
Abstract
Children with special health care needs (SHCN) face poorer access to and quality of health care than children without SHCN, leading to greater unmet health care needs. Chronic pain, a common comorbidity of chronic conditions, is associated with greater risk for poor physical and psychological functioning and increased health care utilization. However, little is known about chronic pain in children with SHCN and unmet health care needs in this population. Secondary analysis of the 2022 National Survey of Children’s Health (NSCH), a nationally representative survey of youth aged 0–17, was conducted. SHCN status, chronic pain presence, and the presence of and reasons for unmet health care needs were assessed. Models were adjusted for demographic and socioeconomic factors. Among all 52,713 participants, 12,762 (21%) had SHCN, and 2806 (5.5%) reported chronic pain. Children with SHCN experienced a higher prevalence of chronic pain (14.0%) than those without SHCN (3.2%). Greater odds of unmet health care needs were associated with chronic pain; odds further increased among children with both SHCN and chronic pain. Commonly reported barriers to health care included problems getting an appointment, services not available in the area, and the office not being open when the child needed care. Children with SHCN are disproportionately affected by chronic pain, which is strongly associated with increased unmet health care needs. Reported barriers primarily reflected issues with access to and availability of services. Enhancing access to pediatric pain management services may help reduce these disparities and improve health outcomes in this population.
Children with special health care needs (SHCN) are defined by the U.S. Maternal and Child Health Bureau (MCHB) as those who have a chronic physical, developmental, behavioral, or emotional condition and who require greater health and related services than generally required by children.1,2 This population represents a diverse group of individuals with a variety of conditions (i.e., intellectual and developmental disabilities, mental health conditions such as depression and anxiety, and chronic illnesses like asthma), with the majority experiencing functional limitations. 1 According to data from the National Survey of Children’s Health (NSCH), approximately one in five children in the U.S. have a special health care need. 3 Compared with their peers, children with SHCN often face greater barriers to accessing health care and receive poorer quality health care services, contributing to higher rates of unmet health care needs in this population.3–5 These unmet health care needs during childhood can lead to exacerbated medical issues, decreased functional level, increased family financial and emotional burden, and poorer health outcomes in adulthood.6,7
Chronic pain, defined as pain persisting or recurring for at least 3 months, is an emerging public health concern among pediatric populations. An epidemiological systematic review of pediatric chronic pain estimated prevalence to be between 11% and 38%, depending on pain type and population characteristics. 8 Chronic pain is a common comorbidity of chronic conditions and is often associated with poorer physical and psychological functioning and reduced quality of life.9–11 While prior research has examined chronic pain prevalence among children with specific conditions such as cerebral palsy or autism, little is known about the prevalence of chronic pain among the broad population of children with SHCN.12,13 Children with SHCN represent a federally recognized population priority group given their heightened need for health care services and system-level attention. 14 Therefore, understanding chronic pain in this population is crucial for informing targeted system-level policies and interventions.
Like children with SHCN, children with chronic pain have higher rates of health care utilization and may similarly face increased risks of unmet health care needs. 15 Yet, unmet health care needs in children with SHCN with chronic pain remain understudied. Given that both chronic pain and unmet health care needs are associated with worse health outcomes, identifying disparities in care for this group is critical. Thus, nationally representative data are needed to characterize the prevalence of chronic pain among children with SHCN and to examine the extent and reasons for unmet health care needs for children with SHCN with chronic pain. Such insights could inform efforts to improve pediatric pain assessment and management, enhance access to care—including specialty pain services—and ultimately support better health outcomes in this population.
This study has two primary aims. First, to assess whether the prevalence of chronic pain differs between children with and without SHCN. Second, to examine whether children with SHCN with chronic pain have increased odds of reporting unmet health care needs, as well as to identify the types and reasons for these unmet health care needs. A secondary aim is to explore differences in other types of health care utilization—such as use of specialty and alternative health care services—between these groups.
Methods
Study design and population
This study analyzed data from the 2022 NSCH. The NSCH is a nationally representative population-based household survey of non-institutionalized youth aged 0–17 years conducted annually by the Health Resources and Services Administration’s MCHB. In 2016, the NSCH started integrating the previous NSCH survey and the National Survey of Children with Special Health Care Needs (NS-CSHCN). All measures in the NSCH are self-administered as a paper mail or web-based survey that is completed by the parent or guardian of the randomly selected child from that sampled household. When appropriate, the NCSH oversamples both children with SHCN and children aged 0–5 years. Sampling weights are provided to ensure estimates are representative and generalizable to non-institutionalized U.S. children. This 2022 NSCH dataset included data from 54,103 children and had a weighted overall response rate of 39.1%. 16 The 2022 NSCH dataset was selected for this analysis, as it is the last survey year in which the Use of Alternative Health Care variable was collected. 17 Participants were included in the analysis if they completed the SHCN screener, chronic pain question, unmet medical needs questions, and had data for all covariates available. This study was deemed exempt from requiring approval by the University of Minnesota institutional review board due to all data being deidentified and publicly available.
