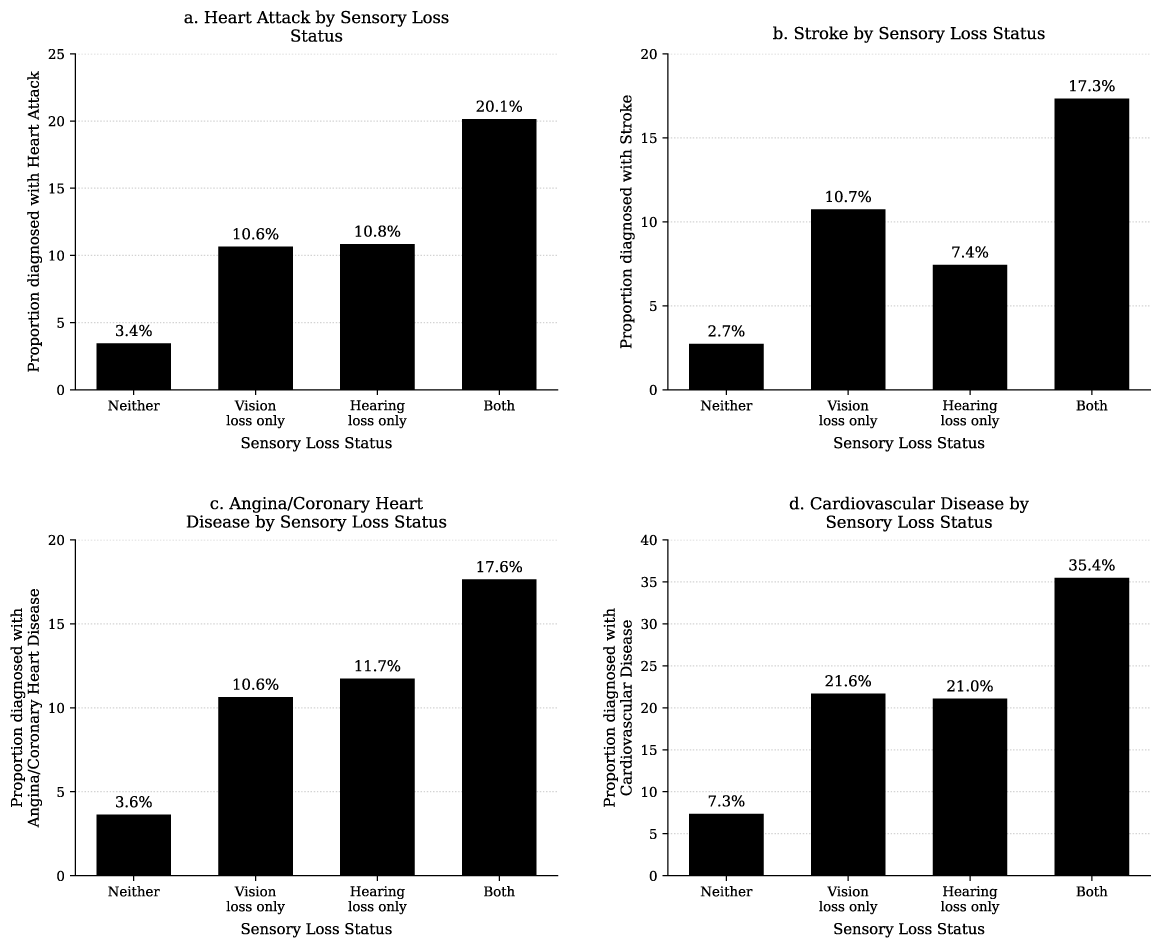
Table 1 shows demographic characteristics, health behaviors, and status by sensory loss status. In the weighted sample, 89.7% reported neither sensory loss, 3.4% reported vision loss only, 5.8% reported hearing loss only, and 1.0% reported both vision and hearing loss. The bivariate analysis showed that sensory loss status significantly differed by all cardiovascular outcomes (P < 0.001). People who experienced single or dual sensory loss had higher proportions of people with CVD in contrast to those with neither sensory loss. The percentages of heart attacks, stroke, and angina/coronary heart disease in individuals without sensory loss were 3.4%, 2.7%, and 3.6%, respectively, which were significantly lower compared with the 20.1%, 17.3%, and 17.6% among those with both hearing and vision loss. The prevalence of CVD ranged from 7.3% among persons with neither sensory loss to 35.4% among persons with both vision and hearing loss (Table 1; Fig. 1a–d).
