
Abstract
Importance
Metacognitive Reflection and Insight Therapy for Occupational Therapy (MERIT-OT) is a novel adaptation of an evidence-based psychotherapy model designed to enhance metacognitive capacity and support recovery. Its philosophical alignment with occupational therapy—particularly the emphasis on meaning-making and life participation—makes it a promising intervention for Veterans with serious mental illness. However, to date no implementation studies of MERIT-OT have been conducted.
Objective
To evaluate the implementation of MERIT-OT within a Veterans Affairs (VA) occupational therapy setting and to explore preliminary findings regarding clinical effectiveness.
Design
Pilot study evaluating the implementation and preliminary effectiveness of MERIT-OT when delivered by occupational therapists in a VA setting.
Setting
One VA Medical Center across four occupational therapy practice areas: psychosocial rehabilitation, outpatient mental health, home health, and women's health.
Participants
Five occupational therapists; three implemented MERIT-OT with nine Veterans over 37 sessions.
Outcomes and Measures
Implementation outcomes were assessed using the Consolidated Framework for Implementation Research when analyzing interviews and chart review data. Clinical outcomes were measured using the Metacognition Assessment Scale–Abbreviated (MAS-A).
Results
Facilitators included perceived relative advantage and tension for change. Barriers included competing priorities and documentation challenges. Quantitative analysis showed early gains in metacognitive mastery; other subscales showed limited change.
Conclusions and Relevance
Preliminary findings suggest ongoing consultation, additional training, and improved tools and resources may facilitate MERIT-OT implementation in VA outpatient mental health.
What This Article Adds
MERIT-OT offers a structured, recovery-oriented approach aligned with occupational therapy values and shows promise for enhancing metacognitive outcomes in mental health settings.
Plain Language Summary
This project looked at a new approach called MERIT-OT, which stands for Metacognitive Reflection and Insight Therapy for Occupational Therapy. It's a way for occupational therapists to help people—especially Veterans—better understand themselves and others and use that insight to improve their daily lives. MERIT-OT was originally developed for people with serious mental health conditions and has been used by psychologists. This study explored how occupational therapists in Veterans Affairs (VA) Medical Centers could use it in their own work. Five therapists at one VA Medical Center took part, and three of them used MERIT-OT with nine Veterans over several sessions. The researchers wanted to know two things: (1) how easy it was for therapists to use MERIT-OT in their regular work and (2) whether it helped Veterans improve their thinking in ways that made their lives better. They found that therapists who felt MERIT-OT was useful and needed were more likely to use it. However, some therapists didn’t use it because time constraints made it hard for them to review MERIT-OT trainings enough to feel comfortable with it. Some therapists also said they might have used it more with better documentation processes in place and better understanding of MERIT-OT as a whole among their co-workers. Veterans who received MERIT-OT showed early improvements in one key area: using insight to solve everyday problems. Other areas of thinking didn’t show consistent changes, possibly because more time was needed. Overall, MERIT-OT seems to fit well with occupational therapy and shows promise for helping Veterans in mental health care. The study suggests that with better support and integration into daily practice, MERIT-OT could become a valuable tool for therapists working in the VA system.
Introduction
Metacognitive Reflection and Insight Therapy (MERIT; Lysaker et al., 2019) is an evidence-based approach originally developed to support recovery among people with schizophrenia. MERIT aims to support recovery by enhancing individuals’ ability to manage their lives, make sense of personal challenges, and decide how to respond to those challenges, thereby promoting greater self-direction in recovery and improved quality of life over time. Since its inception, MERIT has been shown to improve these recovery outcomes for people with a wide range of diagnoses including substance use disorders, mood disorders, and post-traumatic stress disorder (Faith et al., 2024).
