
Abstract
Holistic approaches to mental health that go beyond traditional medication-based therapies are often necessary for older adults (OAs). Forest bathing is a nature-based intervention that combines guided walks with mindfulness activities and has emerged as a complementary alternative to conventional therapies that promote mental well-being. However, most existing forest bathing programs are designed for the general population and may not adequately address the specific needs of OAs, particularly those experiencing mental health challenges. This feasibility study explored how forest bathing can be tailored for OAs. Using surveys, interviews, and focus groups with OAs (N = 15) and program delivery partners (N = 9), we found a synergistic effect of combining nature-based interventions with group-based program delivery. The program was seen by OAs as more than a nature experience, emphasizing improved social connection among those who experienced isolation and depression. The results highlight the importance of tailoring program content and delivery to accommodate diverse abilities, preferences, and life circumstances in later life. The study also proposes a practical implementation framework that integrates personal, social, environmental, and institutional dimensions to guide the design, adaptation, and integration of nature-based mental health programs for OAs.
Nature-based interventions are gaining increasing attention as innovative, sustainable approaches to support aging populations amid rising concerns and pressure on health care and social systems (Harper, 2014; Pretty & Barton, 2020). These interventions encompass structured activities that engage people with natural environments, including horticulture therapy, green exercise, and organized outdoor walking programs (Catissi et al., 2024; Keller et al., 2024; Nevo & Levin, 2025). They are also delivered through nature prescription/green social prescribing pathways, in which health care professionals or community providers refer patients to nature-based activities (Frost et al., 2023; Sun et al., 2023).
Evidence in older adults (OAs) indicates that participation in nature-based interventions can improve mental well-being and social outcomes, including reduced loneliness, particularly when programs are delivered in group formats that foster connection and mutual support (Lavelle Sachs et al., 2024; Tong et al., 2025). Policy initiatives, including the forest medicine approach in Japan and green social prescribing in the United Kingdom, have encouraged integration of nature-based programs into health and social care (DEFRA, 2020; Li, 2022; Yeo et al., 2020).
Within this broader field, forest bathing (Shinrin-yoku) has emerged as a structured nature-based program with promise in addressing mental health for OAs. It typically involves a guided, slow walk in a forested (or forest-like) environment, combined with mindfulness-based practices such as sensory invitations, periods of silence, and facilitated reflection (Hansen, 2018; Hansen & Jones, 2020; Timko Olson, Hansen, & Vermeesch, 2020). Current evidence suggests that forest bathing can produce short-term psychological benefits and acute physiological responses. Recent studies report improvements in affect, perceived stress, and psychological well-being after forest bathing experiences (Antonelli et al., 2022; Kotera, Richardson, & Sheffield, 2022). Forest bathing may also support well-being through social and relational pathways, as group-based participation can strengthen social connectedness and quality of life (Lavelle Sachs et al., 2024; McNeil, Singh, & Chambers, 2022).
Previous studies have also reported immediate postintervention changes such as reductions in blood pressure and stress-related biomarkers, and changes in inflammatory or immune markers after forest exposure (Li et al., 2025a, 2025b; Qiu et al., 2022). However, many of these effects of forest bathing are documented as immediate or short-term outcomes, and longer-term clinical and functional impacts remain less known (Hansen, Jones, & Tocchini, 2017; Stier-Jarmer et al., 2021).
Despite growing interest in forest bathing programs, OAs face barriers in participating in such programs, including mobility limitations and transportation constraints (Enssle & Kabisch, 2020). Additionally, programs developed for the general population may not adequately address OAs’ specific needs, which have implications for design and delivery. Prior research has identified individual-level barriers, including biophobia (fear of nature), anxiety and self-doubt, accessibility issues, and misconceptions about these practices (Clarke, Kotera, & McEwan, 2021). Research also highlights institutional barriers related to cost-effectiveness and assessment of target population needs in developing and implementing nature-based interventions (Taylor et al., 2022). While forest bathing is increasingly promoted as a complementary approach to traditional health interventions, few studies have examined how it can be adapted specifically for OAs or integrated into health care systems.
To address this gap, we conducted an exploratory feasibility study of a 4-week forest bathing program for OAs at Red Butte Garden in Salt Lake City, Utah. Using surveys, interviews, and focus groups with OA participants and delivery partners, we examined perceived benefits as well as practical barriers and facilitators to participation and delivery. The study aims to inform the development of accessible and sustainable forest bathing programs for OAs and proposes a practical implementation framework to guide future design, adaptation, and integration of nature-based mental health programs.
Methods
Study setting
The study was conducted at the Red Butte Garden, a large public botanical garden located in Salt Lake City, Utah, United States. The site featured both landscaped gardens and more naturalistic areas, offering diverse sensory and ecological characteristics. There is an admission fee to enter the garden, but the fees were waived for our study participants through the partnership between the garden and the research team.