Study Indicators for Participants by Sensory Loss Status, 2021 Behavioral Risk Factor Surveillance System Dataset (N = 234,394)
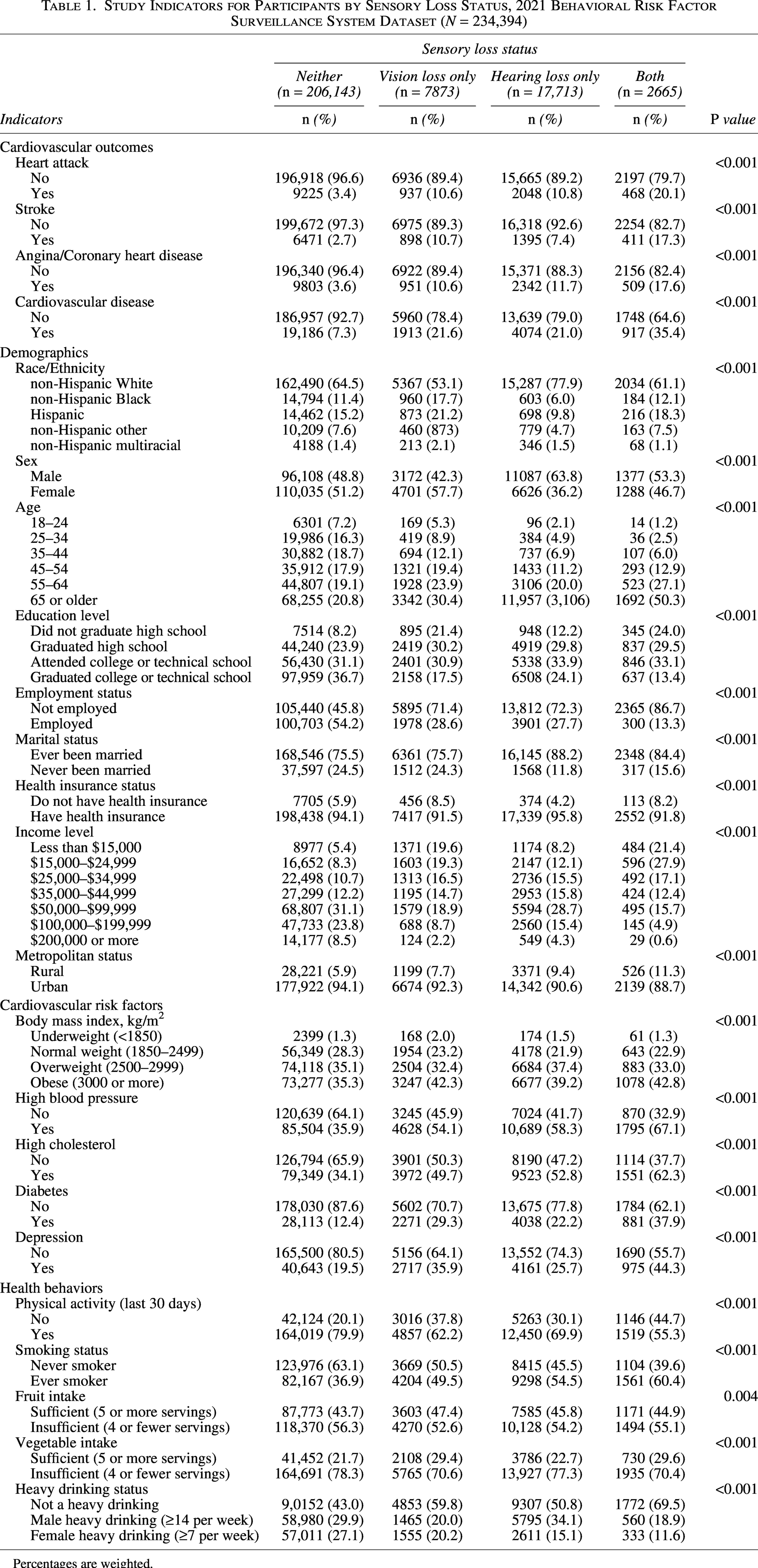
Percentages are weighted.