MERIT integrates eight therapeutic elements designed to stimulate metacognition—defined as the ability to understand oneself and others in diverse social contexts. Metacognition is measured using the Metacognition Assessment Scale–Abbreviated (MAS-A; Semerari et al., 2003), which evaluates self-reflection, understanding others’ thoughts, decentration (recognizing one is not the center of everything) and metacognitive mastery (applying metacognitive knowledge to everyday challenges). Higher scores reflect greater metacognitive capacity. Increased metacognition is linked to collaborative goal setting, motivation, mood, attention, goal attainment, and personal meaning (Faith et al., 2024). MERIT has traditionally been used by psychologists and psychiatrists, but its theoretical foundations align with occupational therapy's emphasis on meaning-making and life participation. MERIT-OT adapts MERIT's eight elements for occupational therapy (Wasmuth et al., 2023).
Veterans receiving mental health services often face complex challenges, including cognitive impairments, difficulties with self-awareness, and disruptions in social functioning that hinder participation in meaningful life roles (Rattray et al., 2021). MERIT-OT directly addresses these challenges by fostering metacognitive capacity—the ability to reflect on one's own thoughts and understand others’ perspectives—within the context of occupational engagement (Wasmuth et al., 2023). By integrating metacognitive strategies into everyday activities, MERIT-OT can help Veterans develop insight, improve problem-solving, and enhance mastery of real-world tasks, which are critical for recovery and reintegration. This approach aligns with the Veterans Health Administration's emphasis on recovery-oriented care and supports functional outcomes such as independence, social connection, and quality of life, making MERIT-OT a promising intervention for this population.
While MERIT's effectiveness has been documented (de Jong et al., 2019), MERIT-OT implementation has not yet been evaluated. To address this, we conducted an implementation study assessing MERIT-OT's implementation and impact in VA OT settings. The primary objective was to identify barriers and facilitators to implementation, using the strategies of educational meetings, ongoing consultation, and external facilitation. A secondary objective was to explore metacognitive and occupational outcomes among Veterans receiving MERIT-OT.
The Consolidated Framework for Implementation Research (CFIR; Reardon et al., 2025) provided a structured, theory-informed approach to assess implementation. CFIR's five domains—intervention characteristics, outer setting, inner setting, individual characteristics, and process—help identify barriers and facilitators across contexts. CFIR is well-suited for implementation studies and supports implementation strategy refinement. Its comprehensive scope makes it ideal for examining the contextual dynamics and stakeholder behaviors that influence MERIT-OT's real-world implementation.
Methods
Design
This pilot study focused primarily on evaluating implementation, with secondary focus on the preliminary effectiveness of the intervention. This design allowed us to evaluate implementation success and explore whether MERIT-OT could replicate recovery outcomes seen when MERIT was delivered by psychologists. Intervention reporting followed the Template for Intervention Description and Replication (TIDieR) checklist, which provides structured guidance for intervention reporting to support transparency and replication.
Participants
Participants included occupational therapy (OT) clinical staff, managers, and OT students/residents within one VA Medical Center, dispersed across multiple OT implementation settings. To recruit participants, the lead author contacted the operational leader of VA OT services, who recommended three VA Medical Centers with strong mental health representation. Of these, one agreed to participate in the study. The other two declined due to competing demands, policy changes, administrative shifts, and uncertainty about staff capacity to implement MERIT-OT. The manager of the participating site contacted OT staff working in settings such as Women's Health, Home Health, and the Psychosocial Rehabilitation and Recovery Center (PRRC) to assess interest. Based on positive feedback, the Center agreed to participate.
This project was deemed “not human subjects research” by the Institutional Review Board and was designated as a quality improvement initiative to inform and enhance implementation of MERIT-OT. All necessary documentation and approvals were obtained by site and institutional personnel.
Intervention
MERIT-OT entails delivering eight therapeutic elements: illuminating the agenda, inserting the therapists’ mind, eliciting a narrative episode, defining the psychological problem, discussing the therapeutic relationship, discussing progress, stimulating reflection of self, and others at the metacognitive level of the patient, and stimulating mastery at the metacognitive level of the patient (Wasmuth et al., 2023). In addition to implementing these elements in OT sessions with Veterans, participating OTs were also asked to assess and document patient metacognition during each OT encounter using the MAS-A (Semerari et al., 2003). As described in the introduction, the MAS-A measures four subdomains of metacognition with four respective rating scales on which higher scores indicated greater metacognitive capacity (self-reflection [0–9], understanding others’ thoughts [0–7], decentration [0–3], and mastery [0–9]).