Participant recruitment
Older adult participants
Between July and August 2023, OA participants (aged ≥65 years) were recruited through partnerships with local hospitals, clinics, educational institutions, and nonprofit organizations in the Salt Lake City, Utah area. Recruitment materials included a study website and flyers distributed at partner sites. Health care practitioners and staff also referred potentially eligible patients or clients by sharing the study website or research team email address. Interested individuals contacted the research team by phone or email, after which a team member explained the study, confirmed eligibility, and administered a brief screening questionnaire. Eligibility criteria for OA participants included: (1) being community-dwelling and aged 65 years or older, (2) English proficiency, and (3) ability to provide informed consent. During the initial telephone screening, a brief semantic verbal fluency task was administered as a cognitive screening test to ensure that study participants have sufficient cognitive capacity for meaningful participation. Of the 32 individuals who expressed interests, 15 met the study criteria. This study was approved by the University of Utah’s institutional review board (IRB #00159853). All participants provided informed consent prior to participation.
Delivery partners
We also recruited delivery partners to capture perspectives on the feasibility and integration of forest bathing in organizational contexts. Nine delivery partners were recruited from three professional groups: (1) health practitioners, (2) garden management personnel, and (3) senior living facility managers. They did not participate in the forest bathing sessions but shared perspectives on feasibility and integration within their organizations. Eligibility criteria required current employment in health care, garden management, or senior living facilities, actively involved in program planning, delivery, or management for OAs, and proficient in English. Although all our OA participants were community-dwelling individuals living independently, senior living facility managers were recruited as delivery partners to assess the potential for implementing forest bathing programs in a more managed care setting.
Recruitment was conducted using publicly available professional contact information and the research team’s professional networks. Potential delivery partners received an email outlining the purpose of the study and a link to contact the research team for further details. Interested individuals were scheduled for an informational call, after which consent was obtained.
Forest bathing intervention
OA participants engaged in a forest bathing intervention delivered weekly as a small group session (maximum seven participants) for 4 weeks in Fall 2023 (August and September) at Red Butte Garden. Each weekly session lasted 90–120 min and was led by a forest bathing guide certified by the Association of Nature and Forest Therapy Guides and Programs (ANFT), an official organization that trains forest bathing guides in evidence-informed, sensory-based forest bathing practices (ANFT, 2025). For every session, one research staff member accompanied the forest bathing guide to coordinate program delivery as well as to monitor participant safety and document participant behaviors.
Each session began with an introductory briefing, followed by the “Pleasure of Presence” stage (20–30 min), which is a sensory invitation encouraging slow, mindful engagement with immediate natural surroundings through visual, auditory, tactile, and olfactory awareness. OA participants then took part in a silent walk (30–40 min) known as “What’s in Motion,” which invited them to notice movement in the natural environment as a way of cultivating present-moment attention. The session concluded with a “Gratitude Circle” (20–30 min), during which they reflected on their experiences and shared insights over a tea ceremony. Figure 1 shows how these sessions were delivered in nature settings.

Photos capturing moments from the forest bathing sessions:
Data collection
Semi-structured interview guides were developed based on prior literature on nature- and group-based interventions with OAs and covered accessibility, social connection, and perceived therapeutic benefits. The interview guides were tailored separately for OA participants and delivery partners (Supplementary Data). Data collection comprised qualitative and quantitative components. Before the forest bathing session, research staff conducted preprogram telephone interviews with OA participants to understand motivations, expectations, and prior experiences with nature-based programs (30–40 min each).
After the OAs completed the sessions, we conducted postprogram interviews via Zoom (30–60 min) to understand their experiences and perspectives on forest bathing. Furthermore, two focus groups were conducted to allow OA participants to discuss various challenges and opportunities related to their experiences in a group setting. These in-person meetings lasted approximately 60–90 min, with all 15 OA participants attending one of two focus groups based on availability.
In parallel, Zoom interviews with delivery partners examined views on forest bathing, integration within existing programs, and logistical considerations for scaling (30–45 min). All interviews and focus groups were audio-recorded with participant consent, transcribed using a secure web-based tool (Otter.ai), checked for accuracy against the audio, and de-identified. Alphanumeric codes were assigned to OA participants (P01–P15) and delivery partners (S01–S9) to preserve anonymity.
In addition to the qualitative assessment, we administered the Patient Health Questionnaire (PHQ-9) to evaluate depressive symptoms (score range 0–27), with higher scores indicating greater symptom severity (Kroenke, Spitzer, & Williams, 2001). Severity categories were as follows: 0–4 (minimal), 5–9 (mild), 10–14 (moderate), 15–19 (moderately severe), and 20–27 (severe). The PHQ-9 scores were measured at baseline and postprogram to assess preliminary changes in mental health outcomes.
Older adult participant characteristics
Table 1 shows OA participants’ characteristics measured at baseline. The mean age of the participants was 74.6 years (standard deviation = 5.19). About half reported mobility limitations, 27% had difficulty walking, and 20% used assistive devices. Most OA participants were identified as White (93%), with a small representation of Asian individuals (6.7%). Income was categorized into broader socioeconomic groups to protect participant confidentiality given the small sample size.
