
Abstract
The United States continues to operate without coordination among the systems that ultimately determine health. Housing instability, untreated behavioral health conditions, food insecurity, and economic stress routinely determine whether patients can manage chronic illness or recover from acute events. Yet the systems responsible for these conditions operate independently of health care delivery. As a result, patients with the greatest needs are often required to navigate the most fragmented systems.
Recent policy efforts have begun to acknowledge this gap. Medicaid waivers, Medicare Advantage supplemental benefits, and federal demonstration programs have expanded support for addressing health-related social needs. The Centers for Medicare & Medicaid Services’ Accountable Health Communities model demonstrated that health systems can screen for social risks and connect patients with community resources at scale. 1 However, these approaches focus primarily on identifying needs and facilitating referrals.
The Central Challenge Is Not Identifying Social Needs—It Is Coordinating the Systems Responsible for Addressing Them
Health is not produced in the way medical treatments produce clinical effects. Rather, it emerges from stable housing, access to food, safety, sleep, and social support. Health systems can influence conditions impacting health only to the extent that they are aligned with the broader, interconnected systems in which patients live. Without that alignment, even well-designed interventions struggle to produce sustained improvements.
The organization of the U.S. health system reflects its historical development around acute and procedural care. Hospitals and specialty services dominate spending, and payment models reward clinical encounters rather than population outcomes. These structures have produced remarkable advances in treatment, but they are poorly suited to addressing conditions that originate outside the clinical setting.
Research consistently demonstrates that social and economic conditions account for a substantial share of health outcomes.2,3 Clinical care remains essential, but it represents only one component of a broader system influencing population health. 4 Despite this knowledge, the institutions shaping these conditions—housing, behavioral health, public health, and social services—operate through separate governance structures and financing streams.
Fragmentation Creates Structural Barriers
For individuals with complex needs, fragmentation creates compounding barriers. Patients experiencing housing instability and untreated behavioral health conditions frequently cycle through emergency departments, inpatient units, shelters, and correctional systems. 5 These patterns reflect not individual failure but system design. Earlier cross-system efforts demonstrate what coordination can achieve. The Jail In-Reach Project, which linked individuals with serious mental illness leaving jail to community-based health services, reduced rearrest rates by 62%. 6
Fragmentation Creates Economic Losses
Fragmentation is also an economic problem. Individuals experiencing housing instability and behavioral health conditions often generate high levels of utilization across multiple systems, including emergency departments, inpatient care, crisis services, shelters, and correctional systems. In fragmented systems, these costs accumulate without coordination, often exceeding tens of thousands of dollars annually per individual while producing poor outcomes and repeated crises. These expenditures reflect fragmented spending rather than coordinated investment.
Defragmentation: Potential Solutions Through Coordination, Homelessness
Complex problems require multisystem and complex solutions. Evidence from Housing First interventions illustrates both the consequences of fragmentation and the potential of coordinated approaches. National evaluations, including randomized controlled trials, have demonstrated reductions of approximately 24% in emergency department visits and hospitalizations among individuals experiencing chronic homelessness. 7
The implications at the system level are substantial. In Houston, where emergency department spending for chronically homeless populations has been estimated at approximately $100 million annually, even this conservative reduction would translate into roughly $24 million in avoidable emergency expenditures each year. 8 Yet emergency department spending represents only a fraction of the total cost burden. Individuals experiencing housing instability often generate substantial costs across inpatient care, crisis services, shelters, and correctional systems—costs that remain largely unmeasured and uncoordinated. Beyond these direct expenditures are broader societal costs, including disrupted education, reduced workforce participation, and lost productivity, which further compound the economic impact across communities. The observed reductions in emergency care are therefore likely only the visible portion of a much larger opportunity to realign spending across systems.
Houston’s experience further demonstrates that these gains are not achieved through isolated programs but through system alignment. Over the past decade, the city reduced homelessness by nearly two-thirds by coordinating public agencies, housing systems, and more than 100 nonprofit organizations into a unified, community-wide approach. 8
These patterns reflect not new spending but a reallocation of existing resources from fragmented crisis response toward coordinated, upstream investment. Fragmentation drives recurrent high-cost utilization, while coordinated investments in housing and supportive services can stabilize both outcomes and spending over time. Between programs for housing, homelessness, food insecurity and other social determinants, and the vast sums that could be saved in downstream health care spending, we do not need more funds, just better coordination and use of the combined totals.
Defragmentation: Potential Solution Through Policy and Governance
Accountable Communities for Health (ACH) provide a practical framework for addressing this fragmentation. ACH models bring together health care organizations, public health agencies, social service providers, and community stakeholders to align strategies and investments around shared population outcomes within defined geographic areas. 9 Rather than creating new programs, these models focus on governance—establishing structures that enable coordination across existing systems.
Shared data systems are central to this approach. Measurement and feedback loops allow communities to identify gaps, allocate resources more effectively, and adapt strategies over time. This creates a dynamic system in which policy, financing, and service delivery evolve in response to real-world outcomes.
Figure 1 illustrates how cross-sector governance structures can reallocate spending over time from fragmented crisis care toward coordinated investment in housing, health, and social services, supported by shared data systems that enable continuous reiterated learning.