Implementation Strategy
We utilized the implementation strategy of external facilitation (Penney et al., 2021). An initial virtual kickoff meeting (Baird et al., 2025) led by the external facilitator included provision of a link to the MERIT-OT recorded training, an overview of MERIT-OT, and a documentation template for tracking Veteran metacognition during OT appointments. Prior to kickoff, the external facilitator (first author) provided a 4 hr live, virtual educational training describing MERIT-OT elements, their application, the founding philosophy of MERIT, and the MAS-A rating tool. The training offered opportunities to practice MAS-A ratings and observe and identify the implementation of MERIT elements. If participants had not attended this training, it was provided at the kickoff as a recorded training they could watch prior to implementation. Following the training and kickoff, OTs were asked to begin using the MAS-A rating documentation templates and participate in monthly virtual consultation with the external facilitator to support MERIT-OT implementation. Ongoing consultation offered implementing OTs and opportunity to discuss their use of MERIT-OT, answer questions, and review MAS-A ratings to support confidence and clarity during implementation. This consultation was scheduled as a recurring Microsoft Teams call at a time set by the manager overseeing each OT participant, who delivered services in various virtual and in-person clinical settings under one VA Medical Center. Participants were also asked to complete interviews 6 and 12 months after kickoff. Training materials and recordings can be accessed by contacting the first author.
Implementation Analytic Framework
The CFIR (Damschroder et al., 2022) guided data collection and analysis to evaluate MERIT-OT implementation. To collect data on drivers of MERIT-OT implementation success, we selected interview questions in the CFIR domains of “Innovation” and “Inner Setting.” We prioritized the Innovation and Inner Setting domains because they directly aligned with the goals of our implementation evaluation for MERIT-OT.
Within the Innovation domain, questions addressed innovation design—how well MERIT-OT was assembled, bundled, and presented—and relative advantage—whether it was perceived as better than current practice or alternatives (Reardon et al., 2025). Interview questions on innovation design included: What supports, such as online resources, templates, materials, or a toolkit, were available to help you implement and use the intervention? What is your perception of the quality of the supporting materials, packaging, and bundling of the intervention for implementation? How did available materials affect implementation in your setting? Interview questions on relative advantage included: How does the intervention compare to other similar existing programs in your setting or to other alternatives that may have been considered? Is there another intervention that people would rather implement? Assessing innovation design was critical because it aligned with our implementation strategy bundle, which included virtual and live trainings, supporting materials, documents, and documentation templates. Responses regarding this domain could directly inform necessary adaptations to the intervention for future implementation. Evaluating relative advantage was equally important to determine whether MERIT-OT offered a preferred alternative to current care, which was the primary purpose of its development.
The Inner Setting domain focused on the culture of the implementation site, including constructs such as tension for change (whether the current situation was intolerable and needed to change) and relative priority (the importance of implementing MERIT-OT compared to other initiatives). Questions regarding tension for change included: Is there a strong need for this intervention? How essential is this intervention to meet the needs of the individuals served by your organization or other organizational goals and objectives? How do people feel about current programs/practices/process that are available related to the intervention? Questions focused on culture and relative priority included: How would you describe the culture of your organization? Of your own setting or unit? How do you think your organization's culture (general beliefs, values, assumptions that people embrace) will affect the implementation of the intervention? To what extent are new ideas embraced and used to make improvements in your organization Describe activities or initiatives that (appear to) have highest priority for you (for the organization). These factors were essential for understanding organizational readiness and competing priorities that could influence adoption.
While additional CFIR domains—Outer Setting, Characteristics of Individuals, and Process—could provide further insights important to MERIT-OT implementation, they were not the primary focus of this study. We first sought to understand the inner setting and characteristics of the intervention because they could directly inform factors that we could adjust such as local adaptations to improve fit. Outer Setting factors such as external policies were outside the scope of this study. An important next step will be to explore how characteristics of individuals and the MERIT-OT process influence MERIT-OT implementation.
In addition to structured questions from these domains, the interviewers asked about other barriers and facilitators to MERIT-OT implementation.