Data collection/variables
SHCN, chronic pain, and unmet health care needs
Classification of being a child with SHCN was identified by the SHCN screener. The screener is a five-item tool that was designed to reflect the federal MCHB’s consequence-based definition of children with SHCN. 18 The purpose of this designation is to identify children with a range of diversity of chronic conditions and special needs, which is more comprehensive than focusing on a single diagnosis or type of special need. To meet special health care need status, the child must have met the following criteria: currently experiences at least one of the five different health consequences (1) use or need of prescription medication, (2) above-average use or need of medical, mental health, or educational services, (3) functional limitations compared with others of same age, (4) use or need of specialized therapies, and (5) treatment or counseling for emotional or developmental problems; the consequence is due to a medical and health condition; and the duration or expected duration of the condition is 12 months or longer.
Chronic pain status was assessed with the question, “During the past 12 months, has the child had frequent or chronic difficulty with the following? Repeated or chronic physical pain, including headaches or other back or body pain,” with dichotomous response options of “Yes” or “No.”
Classification of unmet health care needs was also dichotomous and assessed with the question, “During the past 12 months, was there any time when this child needed health care, but it was not received? By health care, we mean medical care as well as other kinds of care like dental care, vision care, and mental health services.” For parents who responded Yes to this question, they were also asked the question, “Which types of care were not received?”, with the options of hearing care, medical care, dental care, vision care, mental health services, or other. Parents who answered Yes to having unmet health care needs were also asked the question, “Did any of the following reasons contribute to this child not receiving needed health services?”. There were six reasons with each having a response option of “Yes” or “No”: (1) there were problems getting an appointment when this child needed one, (2) the services this child needed were not available in your area, (3) there were issues related to cost, (4) this child was not eligible for the services, (5) the clinic or doctor’s office wasn’t open when this child needed care, and (6) there were problems with getting transportation or child care.
Other health services utilization
Variables measuring utilization of other services such as seeing a specialist, using alternative health care, and requiring a referral to receive services were included in the analysis. Information regarding the use of a specialist visit was assessed with the question, “During the past 12 months, did this child see a specialist other than a mental health professional? Specialists are doctors like surgeons, heart doctors, allergy doctors, skin doctors, and others who specialize in one area of health care.”, with the response options of “Yes,” “No, but this child needed to see a specialist,” and “No, this child did not need to see a specialist,” which were dichotomized into Yes and No for analysis purposes. Parents were also asked the questions of “During the past 12 months, did this child need a referral to see any doctors or receive any services” and “During the past 12 months, did this child use any type of alternative health care or treatment? Alternative health care can include acupuncture, chiropractic care, relaxation therapies, herbal supplements, and others. Some therapies involve seeing a health care provider, while others can be done on your own.”, which both had response options of “Yes” or “No.”
Covariates
Covariates included sex, age, race, insurance type, family income, and U.S. geographical region. Age was categorized into three developmentally relevant groups: 0–5 years, 6–11 years, and 12–17 years. Race was dichotomous and included the categories of White and Black or other races.
Insurance type included the categories of public only (government assistance), private only (privately purchased, including through the ACA marketplace, through an employer, or TRICARE), private and public, and not insured. Family income was measured using the imputed family poverty ratio variable and was categorized as ≥400%, 200–399%, 100–199%, and <100% of the federal poverty level (FPL). U.S. geographical regions were categorized utilizing the state of residence of the respondent and were grouped according to the U.S. census regions of Northeast, Midwest, South, and West.
Variable selection
Outcome and factor selection for this secondary data analysis were guided by Andersen’s behavioral model of health service use (1968). 19 This model proposes that health care access and utilization are influenced by three primary components of individual and system-level factors: predisposing factors, enabling factors, and need factors. Predisposing factors include demographic characteristics such as age and sex; enabling factors include resource-related characteristics such as income and insurance status; and need factors include health-related characteristics such as medical complexity and symptom burden. In this analysis, unmet health care needs and other health care utilization variables (e.g., use of alternative health care) were evaluated as outcomes related to health care access and utilization. Predisposing factors included sex, age, and race; enabling factors included insurance type, family income, and U.S. geographical region; and need factors included SHCN and chronic pain status. These components guided covariate selection and development of multivariable models. Need-related factors, including SHCN and chronic pain status, were of primary interest given their potential combined influence on health care access and unmet health care needs.