There were significant differences in all demographic variables by sensory loss status (all P < 0.001). Hispanic respondents made up a larger proportion of the vision loss only group (21.2%) and dual sensory loss group (18.3%) compared with their representation in the neither group (15.2%) or hearing loss only (9.8%). Gender patterns were also notable; the hearing loss group consisted mostly of men at 63.8%, but the vision loss group had more women at 59.0%. The dual sensory loss group included 50.3% of people aged 65 or older, while only 20.8% of people in the no-loss group reached that age. The highest percentage of individuals lacking a high school diploma (24.0%) and the lowest rate of college graduates (13.4%) were among those who experienced dual sensory loss. The unemployment rate among dual sensory loss respondents was 86.7%, whereas it stood at only 45.8% for respondents without any sensory loss. Income disparities were also evident. Of dual sensory loss individuals, 21.4% reported earnings under $15,000 annually, while 5.4% of those with neither disability earned less than $15,000, showing a clear income disparity compared with nondisabled individuals. Higher proportions of people with single or dual sensory loss had risk factors for CVD (obesity, high blood pressure, high cholesterol, diabetes, and depression) in comparison with those with neither disability. The highest percentages of risk factors occurred in the dual sensory loss group (42.8% obesity, 67.1% high blood pressure, 62.3% high cholesterol, 37.9% diabetes, and 44.3% depression). People with single and dual sensory loss were less likely to engage in physical activity and were more likely to smoke. Conversely, some health-promoting behaviors (not engaging in heavy drinking, eating fruits and vegetables) were more common among persons with single and/or dual sensory loss.
Weighted multivariable logistic regression: Sensory loss and cardiovascular outcomes
Table 2 presents the multivariable logistic regression analysis results of the association of sensory loss and CVD outcomes. There was a higher likelihood of a cardiovascular outcome (heart attack, stroke, angina/coronary heart disease, and CVD) reported among persons with single or dual sensory loss. Figure 1a–d shows the proportion of participants that were diagnosed with each cardiovascular outcome.
The Association of Sensory Loss Status and Cardiovascular Outcomes, 2021 Behavioral Risk Factor Surveillance System Dataset (N = 234,394)
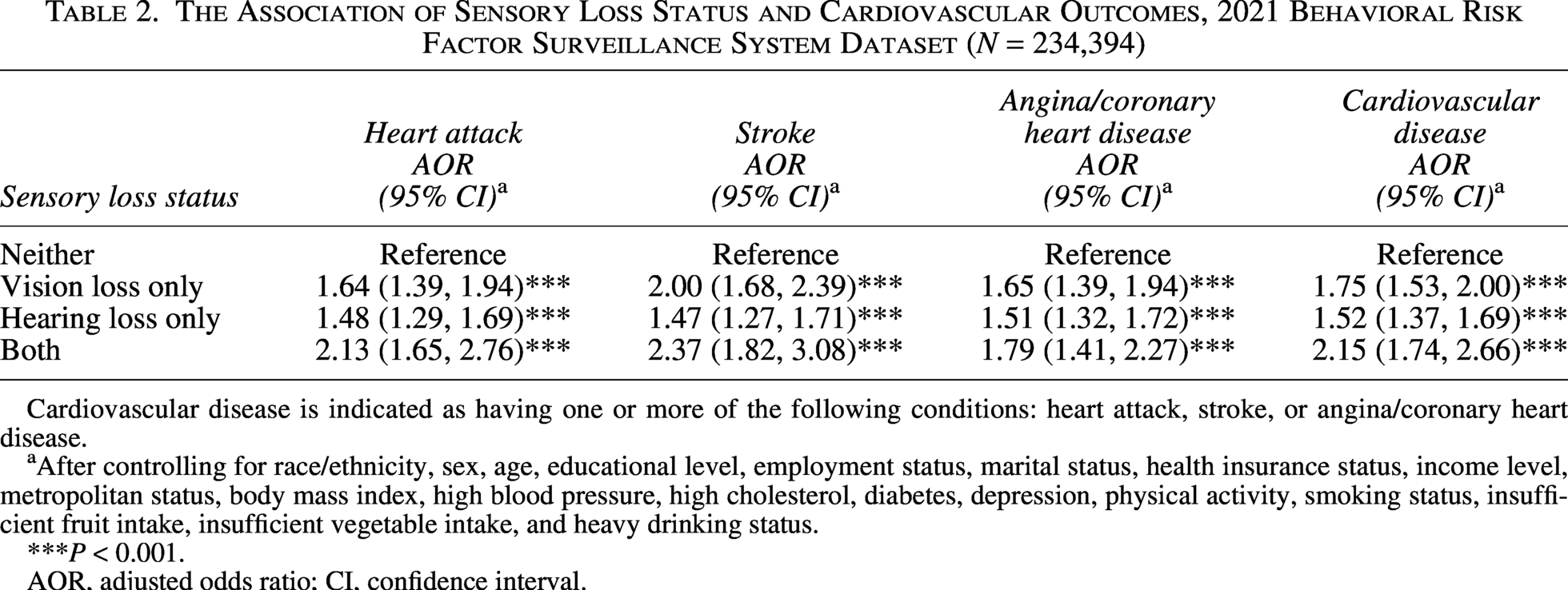
Cardiovascular disease is indicated as having one or more of the following conditions: heart attack, stroke, or angina/coronary heart disease.