CFIR offers a deductive code book for analyzing qualitative interview data, and a rating scale to quantify findings (Damschroder et al., 2022), allowing the team to categorize interview data into the constructs and domains mentioned above as well as other CFIR constructs and domains that emerged during interviews.
Assessing Metacognition
Metacognition was assessed using the MAS-A (Semerari et al., 2003), a clinician-rated measure designed to evaluate the capacity to think about and integrate information regarding one's own and others’ mental states (Lysaker et al., 2014). The MAS-A is applied to narrative material obtained during therapy sessions via applying the eight elements of MERIT-OT. It yields ratings across four hierarchical domains of metacognitive functioning: Self-Reflectivity, Understanding of Others’ Minds, Decentration, and Mastery. Self-Reflectivity is scored from 0 to 9 and assesses the ability to identify, differentiate, and integrate one's own mental states. Understanding of Others’ Minds is scored from 0 to 7 and evaluates the capacity to form complex representations of others’ thoughts, emotions, and intentions. Decentration is scored from 0 to 3 and reflects the ability to understand the self as part of a broader social world rather than the sole center of experience. Mastery is scored from 0 to 9 and assesses the capacity to use metacognitive knowledge to respond to psychological challenges in adaptive ways. Subscale scores are determined by the highest level of metacognitive functioning demonstrated within each domain, and scores are summed to yield a total MAS-A score, with higher scores indicating greater metacognitive integration. The MAS-A has demonstrated good interrater reliability and construct validity across multiple clinical populations and has been widely used in studies of psychopathology and psychotherapy outcomes (Lysaker et al., 2014).
Data Collection
Participants were contacted 6 and 12 months postkickoff and invited to participate in a 30 to 60 min semistructured interview guided by questions derived from the updated CFIR interview guide discussed above (CFIR; Damschroder et al., 2022). Virtual interviews were conducted by the first author via Microsoft Teams.
Chart reviews were conducted on Veterans who received MERIT-OT to extract age, diagnosis, race, gender, ethnicity, dose/duration of OT, MAS-A scores, and any other functional outcome measures documented by the OT during the 10-month MERIT-OT implementation period. Data items pertaining to demographics (i.e., age, diagnosis, race, gender, and ethnicity) were retrieved via a standardized extraction process using the VA Corporate Data Warehouse (Price et al., 2015), while items pertaining to OT service delivery (i.e., dose/duration, MAS-A scores, and functional outcome measures) were entered into a free-response spreadsheet by a member of research team who hand-searched Veteran records.
Data Analysis
Six- and 12-month interview data were transcribed, de-identified, and deductively analyzed by the authors using the updated CFIR codebook (Damschroder et al., 2022). During deductive coding the authors remained open to any emerging themes in the data, making note of salient information falling outside deductive codes.
Qualitative data for each CFIR construct were compiled in Microsoft Excel, with participants listed in rows and CFIR constructs with corresponding qualitative data listed in columns. The authors reviewed the data for each CFIR construct, blinded to the OTs implementation success rating, and independently assigned a quantitative rating from −2 to +2 per construct for each OT. This rating was based on the degree to which the data indicated a positive, negative, or neutral impact on implementation success (Damschroder et al., 2022). For example, if the participant described a high regard for MERIT-OT and favored using it over other available interventions, they received a rating of +2 for relative advantage, which is a perceived advantage of the intervention compared to other similar, available options (Damschroder et al., 2022). If the participant expressed positive regard for MERIT-OT and used it to a similar degree as other interventions, they received a rating of +1. If their perception of MERIT-OT was neutral and/or did not influence their willingness or ability to implement it, they received a 0. If they perceived MERIT-OT as less advantageous than other available interventions they received a −1, and if they perceived it as problematic/undesirable they received a −2. This rating process was completed for each CFIR construct independently by the first two authors, after which they engaged in a blind vote to determine a consensus rating. The authors discussed any voting discrepancies, returning to the data in question, and continued blind voting until consensus was reached for each construct for each participant.
