
Abstract
Study Design
Retrospective cohort review.
Objective
To investigate the relationship between falls from height and facial injuries.
Methods
This is a retrospective cohort study, conducted over a 7-year period, of the medical records of all patients who presented to hospital for a maxillofacial injury following a fall from height. Fall heights were classified as low falls (1–3 m), high falls (3–10 m) and very high falls (≥10 m).
Results
A total of 111 patients with 218 facial bone fractures were identified (78 men, 33 women and mean age 50.3 years). High falls were the most common (n = 58, 52.3%). Multiple fractures were identified in 51 (46.0%) patients. Orbital and middle third fractures were the most prevalent. Nasal, mandible, bilateral and fractures involving more than one facial third, increased as fall height increased, as did the requirement for operative fixation. The majority of patients had an associated injury (n = 100, 90.1%) and overall mortality was 6.3%.
Conclusions
Falls from height are prevalent and there is a trend towards increased severity of facial injury, surgical intervention and associated morbidity as fall height increases. Falls from height are a significant public health concern and an important facet of maxillofacial trauma to recognise, as is the requirement for an interdisciplinary approach as they present to hospital.
Introduction
Falls are a major cause of injury in communities. They can result in serious morbidity and mortality. As such, they are a significant public health concern and are a frequent cause of emergency department presentation and hospitalisation. 1 In developed countries, the prevalence of injuries from falls is surpassed only by injuries that result from motor vehicle accidents. 2
A variety of circumstances can predispose to a fall and the resultant trauma can be classified as being due to either a same level fall (SLF) or a fall from height (FFH). A SLF is generally the result of either a mechanical slip or trip or medically associated with fits, faints or funny turns. A FFH may be considered as either accidental or intentional and can be reasonably quantified as either metres or floors above ground.
2
Unfortunately, there would appear to be no standard classification that is consistently applied across the range of health care delivery systems to stratify the fall height. A practical stratification might be based on SLF, low falls (LF) (<1 storey,
Despite the ubiquitous nature of falls across the community, there would appear to be a paucity of studies in the literature regarding the nature of FFH and in particular as they present to oral and maxillofacial surgery units.3-10 An understanding of the pattern of injury and outcomes of facial injuries sustained from FFH may be useful for treatment and also prevention. 11 We therefore believe that it is timely to investigate this aspect of facial trauma. The purpose of this study is to investigate specifically, the relationship between FFH and those patients who sustained a resultant facial injury and who attended a level 1 trauma centre. The hypothesis is that there are a demonstrable number of such FFH and that the fall height may reflect both the extent of facial and other injuries as well as the clinical significance of the injuries.
Methods
To address the research purpose, the authors designed and implemented a retrospective cohort study of the medical records of all patients who attended our level 1 trauma hospital and whose mechanism of injury was registered as a FFH.
The study was conducted between January 2013 and December 2019. The main inclusion criteria consisted of patients who had suffered a FFH, who were evaluated by the trauma service and who were subsequently consulted by the oral and maxillofacial surgery service. This cohort excluded patients who sustained SLF. It also excluded patients not involved with the trauma service and where our department was consulted directly, as almost all FFH resulted in an initial major trauma call and we currently do not have an accessible data registry similar to that of the trauma service. The data collected included the patient’s age, gender, fall height, injury pattern, management, length of admission and outcome. Patients meeting the following specific criteria were included: primary mechanism of injury registered as a FFH; evaluation by the trauma service with subsequent consultation by oral and maxillofacial surgery; and sustained a facial injury.
The primary predictor variable was the fall height. This was collected as a continuous variable and then categorised into LF (1–3 m), HF (3–10 m) and VHF (≥10 m). The primary outcome variable was the pattern of facial bone fracture. Fractures were classified as frontal, nasal, orbital, zygomatic, maxillary and mandible. These categories were not mutually exclusive. In addition, fractures were classified according to involved facial thirds (upper, middle and lower) and whether they were either bilateral or unilateral. Co-primary outcomes included the need for operative management, length of admission and mortality. The secondary outcome variable was the presence of associated injuries. These were classified as cranial, ocular, thoracic, abdominal and orthopaedic.