Baseline Characteristics of Study Participants in the Forest Bathing Feasibility Program (N = 15)
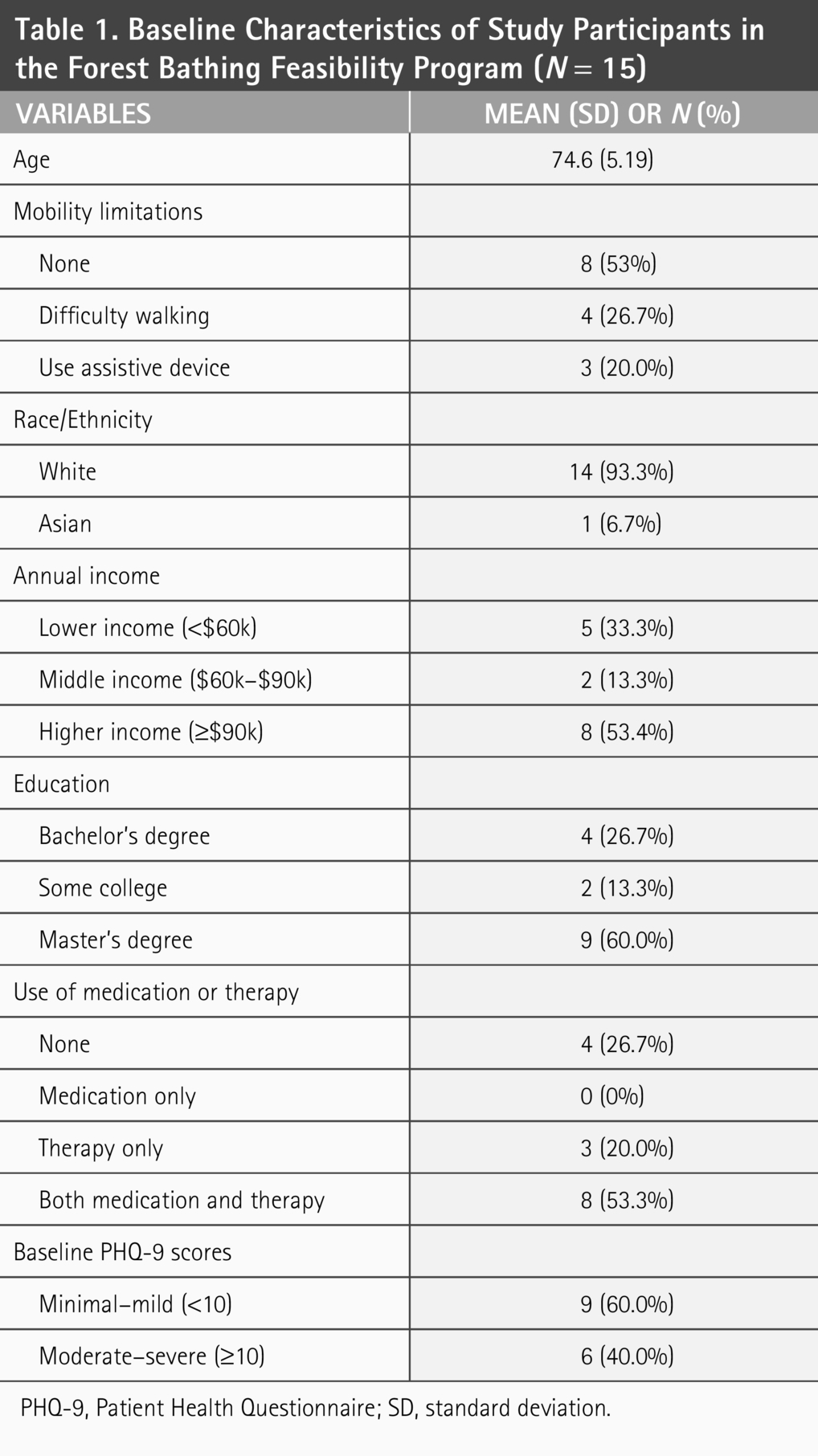
PHQ-9, Patient Health Questionnaire; SD, standard deviation.
About one-third (33.3%) were categorized as low income (<$60,000), 13.3% were middle income ($60,000–$90,000), and almost 53.3% were high income (≥$90,000). Regarding mental health treatment, 26.7% reported no current use of psychopharmacological medication or therapy, 20.0% engaged in therapy only, and 53.3% utilized a combination of both.
Data analysis
Descriptive statistics summarize baseline demographic characteristics. Quantitative analysis of PHQ-9 scores was performed using R version 4.3.2 (R Core Team, 2023). A paired samples t-test compared PHQ-9 total scores before and after the intervention. Exploratory analyses examined item-level PHQ-9 patterns and differential response by baseline symptom severity. Qualitative thematic analysis was used to identify feasibility-related themes from interviews and focus groups (Sandelowski, 2000). We used inductive coding for thematic analysis, with themes emerging from the data rather than from a predetermined framework.
A dual coding procedure was employed to ensure the reliability of qualitative analysis. Initial coding was done by a primary coder and independently verified by a secondary coder (Clarke & Braun, 2017). Discrepancies were resolved through discussion. To strengthen analytic rigor, the team collaboratively reviewed codes and themes using Miro (Miro, 2024), a digital whiteboard, for visual synthesis and refinement of codes and themes during analysis. Interview and focus group data were triangulated to synthesize overlapping perspectives between OAs and delivery partners (Korstjens & Moser, 2018). Data saturation was achieved when no new codes emerged, and thematic patterns recurred across the dataset (Morse, 2015).
Qualitative coding was done by two researchers (one non-Caucasian female and one Caucasian male) to improve the depth and breadth of the thematic analysis. Qualitative data were managed and analyzed using NVivo 12 (QSR International, 2018). The research team brought together interdisciplinary expertise in public health, gerontology, social work, and nature-based interventions. To ensure methodological rigor, the team maintained reflexivity through regular team discussions.