Implementation was conceptualized as frequent, occasional, or absent by reviewing charts to determine whether and how often each OT participant implemented MERIT-OT. OTs used their clinical reasoning to determine when and with whom to use MERIT-OT. Clinicians who used MERIT-OT on a weekly bases were considered frequent implementers. Those who used MERIT-OT a few times but not weekly were considered occasional implementers, and those who did not use MERIT-OT with a Veteran were considered absent implementors. CFIR construct ratings were then examined alongside degree of implementation success to identify potential difference-makers.
Chart reviews were conducted to extract Veteran baseline clinical characteristics (i.e., age, gender, race, diagnosis, and OT assessment scores), MAS-A scores over time, and length of the total intervention period. Within-person trajectories over time were evaluated to examine preliminary signals of effectiveness.
Results
Participant and Site Characteristics
Five OTs from four distinct settings were invited and all agreed to participate; of these five, three implemented MERIT-OT. These three used MERIT-OT with nine Veterans across 37 sessions. Two therapists worked in a VA Psychosocial Rehabilitation and Recovery Center (PRRC), and one in a VA mental health outpatient program. Sessions per Veteran ranged from 1 to 16. Veterans were predominantly male, Black or White, and aged 24 to 77. Diagnoses included bipolar disorder, schizophrenia, and post-traumatic stress disorder.
Clinical characteristics varied by setting. In the PRRC, therapists administered the Patient Health Questionnaire-9 (Kroenke et al., 2001), Internalized Stigma of Mental Illness Scale (Ritsher et al., 2003), Short Warwick-Edinburgh Mental Wellbeing Scale (Tennant et al., 2007), and WHO Disability Schedule 2.0 (Üstün, 2010). The outpatient therapist used the Quality-of-Life Enjoyment and Life Satisfaction Questionnaire-Short Form (Stevanovic, 2011) and single-item questions on life and medication satisfaction. Veteran clinical characteristics varied widely. Supplemental Table 1 provides detailed demographics and clinical data.
Drivers of Implementation Success
Figure 1 illustrates implementation success among the five participating OTs. One OT implemented MERIT-OT frequently, two implemented it occasionally, and two did not implement MERIT-OT. The frequent implementer had positive ratings for all four CFIR constructs. Those who implemented occasionally had one or more neutral or moderate negative ratings combined with at least one strong positive and one moderate positive rating, and no strong negative ratings. The OTs who did not implement had at least one strong negative rating.