Descriptive statistics were presented as numbers (percentage) for categorical data, mean (standard deviation) for continuous parametric data and median (interquartile range, minimum/maximum) for non-parametric data. Mantel–Haenszel chi-squared statistics were used to test for an association between the fall height, as an ordinal categorical variable, and the primary and secondary outcomes. Two-tailed P-values were set at <.05 for statistical significance. Analysis was undertaken using SAS Studio 9.4 (SAS Institute Inc, Cary, NC).
The study protocol was granted authorisation as a negligible risk research activity not requiring approval from a human research ethics committee (Hunter New England Health Authorisation Number AU202009-08).
Results
A total of 11 707 trauma presentations to our level 1 trauma hospital were identified between January 2013 and December 2019. Of those, 2138 (18.3%) were due to a FFH and 111 (1.0%) sustained a facial injury as the result of a FFH.
Characteristics of Patients Sustaining a FFH and Facial Injury.
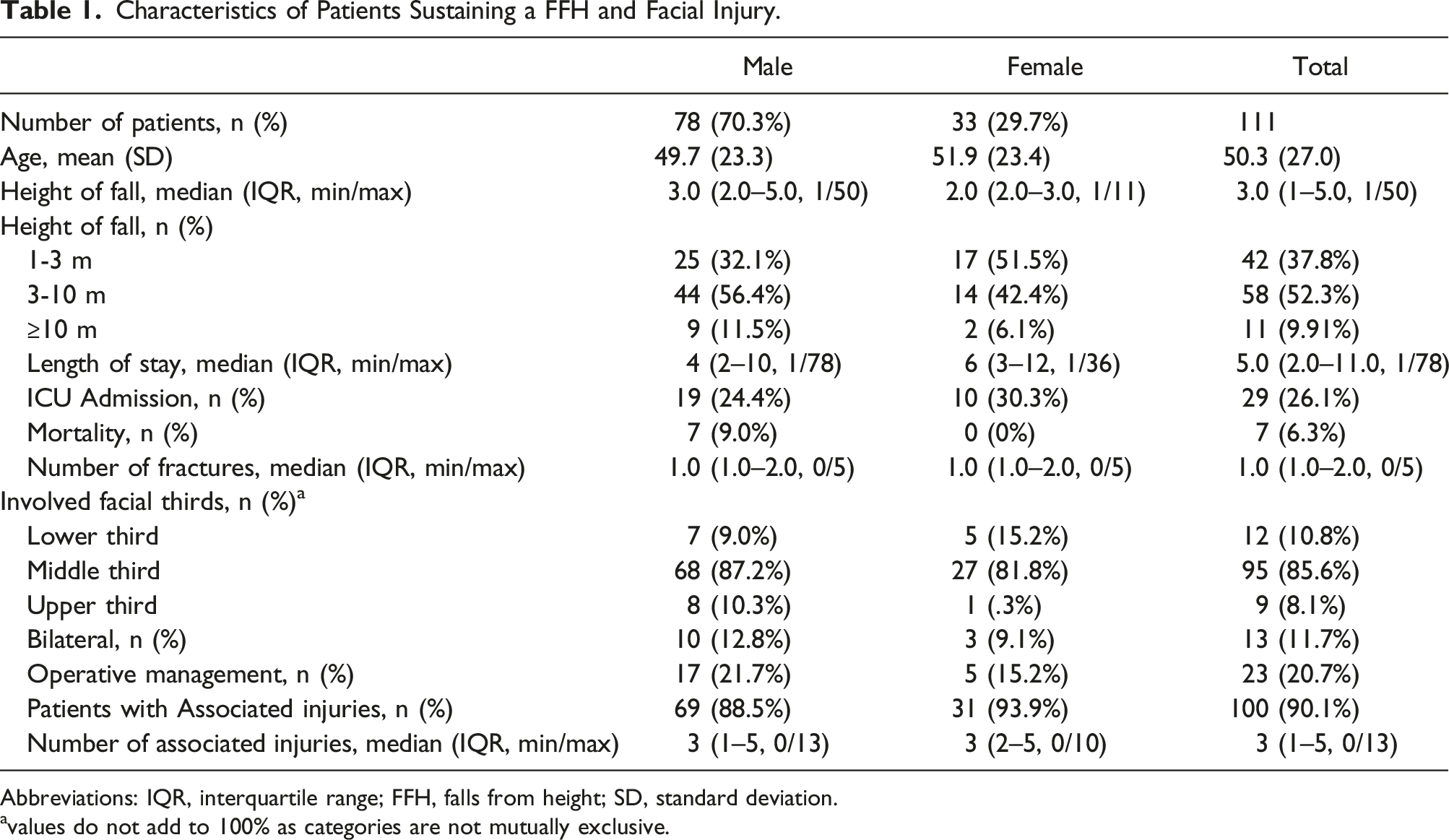
Abbreviations: IQR, interquartile range; FFH, falls from height; SD, standard deviation.
avalues do not add to 100% as categories are not mutually exclusive.