Statistical analyses
Descriptive statistics of the sample by SHCN-status were conducted using both unweighted and weighted counts and weighted proportions for categorical variables. Two logistic regression models were used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for prevalence of chronic pain based on SHCN-status. These included both an unadjusted model of SHCN-status and chronic pain prevalence and an adjusted multivariable model with the covariates of sex, age, race, insurance type, family income, and U.S. geographical region. A multivariable logistic regression model was used to examine the relationship between SHCN and chronic pain status on odds of reporting unmet health care needs while adjusting for the covariates of sex, age, race, insurance type, family income, and U.S. geographical region. Adjusted predicted probabilities and risk differences were estimated from survey-weighted logistic regression models using average marginal effects. Descriptive statistics utilizing weighted survey estimates were calculated for reasons and types of unmet health care needs and use of other health care services. Chi-square tests were used to assess differences in reasons for unmet health care needs as well as differences in other health service utilization measures by SHCN and chronic pain status. For all analyses, the significance threshold was defined as a two-sided P value <0.05. Analysis was conducted using SAS Studio version 9.04.01, release 3.81 (Enterprise Edition), and included adjustments for survey weights.
Results
Study population
Among participants eligible for inclusion in the analysis (n = 52,713; weighted sample size = 70,919,602; mean age 8.8 years, 51% male, 70% white), 21% met SHCN criteria (unweighted sample size = 12,762, weighted sample size = 14,899,392). Children with SHCN were generally older than children without SHCN and slightly more likely to have public-only and combination (private and public) insurance types, be male, and have lower family income, see Table 1. The prevalence of chronic pain in the sample was 5.5% (unweighted sample size = 2,806, weighted sample size = 3,889,907). Unmet health care needs were reported for 3.2% of the sample (unweighted sample size = 1,812, weighted sample size = 2,298,090).
Demographics and Characteristics of Analysis Sample among Children with SHCN and Children without SHCN (N = 52,713)
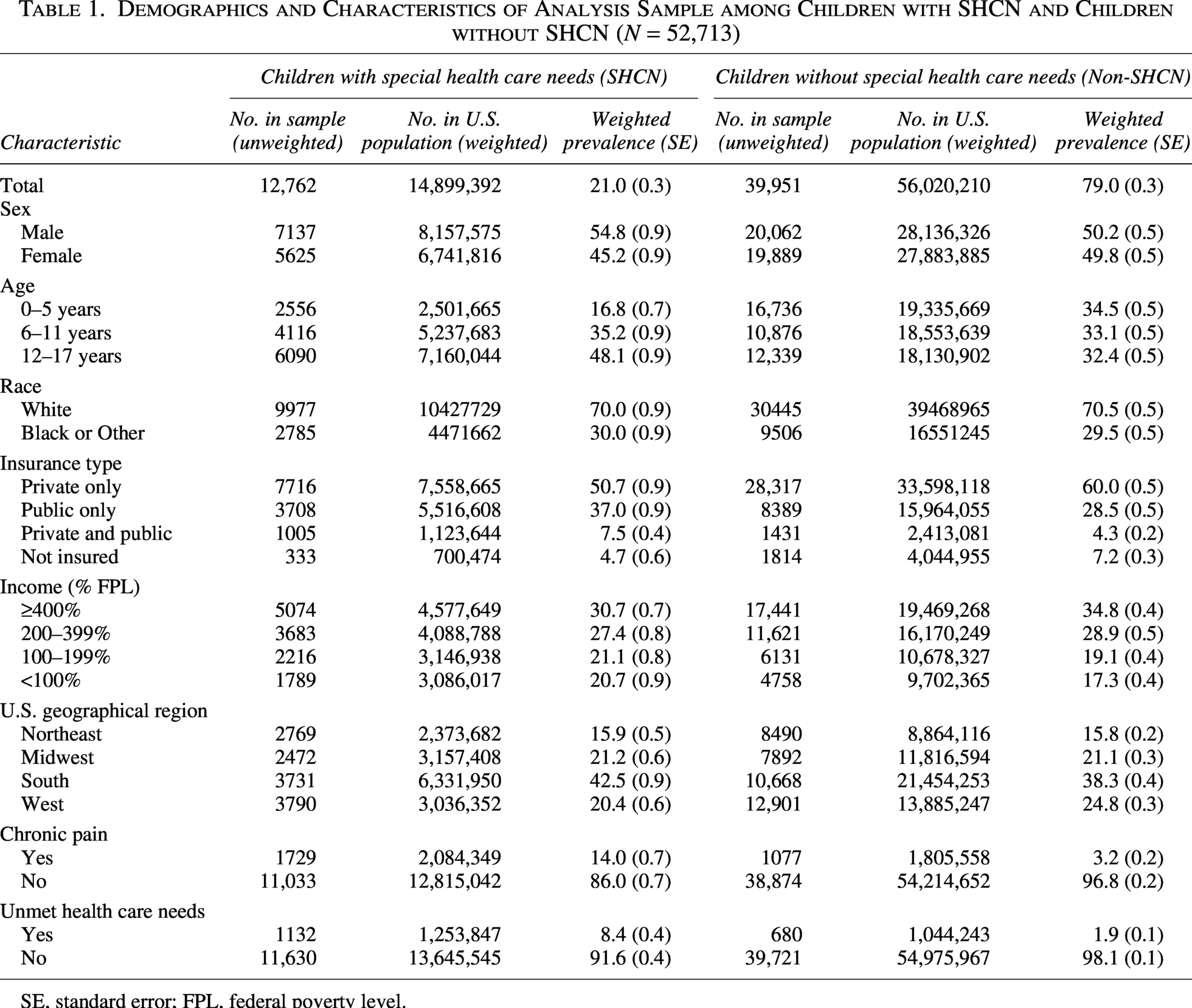
SE, standard error; FPL, federal poverty level.