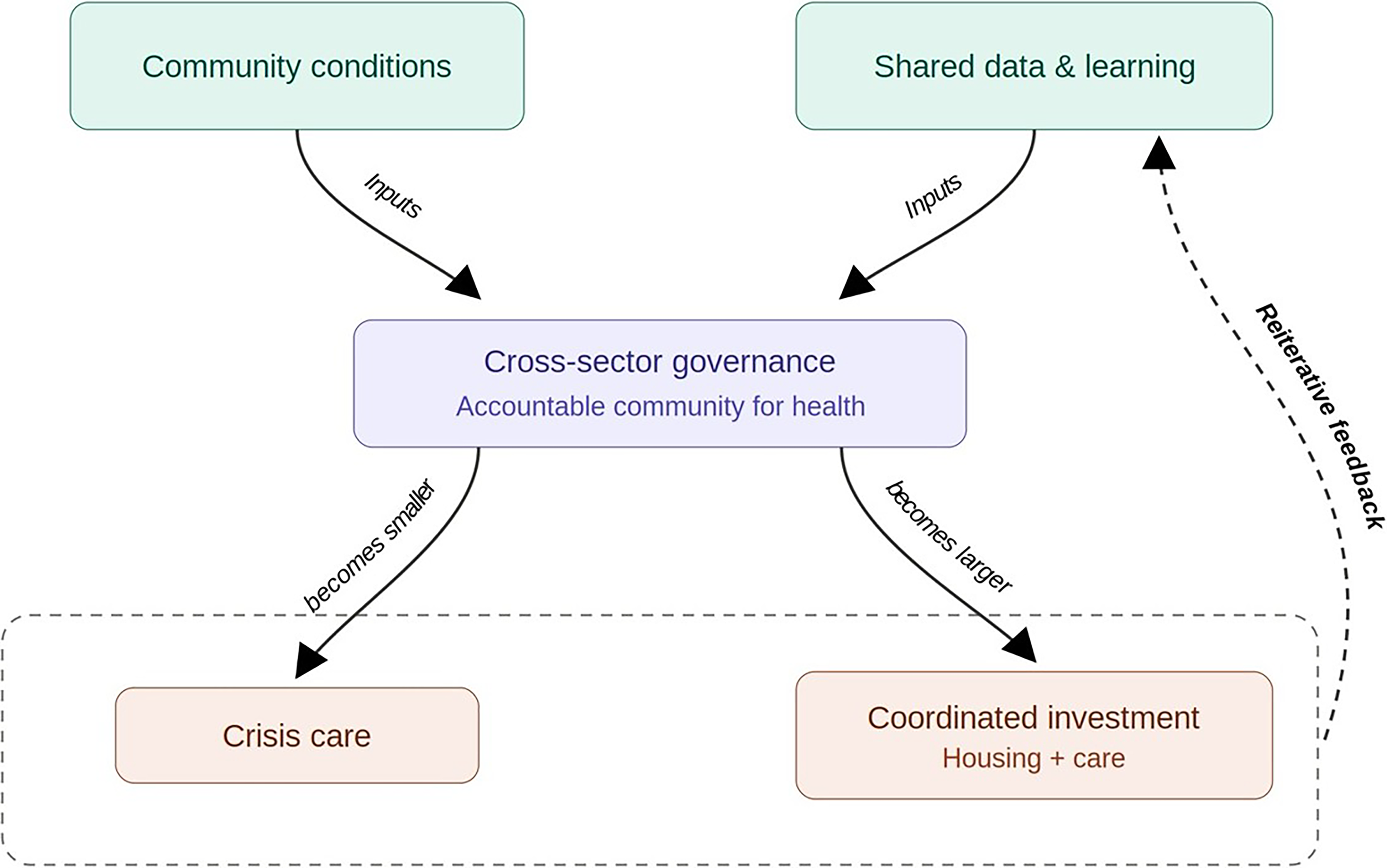
Building coordinated systems for population health: Cross-sector governance structures such as Accountable Communities for Health reallocate spending from fragmented crisis care toward coordinated investment in housing, health, and social services. Shared data and learning systems create feedback loops that allow policy and investments to evolve over time, strengthening the infrastructure that makes health possible.
Significant pilot programs in California (e.g., California Accountable Communities for Health Initiative, CACHI.org) and Texas (e.g., Texas Accountable Communities for Health Initiative, TACHI.org) have demonstrated the potential of ACH, but consistent governance structures and sustainable financing models remain underdeveloped. Building this infrastructure requires policy support across three domains.
First, governance
Policymakers can support community-level structures that align health systems, public health agencies, and social service organizations around shared population outcomes.
Second, financing
Medicaid Section 1115 waivers and related innovation models provide mechanisms to fund services addressing housing, nutrition, and other health-related social needs. 10 However, these efforts often remain fragmented. The next phase of waiver design should explicitly support cross-sector coordination by funding backbone functions—shared governance, data infrastructure, and joint decision-making capacity. Recent waivers in states such as California and North Carolina have begun to include these elements, recognizing that coordination itself requires dedicated investment. Although some waivers have recently been paused or modified at the federal level, emerging evidence suggests that multi-sector waiver models can improve efficiency by enabling more strategic allocation of resources across systems.
Third, workforce
Investments should expand roles such as community health workers and care navigators who can operate across institutional boundaries and support coordination for populations with complex needs. Without dedicated financing for coordination, investments in services will continue to operate in parallel rather than as a system.
Call to Action
It is time to build the infrastructure that makes health possible. Health systems do not produce health. They can build the infrastructure that makes health possible. The next phase of reform should focus on developing community-level accountability structures capable of aligning the systems that shape health. Over time, these efforts can create a coordinated infrastructure that improves outcomes while stabilizing costs. The question is no longer whether social conditions shape health, but whether we will build the systems required to act on that knowledge.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.