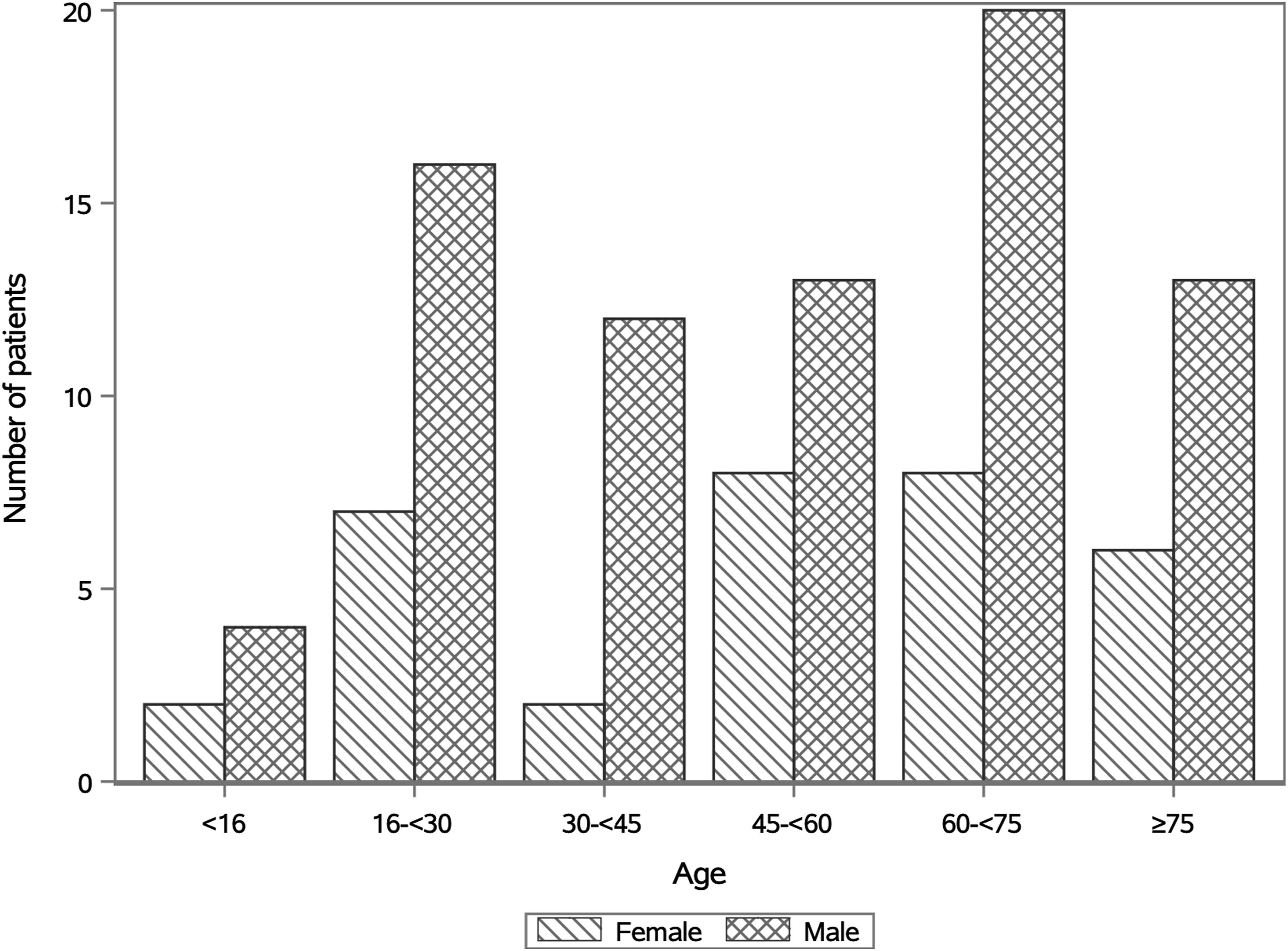
Patient distribution according to age and gender.
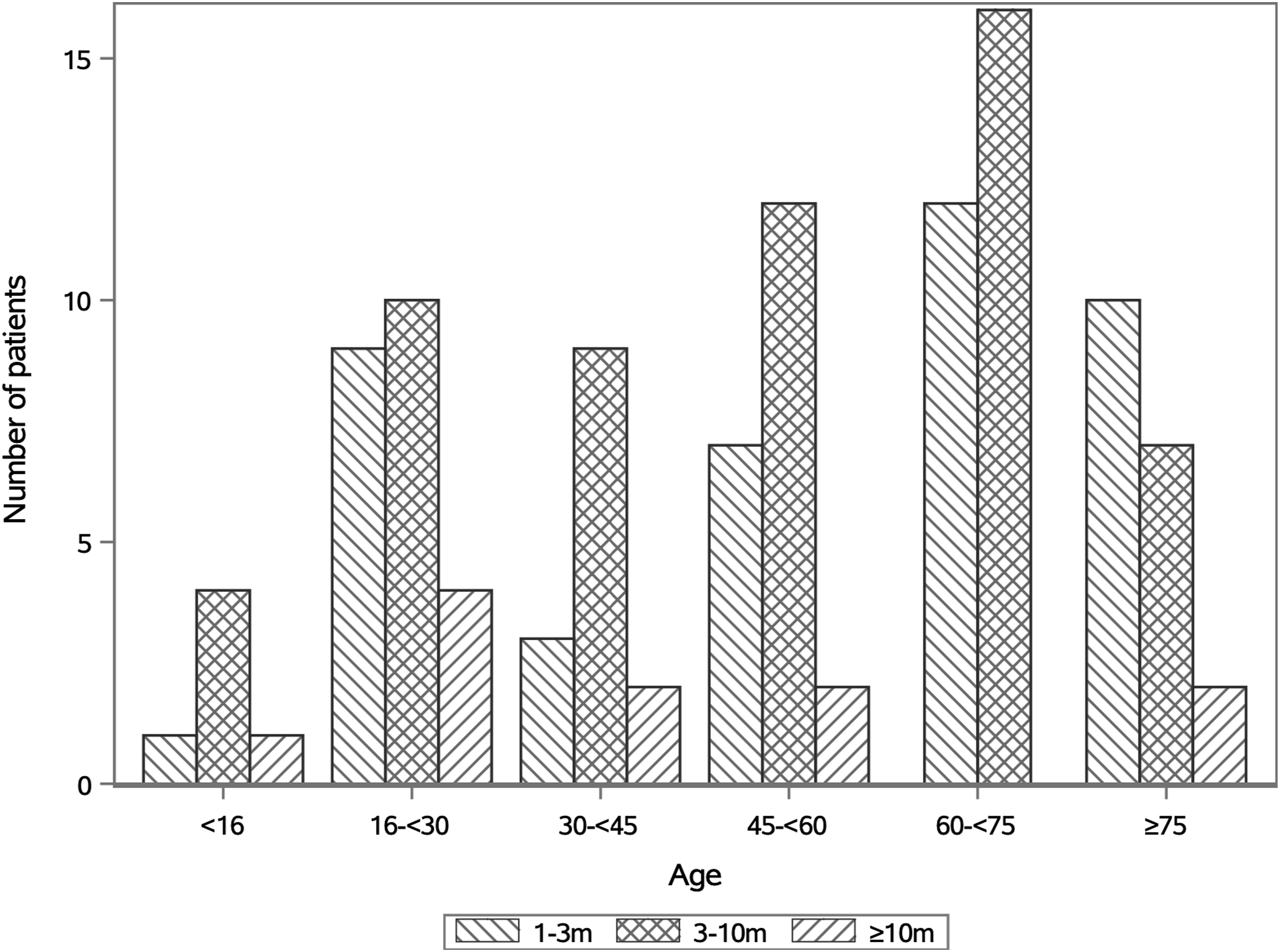
Comparison between fall height and patient age.
Association Between Fall Height, Pattern and Outcome of Facial Injuries.
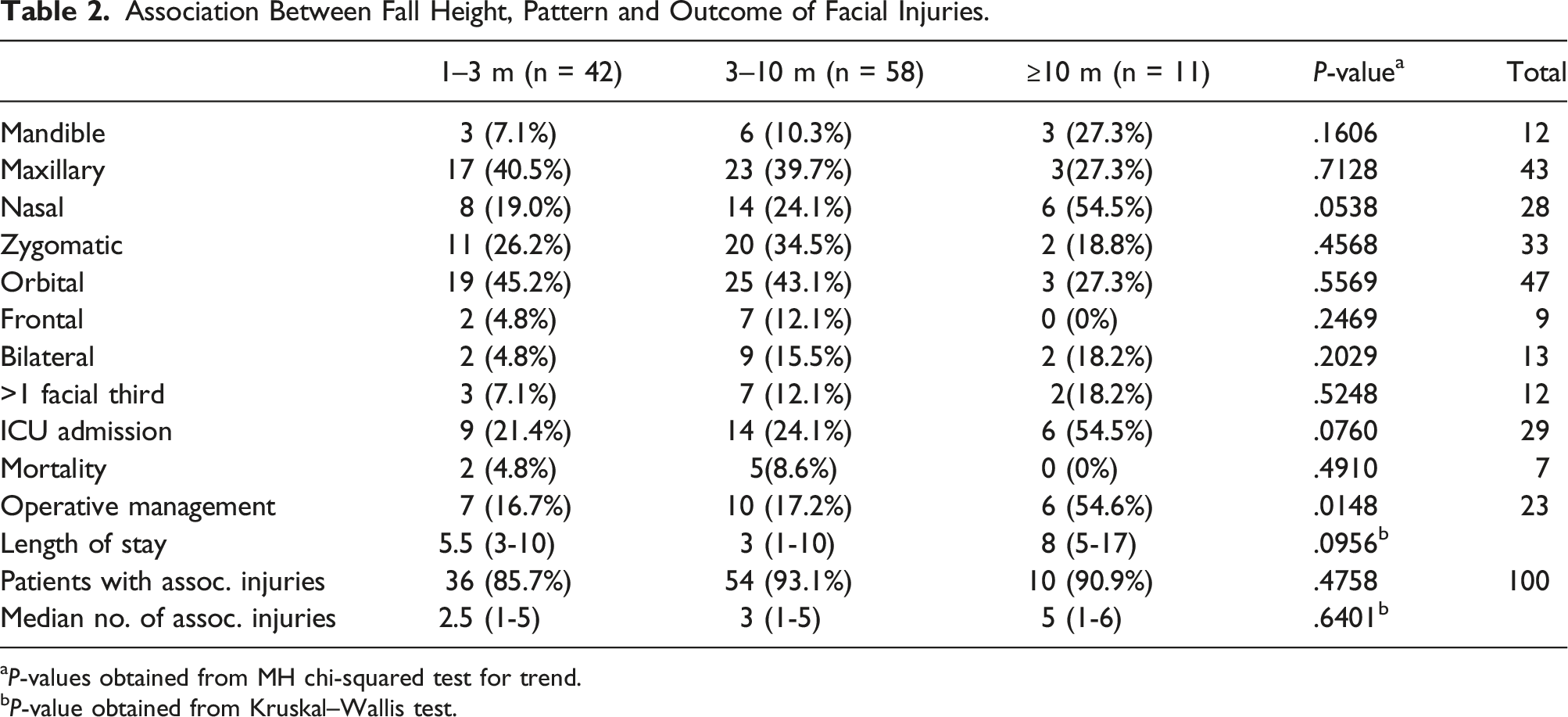
aP-values obtained from MH chi-squared test for trend.
bP-value obtained from Kruskal–Wallis test.
The majority of patients had an associated injury (n = 100, 90.1%). Of those patients who fell from a LF, 85.7% had at least one associated injury, compared with 93.1% of people who sustained a HF and 90.9% of people who sustained VHF. The median number of