SHCN and chronic pain
Chronic pain prevalence was 14.0% for children with SHCN compared with 3.2% for children without SHCN. The unadjusted model results showed that children with SHCN had 4.9 times the odds of having chronic pain compared with children without SHCN (P < 0.001). Children with SHCN had 3.9 times the odds of having chronic pain compared with children without SHCN, after adjustment for covariates (P < 0.001). The adjusted predicted probability of chronic pain was 10.8 percentage points higher among children with SHCN compared with children without SHCN. Significant covariates in the adjusted model were sex, age, insurance type, income, and U.S. geographical region. Odds of chronic pain were higher for females (P < 0.001), those aged 6–11 years and 12–17 years compared with those aged 0–5 years (both P < 0.001), those with public only and combination (private and public) insurance types compared with those with private insurance (both P < 0.01), those with income less than 400% of the FPL (all P < 0.01), and the West compared with the Northeast region (P = 0.021) (Table 2).
Unadjusted and Adjusted Logistic Regression Model Results for Chronic Pain by SHCN Status
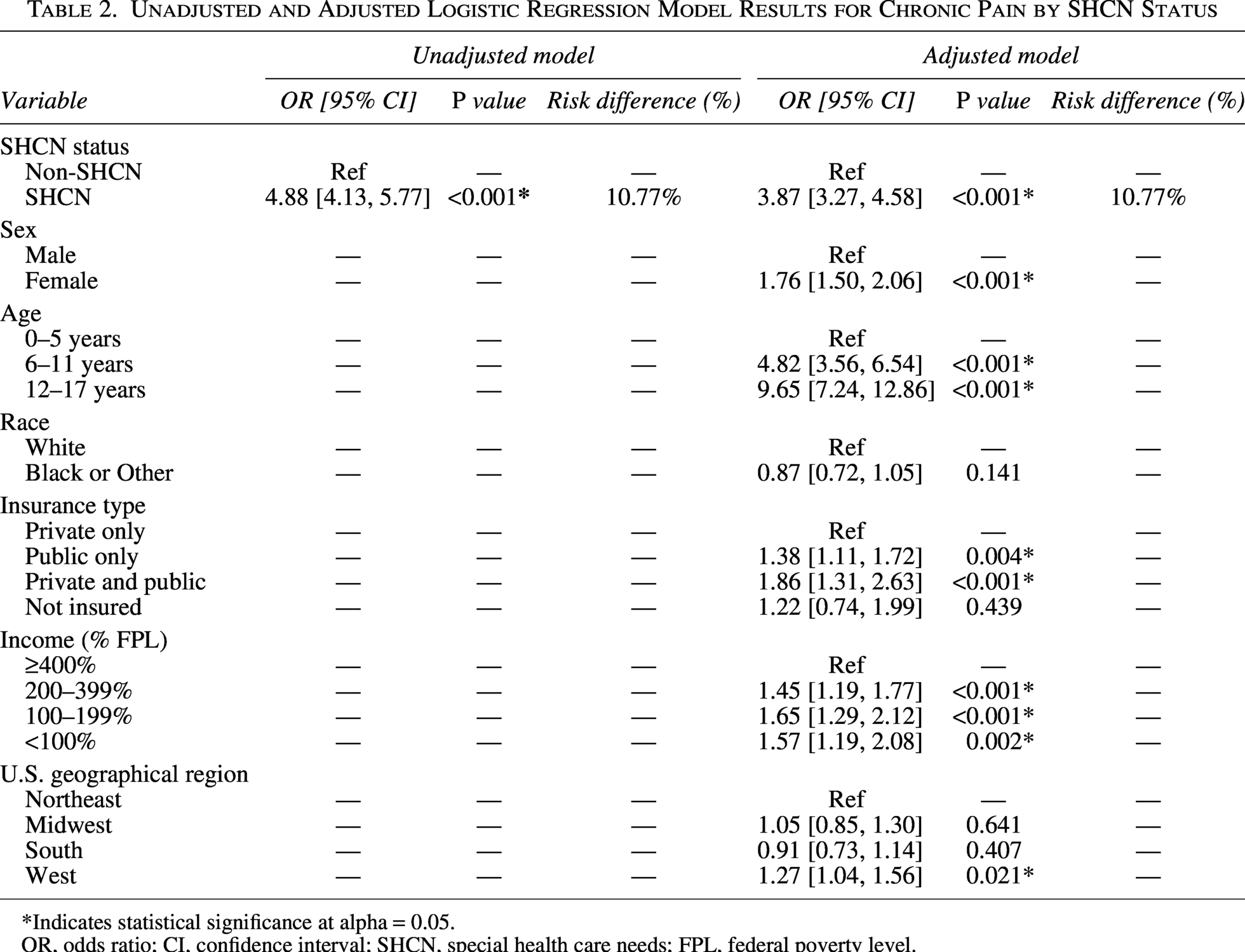
*Indicates statistical significance at alpha = 0.05.