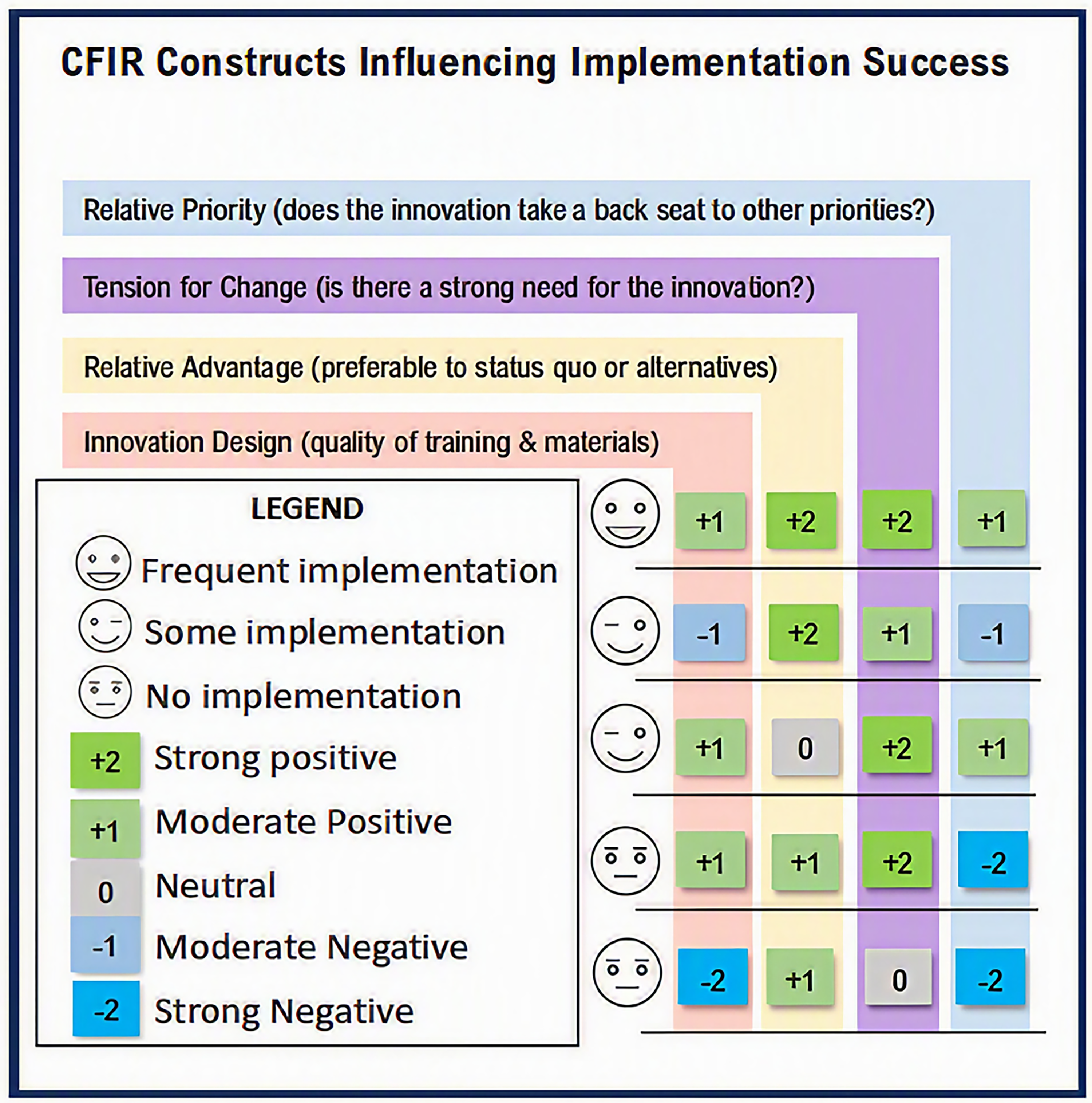
Factors influencing implementation.
No single construct appeared to be a main driver of implementation success. However, as described below and depicted in Figure 1 both “tension for change” and “relative advantage” received overall positive ratings whereas notable limitations were observed in “relative priority” and “innovation design.”
Tension for Change
Most OT participants agreed that there is a strong need for MERIT-OT (tension for change) to adequately capture OT mental health practice and to address the needs of Veterans seeking mental health support. Data from three OTs coded as tension for change were rated as strong positive, expressing statements such as: “It gives us structure and language to something we’re already doing that we don’t always necessarily know how to quantify” (participant 3). Another explained “[MERIT-OT is] very essential…whatever the highest rating is…, yeah, it has been really helpful for both for my understanding of what I'm doing with, especially folks with psychotic disorders, who have a hard time engaging in other approaches or interventions” (participant 5). A third explained seeing a higher percentage of Veterans with mental health diagnoses and cognitive problems related to mental health concerns who struggle with memory, organization, and task management who could greatly benefit from a MERIT-OT approach. Data on tension for change from one OT who thought there was a need to train more OTs in MERIT-OT, especially to address Veterans with psychosis, was rated a moderate positive. Finally, data on tension for change from one OT who noted MERIT-OT as a promising approach, comparable to several other OT interventions, was rated as neutral. No negative ratings were assigned to this construct.
Relative Advantage
Relative advantage—preferring MERIT-OT over current practice or alternative innovations—also did not receive any negative ratings and only one neutral rating, with two strong positive and two moderate positive ratings. OTs described MERIT-OT as particularly advantageous for working with Veterans who don’t fit into clear boxes for therapy episodes of care or who are not responsive to more traditional approaches. Another OT (participant 5) shared a success story: The guy that I have been using it with the longest…he's turning a corner. It's really exciting to see. He's been showing more flexibility and insight…So it's kind of cool to see progress and I've even asked him like, ‘Do you feel like this has been helpful?’ And he's like, ‘Yeah, because you’re like, you’re listening.’