After controlling for race/ethnicity, sex, age, educational level, employment status, marital status, health insurance status, income level, metropolitan status, body mass index, high blood pressure, high cholesterol, diabetes, depression, physical activity, smoking status, insufficient fruit intake, insufficient vegetable intake, and heavy drinking status.
***P < 0.001.
AOR, adjusted odds ratio; CI, confidence interval.
Heart attack
Individuals with vision loss showed a 64% higher risk for heart attacks compared with those without any sensory loss (AOR = 1.64; 95% CI: 1.39, 1.94). Compared with individuals without sensory loss, the likelihood of having experienced a heart attack increased by 48% among people with hearing loss only (AOR = 1.48; 95% CI: 1.29, 1.69). Individuals with dual sensory loss had over double the heart attack occurrence rate of those without sensory disabilities (AOR = 2.13; 95% CI: 1.65, 2.76).
Stroke
Compared with individuals without sensory disabilities, people with vision loss exhibited twice as much likelihood of experiencing a stroke (AOR = 2.00; 95% CI: 1.68, 2.39). Individuals experiencing hearing loss demonstrated a 47% increased risk of having a stroke when compared with those without sensory loss (AOR = 1.47; 95% CI: 1.27, 1.71). Individuals who experience both vision and hearing loss faced a 2.37-fold increased risk of stroke compared with people without sensory loss (AOR = 2.37; 95% CI: 1.82, 3.08).
Angina or coronary heart disease
Individuals with vision loss were subjected to a 65% greater likelihood of having angina or coronary heart disease when compared with individuals without sensory loss (AOR = 1.65; 95% CI: 1.39, 1.94). Compared with people without sensory loss, individuals with hearing loss had a 51% elevated risk (AOR = 1.51; 95% CI: 1.32, 1.72). Individuals who experience both dual sensory loss had nearly double the rate of reporting angina or coronary heart disease than those without sensory loss (AOR = 1.79; 95% CI: 1.41, 2.27).
Cardiovascular disease
The risk of reporting CVD among individuals with only vision loss was 75% higher than that of individuals without sensory loss (AOR = 1.75; 95% CI: 1.53, 2.00). The likelihood of reporting CVD is 52% higher in people with hearing loss than in individuals without sensory loss (AOR = 1.52; 95% CI: 1.37, 1.69). Compared with individuals without sensory loss, people who experienced dual sensory loss faced more than double the risk of reporting CVD (AOR = 2.15; 95% CI: 1.74, 2.66).
Discussion
In this study, a nationally representative sample of US adults was used to investigate the relationship between sensory loss and CVD. Persons with single or dual sensory loss were significantly more likely to have had a stroke, angina/coronary heart disease, or CVD than persons without vision or hearing loss. This indicates that single or dual sensory loss may increase the risk for poor cardiac outcomes. Initiatives are needed that aim to reduce the burden of CVD among persons with vision and/or hearing loss.
The burden of cardiovascular outcomes in this sample was notable among persons with sensory disabilities. Approximately 19% of persons with vision loss, 20% with hearing loss, and 35.2% of persons with dual sensory loss reported having CVD during their lifetime, in contrast to 6.5% of those without sensory loss reporting CVD. The same pattern was evident for specific CVD outcomes. The range is from the lowest burden among those with neither to the highest burden among those with dual sensory loss, as seen in Figure 1a–d. This finding is aligned with prior works indicating that the burden of CVD rates tends to be higher among persons with disabilities. 20 Hence, our findings add to a growing body of knowledge indicating that there may be a substantial burden of CVD among persons with vision and/or hearing loss in United States.
We also noted that the effect of sensory loss on cardiovascular outcomes was greatest among individuals with dual sensory loss. Prior work has shown that dual sensory impairment, in contrast to a single impairment, can substantially increase risk for poor health. Findings report that multiple sensory impairments increase the risk for some poor health outcomes in a graded fashion. 5 Other research indicates that single disabilities, in contrast to multiple disabilities, have been associated with better cardiovascular health. 21 A recent scoping review found that 91% of studies with comparison groups (n = 141) reported worse psychosocial, physical health, or participation outcomes in individuals with dual sensory impairment. 15 The current study is the first known to assess single and dual sensory loss in relation to specific and composite CVD outcomes in the United States. These findings underscore the urgent need for strategies to reduce CVD among those with single and dual sensory loss in the United States.