OR, odds ratio; CI, confidence interval; SHCN, special health care needs; FPL, federal poverty level.
SHCN, chronic pain, and unmet health care needs
Unmet health care needs were rare for children with no chronic pain and without SHCN (1.7%). The rate of unmet health care needs was 7.2% for children with SHCN who had no chronic pain; whereas those with both chronic pain and SHCN had the highest rate of unmet health care needs (15.8%). For both children with and without SHCN, those with chronic pain had statistically significantly higher odds of reporting unmet health care needs than those without chronic pain (both P < 0.001) after adjustment for covariates. Those with both SHCN and chronic pain had 9.8 times the odds of reporting unmet health care needs compared with those without SHCN or chronic pain, after adjustment for covariates (P < 0.001) (Table 3). The adjusted predicted probability of unmet health care needs was substantially higher for those with both SHCN and chronic pain, while those with SHCN or chronic pain only showed more moderate increases. Significant covariates in the model included insurance type, income, and U.S. geographical region. Those who had public insurance, combination insurance (private and public), and were not insured had higher odds or reporting unmet health care needs than those with private insurance (all P < 0.01). Additionally, those with family income less than 400% of the FPL (all P < 0.01) and those in the West compared with the Northeast region of the U.S. (P = 0.036) had higher odds of reporting unmet health care needs.