associated injuries was 2.5 in LF, 3.0 in HF and 5.0 in VHF (Figure 3). Cranial injuries, which included concussion, were the most common type of associated injury followed by orthopaedic injuries (Table 3). The incidence of these did not vary significantly with the fall height. Ocular injuries occurred rarely (n = 3, 2.7%). Abdominal injuries were also uncommon, however, were significantly associated with increased fall height (P < .001). There was a trend towards an increased incidence of thoracic injuries as fall height increased (9.5% for LF, 12.1% for HF and 36.4% for VHF); however, this was not statistically significant. Associated injuries and fall height. Patient With Associated Injuries According to Fall Height.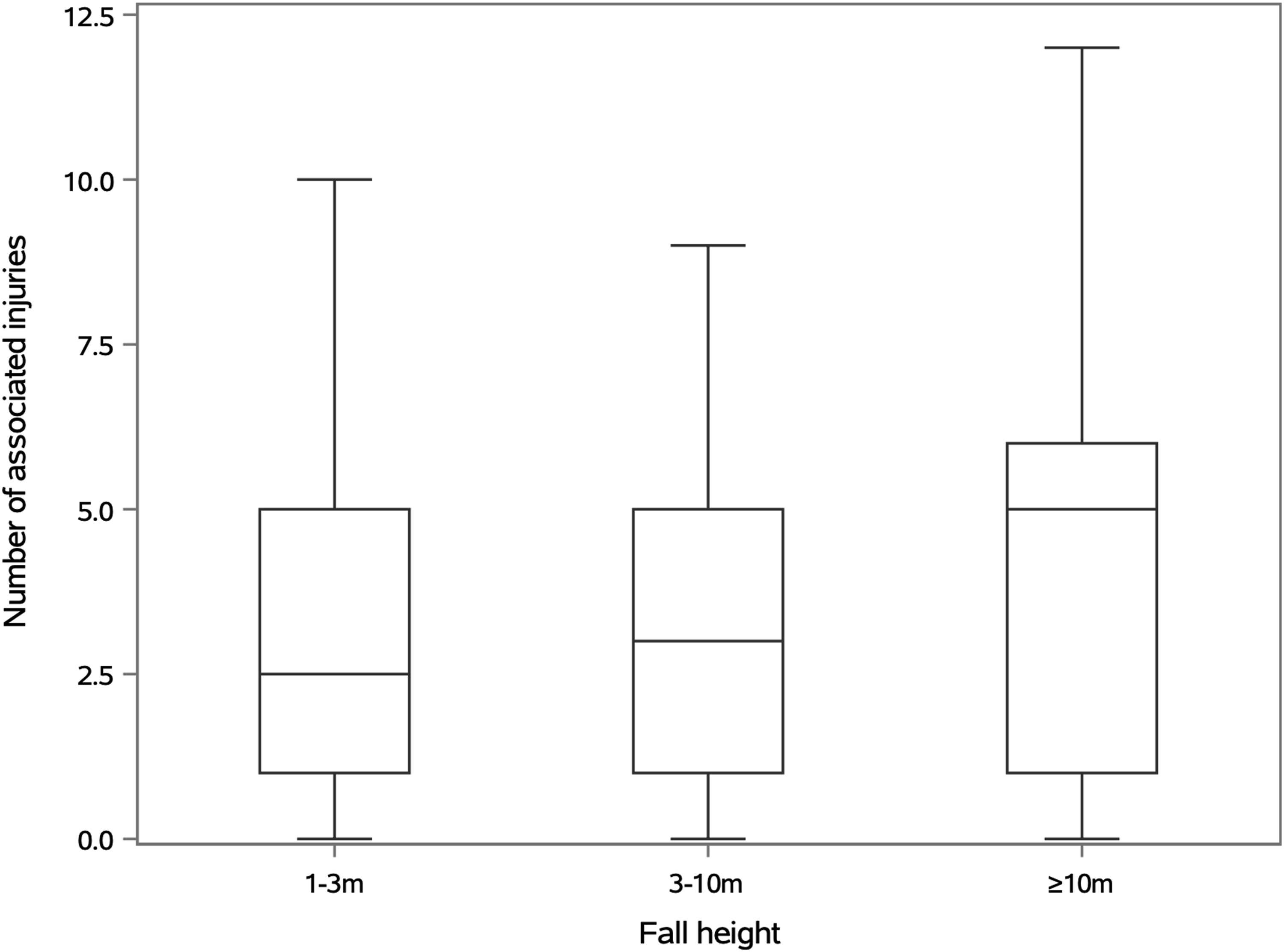

Discussion
Facial injuries that result from a FFH are a common occurrence. Our institution is a level 1 trauma centre where our department is responsible for the management of all facial trauma from urban metropolitan and rural and remote areas, including both paediatric and adult patients, with a catchment population of over 1 million people. During the study period, the average yearly incidence of facial bone fractures from all trauma was 10.5 per 100 000 persons. The yearly incidence of facial bone fractures from a FFH specifically, was 2.4 per 100 000 persons. A FFH is usually associated with work activities, recreational pursuits and suicide attempts. According to Safe Work Australia, a FFH was the cause of 11% of all work-related deaths and half of these involved heights of 3 m or less. 12 Approximately 9% of all worker hospitalisations were due to a FFH. Moreover, 25% of all falls-related claims resulted in fractures, culminating in an average of 6.2 weeks off work. This highlights the public health implications surrounding FFH and their associated injuries, both from a health and economic perspective.