Results
Change in depressive symptoms of OA participants
The OA participants' mean PHQ-9 scores declined by 39% from 8.47 to 5.13 after program completion (t[14] = −4.58, p < 0.001). This represents a statistically significant reduction in depressive symptoms, with a large magnitude in change (Cohen’s d = 1.18) (Fig. 2B). On average, participants were within the mild range of depressive symptoms (PHQ-9 score of 5–9) at baseline, and after the program, almost all participants were approaching the minimal range (PHQ-9 score of 0–4). Of the 15 participants, 9 (60.0%) shifted to a lower PHQ-9 severity category after the intervention (33.3% from mild to minimal; 13.3% from moderate to mild; 6.7% from moderate to minimal; and 6.7% from moderately severe to moderate).
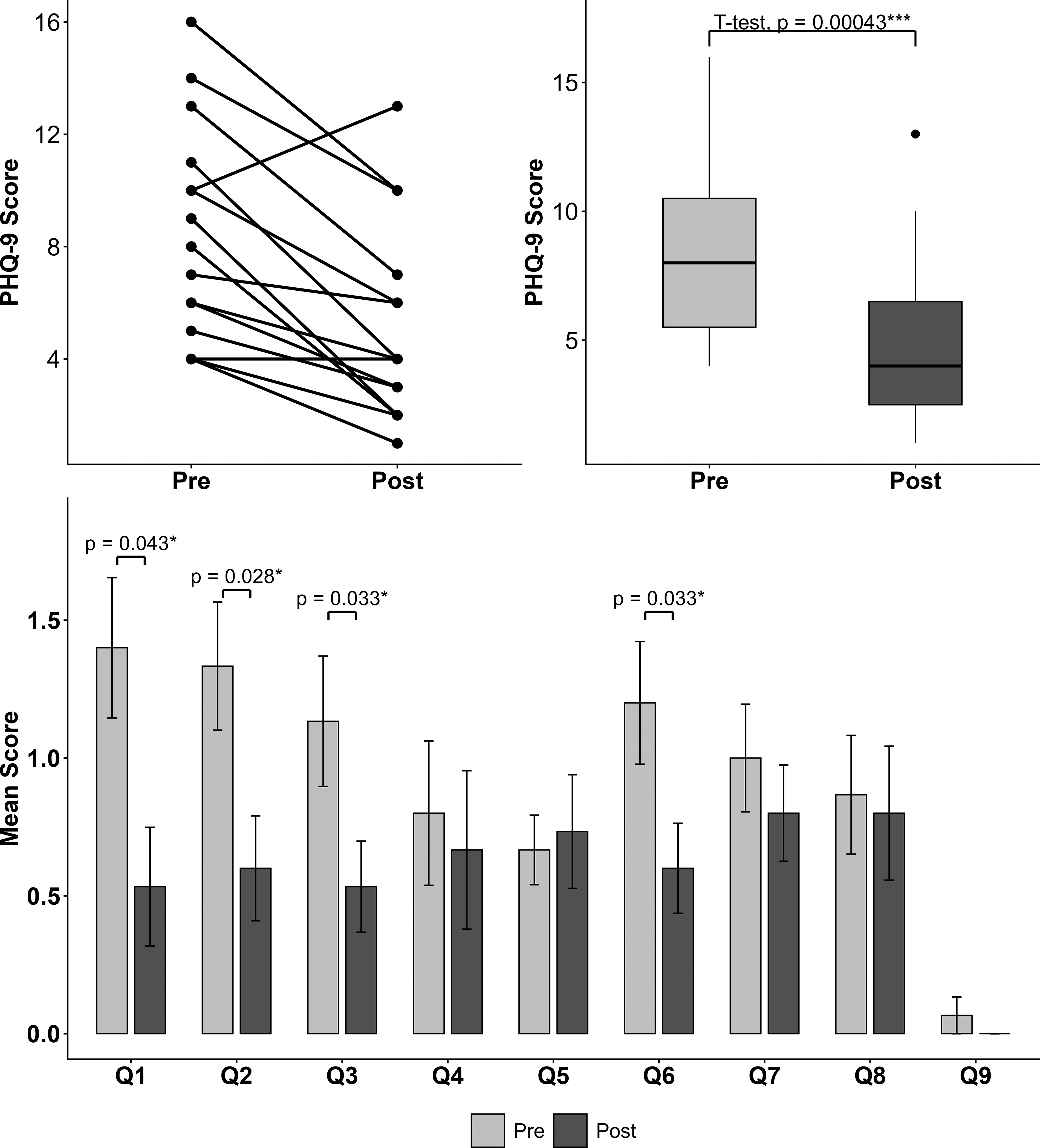
PHQ-9 scores before and after the forest bathing intervention.