Adjusted Logistic Regression Model Results for Unmet Health Care Needs by SHCN and Chronic Pain Status
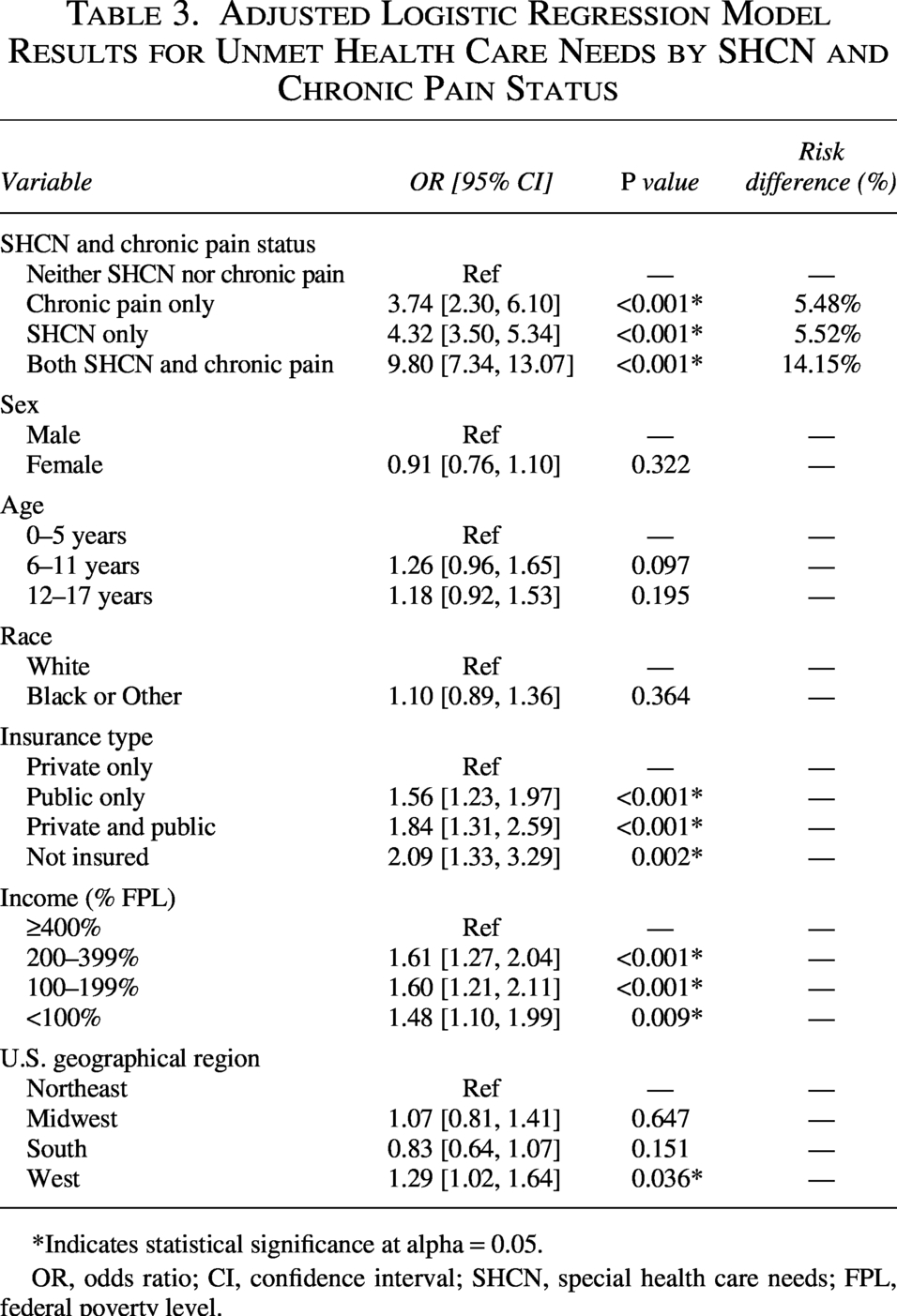
*Indicates statistical significance at alpha = 0.05.
OR, odds ratio; CI, confidence interval; SHCN, special health care needs; FPL, federal poverty level.
For those who reported having unmet health care needs, the top reasons for not receiving needed health care were problems getting an appointment, services not available in the area, and issues related to cost. Those with both SHCN and chronic pain were significantly more likely to have reported unmet health care needs due to problems getting an appointment (P = 0.002), services not available in the area (P = 0.001), office not open when child needed care (P = 0.029), and problems getting transportation or childcare (P = 0.006) compared with those without SHCN or chronic pain (Table 4). For those with both SHCN and chronic pain, the most common types of health care needed but not received were mental health (51%), medical (38%), and dental (38%).
Chi-Square Tests Results Examining Differences in Reasons for Needing Health Care but Not Receiving It by SHCN Status, Chronic Pain Status, and Their Combination. Values Represent Unweighted Frequencies and Weighted Prevalences
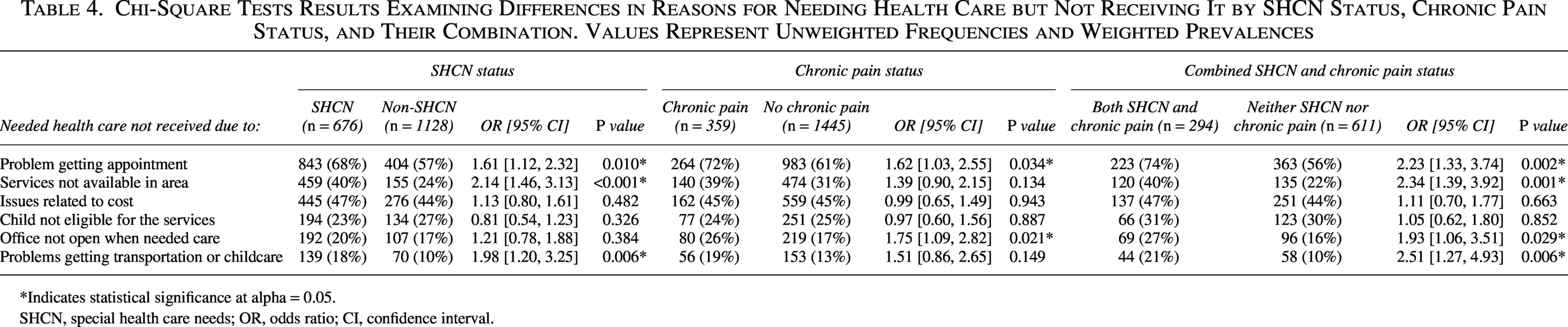
*Indicates statistical significance at alpha = 0.05.
SHCN, special health care needs; OR, odds ratio; CI, confidence interval.