Innovation Design
Innovation design, which refers to the quality of trainings, supporting materials, and resources, received three moderate positive ratings, one moderate negative rating, and one strong negative rating. Demonstrating a strong negative rating, one nonimplementing OT (participant 1) noted limitations of the MERIT-OT documentation templates: I think it [the documentation templates] could be [useful], but…how does that replace what I wrote in my note? Does that meet the requirements of my documentation? That's very different than how my notes look now. I know we had the templates, but…I would have been more successful with it if I'd integrated it into my normal note and just deleted it out when I didn’t need…that probably would have helped me because it would have cued me…it was all about how often I forgot to record that I did it, and for me, out of sight, out of mind.
Relative Priority
The most limiting factor influencing implementation success was relative priority, which examines the extent to which MERIT-OT takes a backseat to other demands/priorities. The two OTs who were unable to implement MERIT-OT were rated as strong negative for this construct. One occasional implementer was rated as moderate negative. The remaining OTs were rated as moderate positive. No strong positive ratings were assigned for relative priority. OTs unable to implement MERIT-OT noted having “way too much on their plates” and not having protected time which they felt was needed to review MERIT-OT training materials and guidelines. Others noted the immediate demands of patients as taking priority over the use of MERIT-OT combined with short duration of visits (30 min) that made it difficult to integrate MERIT elements of practice. Those with positive ratings for relative priority also noted the need to focus on Veteran needs but framed this as a way to prioritize MERIT-OT: “We really just focus on doing the interventions that best suit the Veteran's needs, and so that really is time where I can use a lot of MERIT-OT” (participant 4). These differences illustrate how the varied needs/priorities of Veterans within different mental health settings influence MERIT-OT implementation in the context of relative priority.
Other Barriers and Facilitators to Implementation
In addition to the above data that aligned with CFIR constructs, participants noted some general barriers and facilitators to MERIT-OT implementation. Barriers included desiring (and not having) protected time to review training materials (“I would need probably more administrative time to sit with the materials in the trainings”, participant 2) and feeling the need to fully master material before using it in clinical practice. As one OT noted, “I feel like this is a little more involved and, you know, I want to be very…confident in using it and also confident in explaining it and in figuring out how it all fits in and how it can help” (participant 2).
Facilitators included using memory aids such as posting MERIT-OT's eight elements on computer monitors, having supportive leadership, and the accessibility and style/content of MERIT-OT consultation. Demonstrating the impact of supportive leadership, one OT explained: “I feel very supported by my director and my supervisor. [Site] is very forward thinking in how we utilize our OTs, what that looks like” (participant 3). This flexibility and forward thinking helped the practitioner feel more confident in attempting a new, nontraditional approach to OT. Consultation was critical for all participants, who expressed things like “I don’t think I’d understand what I’m doing without that” and “having someone who knows a lot about it to talk with helped a lot” (participant 5).
Preliminary Effectiveness of MERIT-OT
MAS-A subscale scores over time are displayed in Supplemental Table 2. The first five visits are reported because only one Veteran record contained more than five MAS-A scores. Within-person trajectories across all treatment sessions are displayed in Supplemental Figure 1. When MERIT-OT was documented more than one time, intervention lengths ranged from 5 to 36 weeks, with sessions most often occurring weekly or biweekly. Across the nine Veterans who received MERIT-OT, MAS-A scores varied, with the range of each subscale approaching the extreme ends of each subscale's spectrum. In general, Veterans’ scores fluctuated throughout the duration of treatment, with no visible sustained change over time emerging across sessions. One Veteran demonstrated improvement in all subscales from the initial to the fifth intervention session, and one Veteran did not demonstrate improvements in any of the subscales. Three of the five Veterans demonstrated improvement in the mastery subscale; two of the five Veterans demonstrated improvement in each of the other subscales.