Exploratory examination of individual items showed significant reductions in four symptom domains (Fig. 2C). The largest mean reductions were observed for anhedonia (Q1; mean change = −0.87, p = 0.043), depressed mood (Q2; mean change = −0.73, p = 0.028), sleep disturbance (Q3; mean change = −0.60, p = 0.033), and feelings of worthlessness (Q6; mean change = −0.60, p = 0.033). We also conducted an exploratory subgroup analysis to assess whether participants with higher baseline scores experienced greater reduction. Using a PHQ-9 score of 10 as a cutoff, OAs with higher baseline scores (≥10; n = 6) showed greater reductions in mean PHQ-9 scores than those with lower baseline scores (<10; n = 9) (reduction in mean PHQ-9 score: 4 vs. −2.89).
Qualitative findings
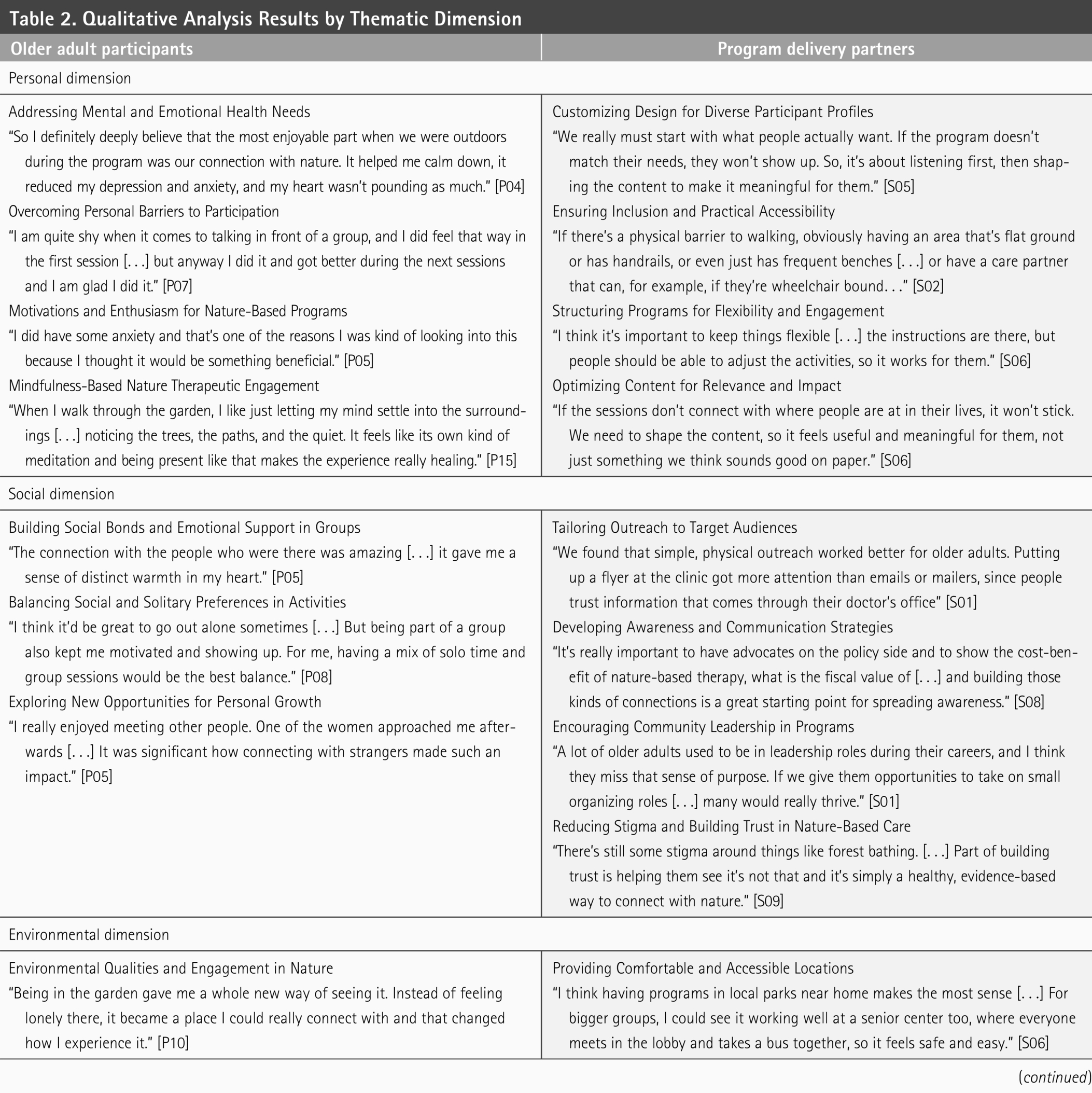
Drawing on interviews and focus groups with OA participants (N = 15) and program delivery partners (N = 9), we identified themes that clustered within four overarching dimensions (personal, social, environmental, and institutional). Subthemes within each dimension, together with representative quotes, are summarized in Table 2.
Qualitative Analysis Results by Thematic Dimension
Personal dimension: Mind–body needs, motivation, and person-centered engagement
OAs approached the program believing it had healing potential and were interested in new ways to improve well-being. Many expected time in nature to be restorative and were curious about non-pharmacological ways to feel better. Some of them were interested in learning how to address anxiety, depression, or stress. They also wanted to learn everyday self-regulation skills despite having no prior familiarity with forest bathing. For example, a participant explained: I do have some anxiety and depression. That’s one of the reasons I was kind of looking into this because I thought it would be something beneficial to […] help with that. I have never heard of forest bathing, but I personally feel more relaxed when I am in nature. (P05)
Throughout the interviews, OAs reported that forest bathing sessions helped them concentrate, relax, and learn mindfulness techniques they could apply in daily life. As one participant said, “I spend the same amount of time in nature as I did before, but now I’m more focused and aware of my surroundings, before I used to be caught up in my thoughts” (P02).