Other health services utilization
For those with both SHCN and chronic pain, 45% saw a specialist other than a mental health professional, 53% needed a referral to see a doctor or receive services, and 22% used alternative health care or treatment compared with 7%, 13%, and 4% for those without SHCN or chronic pain, respectively. All differences were statistically significant (all P < 0.001). Those with SHCN only and those with chronic pain only were also significantly more likely to see a specialist, need a referral, and use alternative health care compared with those without SHCN and without chronic pain, respectively (all P < 0.001) (Table 5).
Chi-Square Test Results Examining Differences in Other Health Services Utilization by SHCN Status, Chronic Pain Status, and Their Combination. Values Represent Unweighted Frequencies and Weighted Prevalences
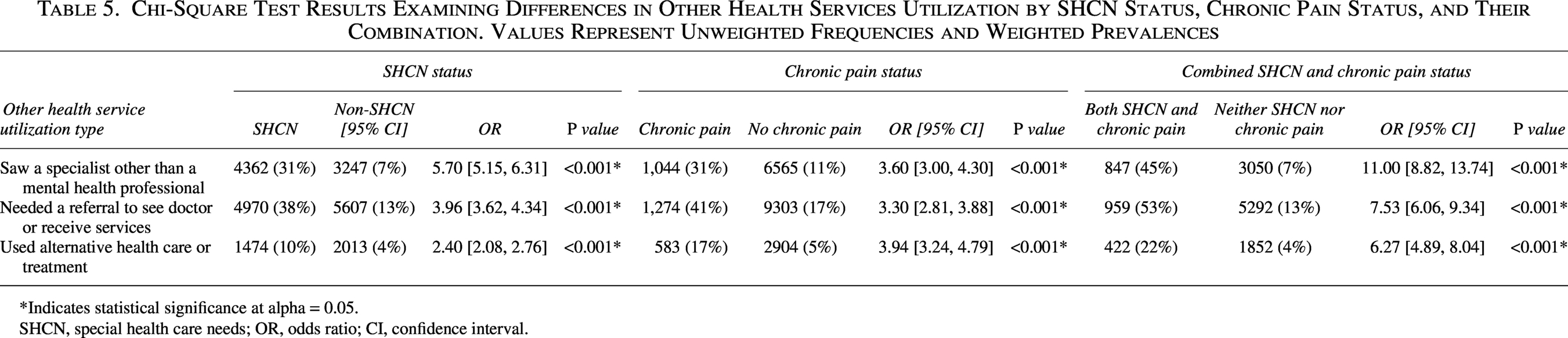
*Indicates statistical significance at alpha = 0.05.
SHCN, special health care needs; OR, odds ratio; CI, confidence interval.
Discussion
Most epidemiological studies of pediatric chronic pain have not specifically focused on children with SHCN or disabilities, nor have they used large, nationally representative, population-based datasets. This analysis, using data from a large, nationally representative sample of U.S. children, demonstrates that children with SHCN experience higher rates of chronic pain and that those with both SHCN and chronic pain have nearly 10 times the odds of reporting unmet health care needs compared with those without. Additionally, children with SHCN with chronic pain were more likely to report unmet health care needs due to problems getting an appointment, services not being available in the area, the office not being open when the child needed care, and problems getting transportation or childcare. There was greater reported use of other health service utilization in children with SHCN with chronic pain, with this population being more likely to see a specialist other than a mental health professional, use alternative health care or treatment, and need a referral to receive services.
Previous literature has shown that children with SHCN have higher health service utilization yet report greater unmet health care needs and face more disparities in access and quality of health care services compared with children without SHCN.3–5 Studies further suggest that the likelihood of unmet health care needs increases with the complexity of medical needs or the presence of multiple comorbid conditions.4,5 Additionally, those with disabilities related to pain are more likely to report unmet health care needs than those with other types of disability. 20 This aligns with the findings of the current study, which found that children with SHCN with chronic pain had significantly higher odds of reporting unmet health care needs. Understanding the underlying reasons for these barriers is critical, as unmet health care needs and poor access in childhood can lead to exacerbated medical issues and lower functional levels into adulthood.6,7 Consistent with prior literature among children with SHCN, the analysis identified a relationship between socioeconomic variables such as family income, insurance type, and geographical region and unmet health care needs.21–23 These findings also correspond with broader research demonstrating that social and community-level factors, such as social capital, may negatively impact health care access in this population. 24 Collectively, these findings align with Andersen’s behavioral model of health service use and underscore the importance of considering socioeconomic factors when developing targeted system-level policies and programs to reduce unmet health needs among children with SHCN with chronic pain. 19 However, despite adjusting for socioeconomic variables, children with both SHCN and chronic pain remained significantly more likely to report unmet needs, suggesting that additional barriers may play a role in limiting health care access.