An understanding of facial bone fracture patterns resulting from a FFH as they present to trauma and oral and maxillofacial surgical units is equally as important, as is recognising the impact such injuries have on patients and the health care system. The majority of FFH are accidental and occur in the workplace, whilst intentional falls or suicide attempts tend to occur from higher distances. 13 As with all facial trauma, alcohol and illicit drugs also play a significant role in the aetiology of falls.14-16 The kinetic energy absorbed by a person falling is determined by the fall height and the stopping distance. This, together with the position of landing, the region of contact and the surface of impact, all determine the pattern and severity of injury. 17
In our study population, FFH were most common amongst men, with more men falling compared to women in all age groups and all categories of LF, HF and VHF. The highest number of FFH occurred in the 60–74 year age group for both men and women, followed by the 16–29 year age group for men. This bimodal distribution can possibly be explained by the risk factors that are inherent to falls in the elderly and that younger men are more likely to be involved in lines of work involving heights as well as engaging in risky recreational behaviour. This is further reinforced by the fact that the highest number of VHF occurred in the younger 16–29 year age group and the highest number of LF and HF both occurred in the older 60–74 year age group. Furthermore, no VHF were recorded in the older 60–74 year age group. High falls were the most frequent in our study population with a median fall height of 3 m. LF were the most frequent in the 75 and older age group, reflecting the lower likelihood of this age group to be involved in employment and recreational activities at heights. An Australian overview of work-related FFH revealed similar findings. 12
Overall, fractures of the middle third of the face were most common as well as most frequent in each of the LF, HF and VHF categories. This reflects the nature of the crumple zone of the middle third of the facial skeleton made up of relatively thin bone, essentially designed to withstand and absorb occlusal forces resulting from masticatory loading and afford protection to visceral structures contained therein. Fractures of the orbit were most common overall and likely reflect the multiple bones that articulate to form the walls of the orbit as well as being made up of relatively thin bone to avoid penetrating injuries to the eye. We expected that the incidence of fractures would have increased as fall height increased; however, this was only true of nasal and mandible fractures. The incidence of bilateral fractures and fractures involving more than one facial third, did however, increase as the fall height increased. Interestingly, the incidence of orbital and maxillary fractures decreased as the fall height increased. One theory for this could be that the body has a chance to completely rotate around its centre of gravity the higher the fall and therefore the face is usually not the first point of contact in VHF greater than 10 m. This is supported by other studies which show that the frequency of head injuries is highest in FFH below 7 m 18 In our study, cranial injuries were most common in HF and decreased in VHF. As expected, orthopaedic injuries were commonly associated with a FFH given the dynamics of falling/breaking a fall and increased in incidence as fall height increased. However, the number of associated orthopaedic injuries did fall short of the number of associated cranial injuries and we suspect that this is due to the inclusion of concussion as a cranial injury in our study. High rates of associated injuries highlight the importance of thorough primary, secondary and tertiary surveys as FFH present to emergency departments and oral and maxillofacial surgery units. Moreover, the trend towards a higher number of ICU admissions and operative fixation with increasing fall height is an important consideration for oral and maxillofacial surgeons when assessing and managing patients who have sustained a FFH.
Comparing the sexes, the average age of women was slightly higher and the majority of women fell from lower heights. A higher proportion of women sustained fractures of the lower third of the face as well as an associated injury. Interestingly, women had a slightly longer hospital stay with a higher proportion requiring ICU admission; however, all fatalities recorded were men. Given that there were more than twice as many men as women in our study, it was difficult to draw any conclusions regarding the difference in severity of injury between the sexes. This could form the basis of further studies.
The results of our study were similar to other institutional data in that more men were involved in FFH, there was a bimodal age distribution, midface fractures were the most common and multiple fractures occurred in almost half of patients who fell from height.3-6,10 Despite the large number of overall trauma presentations, the sample size of our study was relatively modest, particularly in the very high fall group, thereby limiting the power to detect statistically significant trends in this group. Other limitations include the use of a pre-existing database and that radiographs were not reviewed to check for accuracy of radiological reporting. Moreover, soft tissue injuries were not documented accurately enough to be included, which would have aided in the calculation of a facial injury severity score. 19
To conclude we wish to highlight the public health concern of FFH; the morbidity and mortality associated with them; as well as raise awareness of injuries which do not usually receive widespread attention. We believe our data is transferrable to other developed countries and encourage further similar, targeted studies. As FFH present to oral and maxillofacial surgical units, we would like to stress the importance of thorough assessment and consideration for ICU admission as well as operative fixation. Also, due to the complex nature of such presentations and associated injuries, we highlight the importance of developing a close working relationship with neurosurgical, orthopaedic and other surgical specialities and colleagues.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.