OA participants viewed the program’s therapeutic components (e.g., guided meditation and gentle movement) as a unique approach to supporting well-being and mental health. Some felt it complemented traditional treatments, while others preferred it over medication. As one person mentioned, “If I had an opportunity to do this enough, without medication, and found that my situation improved, I would certainly prefer this over medication to solve my problems” (P07).
Participants also identified several barriers that negatively influenced their engagement, including discomfort with prolonged sitting on the ground, hearing limitations, initial social hesitation, and fluctuating attention or energy. Preferences regarding the program structure varied: Some felt greater variety would make the sessions more effective, while others valued the repeated nature of the program for honing their skills in forest bathing practice. As one participant stated, “I would have preferred more diverse activities and a new narrative each session. However, I thought the reiteration of meditation was an important reminder” (P08).
Tailoring to personal characteristics was central to effective engagement. OA participants varied in mobility and functional capacity, hearing and sensory preferences, confidence in sharing, attention span, and prior exposure to mindfulness. They valued being able to pace themselves and choose their level of participation (e.g., silence versus discussion; gentler versus active movement). This was supported by clear step-by-step instructions and scheduling that aligned with their safety preferences. Delivery partners echoed this emphasis on person-centered adaptation, emphasizing the importance of understanding patients’ needs before offering the program: There is a lot of potential, but we must understand what their needs are first. That takes […] intentionality and patience to really understand them before offering any service. (S05)
Social dimension: Belonging, trust, and shared growth in group-based practice
The program extended beyond mental health benefits. Participants developed a sense of community and emotional support, leading to some level of social bonding after the program ended. OA participants described the warm and low-pressure atmosphere as making it easier to connect, check in on one another, and continue conversations beyond the sessions. As one person noted, “It’s very important to me to see nature, but I also love to say hello to strangers… not necessarily having big social connections, but it makes me feel good to see someone else feeling good” (P06). The group setting helped several people feel seen and encouraged, and some described this sense of belonging as therapeutic.
However, comfort with social interaction varied. Some preferred quieter, more reflective moments, while others enjoyed sharing stories and group discussion. For some OAs, the group format initially felt daunting, as mentioned by one person, “I didn’t like the sharing at first, to be honest. Sometimes it was like, ‘oh no, I said that too,’ and afterwards I would feel embarrassed” (P02). The sharing circle, where reflections were invited, created anxiety for some people. Sensory impairments such as hearing loss also limited their ability to participate in those interactive sessions.
Despite these varied preferences, OA participants appreciated the opportunity to alternate between group-based activities and quieter, reflective interactions. This alternating mode allowed them to engage in the program on their own terms, balancing social and personal preferences without pressure. As one participant put it: I see myself doing more quiet time and exercise on my own, but if it were only that, I wouldn’t follow through as much as I do when it’s social. I want to keep it as part of my routine but also look forward to meeting with others once in a while. I think both are important. (P13)
This flexibility opened space for personal growth, as participants tried new ways of connecting, practicing mindful listening, and discovering common ground with strangers. Building and sustaining these connections also depended on thoughtful communication.
Delivery partners also acknowledged the importance of the social dimension. They emphasized the need to leverage established community networks. Such outreach was deemed essential to validate the program, mitigate any stigma around nature-based care, and build trust among those who were unfamiliar or skeptical about the program: My mind goes to using the participants who have already engaged in the program. They know what it’s like and can speak about it genuinely. They have some sort of community connection and some trust among themselves, which they might not have with clinicians. (S01)
Delivery partners also emphasized incorporating purposeful social roles into the program to enhance its appeal. Providing opportunities for participants to play a small role could offer a sense of agency and participation, which are critical for sustained engagement. As one delivery partner stated, “They used to have these careers in which they were like leaders and had tasks and roles, I think they sort of miss that” (S06).
Environmental dimension: Therapeutic settings, access, and supportive design
OA participants consistently valued the sensory-rich natural setting of the garden including the greenery, flowers, and open views. The natural setting invited them to slow down and engage with their surroundings. Many described the garden as serene and welcoming, and framed nature itself as therapeutic and meaningful. As one participant who had tried their newly acquired forest bathing techniques at home explained: “At home, I’m just with my thoughts, I get distracted… here there are things I can listen to, touch or smell … I think the beauty and environment of the garden setting made it easier to focus” (P15).
At the same time, the physical landscape and logistics influenced participants’ level of comfort and willingness to attend. Barriers included low-light conditions, steep or uneven slopes, limited seating, and being unprepared for cold weather, which made some activities difficult or unappealing. Transportation, especially in the evening, was a recurring constraint for participants: “Just getting here and going back home… it was getting dark, and I had to drive through the city at night, which I really didn’t like!” (P02). Requests for daytime sessions and seasonal scheduling were tied directly to safety, visibility, and ease of access.