In addition, in this study, individuals with sensory loss had higher proportions of not graduating high school, not having employment, and having a lower income level when compared with those without a sensory disability. These results are mirrored by other evidence suggesting that individuals with disabilities experience lower SDOH. Literature indicates that the social determinants of health drive of health behaviors, which may indicate why individuals with sensory loss in this study were more likely to not participate in physical activity and higher rates of insufficient fruit and vegetable intake compared with individuals without sensory loss. Thus, addressing structural factors that influence the SDOH among individuals with sensory loss may improve health behaviors and CVD health outcomes.
Mechanisms through sensory loss may influence cardiovascular outcomes, which are behavioral, psychological, social, and biological in nature. Behaviorally, individuals with sensory loss may have lower engagement in health-promoting behaviors (eg, exercise) and higher engagement in health-risk behaviors (eg, smoking), increasing their risk for CVD.22,23 Psychological and social indicators of poor prognostic CVD outcomes such as depression and social isolation have been found to be more likely among persons with sensory impairments. 24 Biological factors such as inflammation and other physiological changes due to microvascular disease may influence this relationship.25,26 Individuals with dual sensory impairment, in contrast to those with a single sensory loss, may experience the greatest burden of CVD due to an inability to engage in sensory substitution (in which one hearing may compensate for vision loss or vice versa). Hence, mechanisms through which sensory loss may influence CVD may be amplified among persons with dual sensory loss, creating a cumulative effect on cardiovascular outcomes.
Strengths of this study are that we used a nationally representative sample of adults in the United States. Our sample included older adults, as in most prior work, and people aged 18 and older, providing broader inferences nationally. We assessed both single and dual sensory loss to provide insights for the increasing segment of persons with single and dual sensory loss in the United States. Furthermore, we assessed several specific cardiovascular outcomes (heart attack, stroke, angina/coronary heart disease) and a composite measure of CVD.
The limitations of this study are important to note. First, the cross-sectional study design inhibits making temporal inferences about cause and effect from these findings. Further longitudinal research is needed to assess temporality. Second, self-reports were used to obtain data on health status, which was subject to recall or prevarication biases. However, self-reported responses in BRFSS have been validated in prior research. 27 Lastly, there is the possibility of unmeasured or mis-specified (eg, self-efficacy, disability accommodations, racial/ethnic subgroups) confounders that may influence the association between sensory loss status and cardiovascular outcomes. These factors should be integrated into future research.
Findings from the current study have implications for health care provision, policy development, and additional research. Persons with sensory loss experience a disproportionate burden of CVD outcomes in the United States, particularly those with dual sensory loss. To mitigate the widespread impact of CVD on morbidity and mortality in the United States, targeted initiatives are needed to address the burden of cardiovascular outcomes among persons with hearing and/or vision loss. Existing programs, such as diabetes prevention programs, can be modified to address the needs of persons with sensory loss. A multilevel approach for interventions could address CVD morbidity, mortality, and CVD-related outcomes and improve the health outcomes among individuals with sensory loss as well as others. In clinical health care encounters, providers should be aware of the possibility of tailored support needs related to cardiovascular outcomes among persons with vision and/or hearing loss, or vice versa. Other multilevel interventions such as policy change/development could aim at addressing individual, social capital/cohesion, and environment to improve access and incorporating accommodations to improve SDOH and health behaviors. Incorporating a multilevel intervention approach could enhance the morbidity, mortality, and CVD outcomes among individuals with and without sensory loss.
Ethics/Consent
These data were deidentified and publicly available and were deemed exempt by the Arcadia University IRB. Informed consent was obtained from all individual participants included in the initial study. The authors affirm that human research participants provided informed consent for publication for these findings.
Data Availability
The datasets generated during and/or analyzed during the current study are available in the Behavioral Risk Factor Surveillance System repository, https://www.cdc.gov/brfss/annual_data/annual_2023.html.
Footnotes
Acknowledgments
All authors contributed to the study conception and design. Material preparation and analysis were performed by L.E. The first draft of the article was written by H.M., and all authors commented on previous versions of the article. All authors read and approved the final article.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors have no relevant financial or nonfinancial interests to disclose.