This analysis found that children with SHCN with chronic pain were more likely to report unmet health care needs due to problems getting an appointment, services not being available in the area, the office not being open when the child needed care, and problems getting transportation or childcare. These barriers point to broader issues with service availability and accessibility at the time care is needed. This aligns with prior research in pediatric pain management, which highlights significant structural barriers to care that lead to high wait times and rates of unmet health care needs—including a limited number of specialized pain clinics, a shortage of trained professionals across overlapping medical subspecialties, and complex, often lengthy referral processes.25–27 One U.S.-based study of youth with chronic pain reported an average wait time of 6.5 months before initial evaluation. 25 This is particularly concerning, as previous literature has demonstrated that wait times exceeding 6 months are associated with declines in quality of life, worsening psychological well-being, and increased depression symptoms. 28 More broadly, untreated chronic pain has been linked to negative impacts on mental health, sleep, and personal relationships. 11 In this analysis, the most commonly reported unmet health care needs among children with SHCN with chronic pain were in the domains of mental health and medical care, consistent with literature showing associations between chronic pain and mental health challenges. These findings underscore the critical need to expand access to timely, high-quality pediatric pain management services, particularly for children with SHCN, who already face higher rates of unmet health care needs and have additional medical needs and complexity. Research has consistently shown that participation in multidisciplinary pediatric specialty pain clinics is associated with superior pain management, reduced emergency department visits, fewer hospitalizations, and lower overall health care costs.29–33 Meeting these unique health care needs this population may help reduce the burden of chronic pain, improve health outcomes, and decrease long-term health care utilization and costs. These findings collectively emphasize the need for timely and accessible care pathways for managing pediatric chronic pain, particularly among children with SHCN. In addition to highlighting gaps in care access, the current study also revealed patterns in health care utilization that may reflect attempts to navigate these barriers.
Specifically, the current study found that children with SHCN with chronic pain were more likely to see specialists, use complementary and alternative medicine (CAM), and require referrals to access needed services. This is consistent with previous research reporting that among individuals with chronic pain, those who reported unmet health care needs had more than twice the odds of utilizing CAM than those without unmet health care needs. 34 Other studies have similarly shown that children with chronic pain are more likely to engage in specialty care, use CAM, and seek emergency services compared with their peers without chronic pain.15,35 These patterns may reflect efforts to manage pain in the absence of coordinated or accessible care and align with prior literature that has shown a high prevalence of unmet need for care coordination among children with SHCN, further underscoring the high burden of unmet health care needs in this population. 36 The elevated use of emergency care in children with chronic pain highlights the potential consequences of untreated or poorly managed pain. Expanding access to specialty pediatric pain clinics may help reduce reliance on emergency services, improve symptom management, and enhance overall outcomes for children with SHCN with chronic pain. These strategies are particularly important for addressing the multifaceted care needs of this vulnerable group.
Limitations
A key limitation of the dataset is that chronic pain was assessed using a single parent-reported item, without information on pain type, location, frequency, or severity. This restricts the ability to characterize the nature and impact of chronic pain in this population. Including more detailed and validated measures of chronic pain in future iterations of the NSCH would significantly enhance the ability to examine pediatric pain experiences, both among children with SHCN and the broader pediatric population. Furthermore, because pain classification relied on parent report, it may not fully capture the child’s own experience, which can differ from caregiver perceptions. Lastly, while the current study focused the analysis on the broad population of children with SHCN, types of SHCN and specific conditions were not examined separately. Additional research is needed to better understand unmet health care needs specific to chronic pain management and how this may differ by type of SHCN, condition, or severity of pain.
Conclusion
This analysis provides nationally representative evidence that chronic pain is more prevalent among children with SHCN compared with their peers without SHCN in the United States. Moreover, significantly higher odds of reporting unmet health care needs among children with chronic pain were identified, with the highest odds observed in those who have both SHCN and chronic pain. These findings underscore the urgent need to address barriers contributing to these unmet needs, including long wait times and limited access to specialized pediatric pain care. Expanding and improving access to chronic pain treatment and management services—particularly for children with SHCN—may play a critical role in reducing unmet health care needs, improving health and quality of life outcomes, and decreasing long-term health care utilization and costs.
Authors’ Contributions
M.J.W. conceptualized and conducted the secondary data analysis, drafted the initial article, and critically reviewed and revised the article. C.C.B. critically reviewed and revised the article. R.G.C. critically reviewed and revised the article.
Ethical Considerations
This study was deemed exempt from requiring approval by the University of Minnesota Institutional Review Board due to all data being deidentified and publicly available.
Data Availability
All data used in the analysis are publicly available on the Maternal and Child Health Bureau’s National Survey of Children’s Health (NSCH) webpage [https://www.census.gov/programs-surveys/nsch/data/datasets.html].
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.