Delivery partners also emphasized the importance of aligning program site selection with OAs’ preferences and needs. Comfortable, accessible locations with clear pathways, stable surfaces, good lighting, and places to rest were viewed as important requirements. They also mentioned providing structural and interpersonal support including on-site wheelchair availability and caregiver assistance as needed. As one clinician explained: There are barriers to getting folks outside […] transportation, gear, and deeper issues like not feeling they belong in outdoor spaces. With seniors, make sure the ground is paved, wheelchairs are accessible, and having their care partner assist them. Just being flexible in terms of how they can participate is important. (S02)
Institutional dimension: Integration, credibility, and sustainable delivery
Delivery partners discussed the potential of incorporating forest bathing into existing health care practices. This would involve aligning organizational strategies and objectives with day-to-day operations and services. They also highlighted the value of institutional validation and formal endorsement. This includes obtaining accreditation from recognized health care or social service entities: Consider mental-health organizations… the APA, social work/psychotherapy association and even CMS (Centers for Medicare & Medicaid Services); they already endorse things like tai chi for fall prevention. See which groups have issued similar endorsements and start there. (S09)
Other important issues discussed by delivery partners included better communication, formal health care partnerships, sponsorships, and the use of digital platforms to build a supportive network around the program. As one partner noted: Utilizing community and senior centers and partnering with them in this program. Some of the local senior centers have hiking groups and some more ongoing outdoor programs. They are the concentrated area to reach older adults. (S08)
They also emphasized integrating the program into existing clinical and organizational systems through care-plan workflows or wellness referrals so that forest bathing can be offered and tracked like any other service. As one clinician noted: We already refer to community programs in Epic/MyChart;
1
a wellness referral could easily include forest bathing. The workflow is there, [but] the challenge is getting clinicians to put the order in. (S09)
Some clinicians added that moving the program from pilot to service requires defining the target population and outcomes to support sustainability. Furthermore, successful implementation in managed care settings depends on operational readiness. Senior living managers noted that programs must be supported by enough on-duty staff, aligned with existing facility schedules, and comply with required staffing mandates.
Two elements stood out for sustaining implementation: viable financing and proof of impact. Delivery partners proposed blended and innovative funding sources (e.g., insurance where possible, institutional support or scholarships, or small incentives) paired with routine outcome monitoring and peer-reviewed evidence to secure leadership support for forest bathing. As one clinician put it:
“Would a payer like Blue Cross 2 cover this? They’ll want evidence. Fewer hospitalizations/ER visits, reduced depression service use, people staying at work. The key is whether this is prevention, treatment, or both” (S04).
Program quality was also viewed as crucial for adoption into routine care. Key facilitators of integration include the provision of therapeutic and inclusive structures that offer flexible participation options. Clear guidance and accessibility across varying levels of physical and cognitive ability were viewed as prerequisites for scalable implementation. Another important issue, especially with OAs, was caregiver engagement.
Delivery partners advocated treating caregivers as integral stakeholders and bringing them on board early. As one delivery partner noted, success depends on “getting the care partner on board, … making sure consent and up-to-date contacts are in the chart, and using whatever channel actually reaches them” (S06).
Discussion
This study examined the feasibility of developing forest bathing programs for OAs. Preliminary PHQ-9 results showed that this pilot program significantly reduced depressive symptoms among participants, suggesting its potential as a therapeutic tool for OAs’ mental well-being. Exploratory subgroup analysis indicated that OAs with higher baseline depressive symptoms (PHQ-9 ≥ 10) experienced larger reductions in mean scores compared with those with lower baseline scores (−4 vs. −2.89). This pattern is consistent with evidence suggesting that individuals with higher baseline symptom severity tend to demonstrate greater treatment responsiveness (Cuijpers et al., 2013). This is also supported by existing theories of nature-based interventions, which propose that individuals experiencing higher distress may benefit more from restorative natural environments (Kaplan, 1995; Ulrich et al., 1991). While these quantitative results are encouraging, qualitative analysis revealed several challenges that must be addressed to ensure effective implementation across personal, social, environmental, and institutional (PSEI) dimensions.
First, tailoring the forest bathing program to individual needs and abilities was identified as essential for engagement and accessibility (personal dimension). OA participants faced varying mobility limitations and cognitive impairments, which influenced their ability to fully participate. Assessing OAs’ activities of daily living (ADLs) and instrumental activities of daily living (IADLs) may provide a systematic way to evaluate functional capabilities and design suitable nature-based programs (Hopman-Rock et al., 2019; Seidel et al., 2010). Assessment tools within the ADL/IADL criteria, such as the Functional Autonomy Measurement System, Functional Independence and Difficulty Scale, and Barthel Index, can also help tailor interventions and track progress (Toto et al., 2013). OA participants and delivery partners also emphasized aligning activities with cultural backgrounds, personal preferences, and previous experiences with nature. These considerations may foster meaningful engagement and strengthen “person-environment fit”, which is critical for motivating and sustaining participation (Jao et al., 2021). Taken together, these findings suggest that a hybrid delivery model accommodating both individual tailoring and group-based participation may be most effective, particularly for OAs experiencing both depression and social isolation.
Second, OA participants described forest bathing as extending beyond mental health benefits by fostering a sense of community and belonging (social dimension). They reported increased social connection through group activities, which has the potential to address social isolation among OAs (Forsman et al., 2013; Koehn, Ferrer, & Brotman, 2022). The group-based format of the program encouraged participants to interact, share personal experiences, and build empathy, supporting meaningful connections in a nature-based setting (Joshi, Finney, & Hale, 2025; Watt et al., 2024). The synergy between group dynamics, natural environments, and community engagement was reported to enhance the program’s effectiveness, promoting well-being through shared experiences (Berlin & Perone, 2024; Duvall & Kaplan, 2014). Participants also reported a heightened sense of peace in nature, aligning with evidence that natural environments can help combat social isolation among OAs (Finlay et al., 2015). Future research should examine the synergistic effects of group dynamics, natural environments, and community engagement.
Third, the natural environment was reported to create a welcoming space for OAs to share personal experiences and build social connections (environmental dimension). Our findings suggest that forest bathing may complement traditional mental health treatments, particularly for OAs with mild depression, by leveraging nature’s healing properties. However, most existing studies on forest bathing have focused on nonclinical or mildly symptomatic populations, and evidence regarding OAs with moderate to severe depression remains limited (Kotera et al., 2022).
Our findings further suggest that the natural surroundings of the study site enriched sensory engagement and promoted a deeper sense of connection to both nature and other participants (Nevo & Levin, 2025). These findings align with research showing that mindfulness practices are more effective in natural settings, where focused attention and stress reduction are amplified (Buse et al., 2024; Nabhan et al., 2020). Nature-based interventions have also been shown to reduce rumination and improve mood more effectively compared with indoor settings (Lipponen et al., 2022; Naor & Mayseless, 2021). These interventions may be more cost-effective than traditional therapies in improving mood and well-being, implying the potential for equal or even greater effectiveness in managing emotional distress (Capaldi et al., 2015).
Finally, delivery partners described broader considerations such as program accreditation and institutional support as crucial to wider adoption of forest bathing programs within health care systems (institutional dimension). Successful adoption of forest bathing programs depends on organizational readiness, cultural alignment, and the willingness of institutions to integrate non-traditional interventions into existing services. While this research was not formally structured as an implementation study, our findings closely align with the RE-AIM implementation framework, a model designed to bridge the gap between research and real-world impact (Glasgow, Vogt, & Boles, 1999). Specifically, our results highlight factors critical to adoption (the willingness of organizations to initiate the program) and maintenance (the long-term integration of the program into routine care). Our findings suggest that programmatic adaptations, such as the integration of cultural elements, tailoring delivery methods, and alignment with participant preferences, can enhance adoption by demonstrating the intervention’s flexibility and relevance to OAs (Nhim et al., 2019).
The need for program standardization also emerged as essential for sustaining implementation beyond the pilot. Standardization facilitates integration into existing wellness interventions, psychological therapies, or social care services. To ensure long-term success, future forest bathing programs should prioritize embedding programs in organizational practices, providing staff training, fostering community partnerships, securing funding, and using targeted health promotion strategies (Racey et al., 2021).
Limitations
Several limitations of this study should be noted. First, the small sample size (N = 15 OA participants; N = 9 delivery partners) limits statistical power and generalizability. The PHQ-9 findings should therefore be interpreted as preliminary given the limited power to detect small effects. Second, the sample was predominantly White (93.3%) and higher income, likely reflecting the broad demographics of Salt Lake County (86.9% of adults aged 65+ identify as White [U.S. Census Bureau, 2020]), which limits transferability to more diverse urban contexts. Future research should prioritize purposive sampling and inclusive recruitment to assess the intervention’s applicability across more diverse populations. Third, we did not examine seasonal challenges (e.g., winter snow or summer heat) that may influence the forest bathing experience. Future research should assess adaptability across seasons and geographic contexts.
Conclusions
Our findings demonstrate that forest bathing offers a promising and sustainable intervention for addressing social isolation and mental well-being in OAs. Forest bathing not only leverages the restorative properties of nature but also fosters a sense of community and belonging among participants. Unlike clinical settings, the welcoming atmosphere of nature encourages open communication and social connection among participants. By identifying critical PSEI dimensions, this research provides a holistic framework for the adaptation and integration of nature-based interventions into formal health care systems. Our findings suggest that while personal adaptations are important for making the program more inclusive, institutional-level standardization and accreditation emerge as critical components of systemic adoption. Integrating these PSEI dimensions into established implementation models (e.g., RE-AIM) offers a rigorous and scalable pathway for transitioning nature-based therapies from pilot interventions into more mainstream health care practice.
Authors’ Contributions
A.H.: Conceptualization, supervision, methodology, formal analysis, writing—original draft, writing—review and editing, project administration, and funding acquisition. T.M.H.: Methodology, investigation, formal analysis, writing—original draft, and writing—review and editing. M.E.: Formal analysis and writing—original draft. V.G.: Conceptualization, funding acquisition, methodology, and writing—review and editing. S.C.: Conceptualization, funding acquisition, methodology, formal analysis, and writing—review and editing. A.R.: Conceptualization, funding acquisition, methodology, and writing—review and editing. M.S.: Conceptualization, funding acquisition, methodology, and writing—review and editing.
Footnotes
Data Availability
The authors do not have permission to share the data. The interview transcripts are protected under IRB/ethical restrictions and cannot be made publicly available.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This work was supported by funding from the Nature and Human Health Utah (2022). No grant number was assigned to this funding.