Discussion
This pilot study of MERIT-OT within VA mental health services offers valuable insights into implementation barriers and facilitators. The findings suggest that MERIT-OT's integration into routine practice is shaped by systemic and contextual factors. Using the CFIR, we identified factors that positively influenced implementation, including relative advantage and tension for change, consistent with CFIR's emphasis on the importance of stakeholder buy-in and perceived need for innovation (Damschroder et al., 2022). However, limiting factors including relative priority and design quality—including documentation burden and competing demands—echo challenges noted in other VA implementation efforts (Reardon et al., 2025). Although we created a documentation template to support ease of documenting MAS-A metacognition ratings which some OTs found easy to use, we learned that taking this a step further and integrating it into the existing OT progress note template would further facilitate implementation. Additionally, OTs suggested it would be useful to integrate the therapist adherence scale, which tracks the degree to which the OT completed each of the eight elements of MERIT-OT. This would serve as a reminder to perform each element, thereby supporting implementation.
These findings align with broader implementation science literature, which emphasizes the need for adaptive strategies that integrate new interventions into existing workflows and provide ongoing support (Kirk et al., 2016). Embedding MERIT-OT into electronic health records and aligning it with VA performance metrics may enhance sustainability.
Therapists reported that MERIT-OT provided language and structure to practices they were already intuitively applying, a phenomenon consistent with the concept of practice-based evidence (Greenhalgh et al., 2014). Moreover, the VA's directive on occupational therapy (Directive 1170.06, 2024) reinforces the importance of evidence-based, recovery-oriented care, and supports the expansion of OT roles in mental health settings. MERIT-OT's emphasis on metacognitive development aligns with this directive's goals of promoting functional recovery and self-directed care.
Metacognitive Outcomes
The MAS-A has been validated as a reliable tool for assessing metacognitive capacity in individuals with serious mental illness (Semerari et al., 2003; Lysaker et al., 2018). Descriptive analysis suggested early gains in the Mastery subscale of the MAS-A, indicating that MERIT-OT may help clients begin to apply metacognitive insights to real-world challenges. This finding echoes insights from prior OT literature that suggested, among those with substance use disorders, occupation-based interventions may be particularly effective at improving metacognitive mastery more than the other three subdomains (Wasmuth et al., 2015).
While other subscales did not show obvious change, this may reflect the need for longer intervention duration. Prior studies have shown that metacognitive development is a gradual process requiring sustained therapeutic engagement (Lysaker & Klion, 2017; Musket et al., 2024). Additionally, this exploratory study was not powered to detect meaningful quantitative change but rather suggests possible areas for future investigation of the impacts of MERIT-OT.
Limitations
While this pilot study offers valuable insights into the implementation and preliminary effectiveness of MERIT-OT within VA settings, several limitations should be acknowledged. First, the sample size was small and drawn from five sites under the umbrella of a single VA Medical Center, limiting the insights offered regarding other clinical sites. Future evaluation should include multisite studies with larger, more diverse clinician and patient samples.
Implementation outcomes were prioritized over clinical effectiveness, which naturally limits the depth of analysis regarding client-level therapeutic impact. Although preliminary effectiveness data were collected, these findings should be interpreted as suggested areas for future effectiveness studies.
Finally, the evolving nature of MERIT-OT and its adaptation from psychotherapy to occupational therapy practice presents challenges in standardization. As the model continues to be refined, ongoing feedback from practitioners and clients will be essential to ensure its relevance, feasibility, and therapeutic integrity.
Implications for Occupational Therapy Research and Practice
To enhance MERIT-OT's sustainability, future efforts should focus on:
Workflow integration: Embedding MERIT-OT into standard documentation, treatment planning tools, and alignment with site performance metrics. Training infrastructure: Providing ongoing consultation and fidelity support, as recommended by CFIR implementation guides (Damschroder et al., 2022). Outcome expansion: Evaluating MERIT-OT's impact on broader domains such as occupational engagement, social functioning, and quality of life.
Conclusion
Findings from this pilot implementation and preliminary effectiveness study underscore the importance of integrating MERIT-OT into existing workflows, reducing documentation burden, and providing ongoing consultation to support implementation. Sustained implementation will likely require alignment with VA performance metrics, embedding tools into electronic health records, and continued training infrastructure. Future work should prioritize multisite evaluations, workflow adaptations, and strategies to address competing priorities to ensure MERIT-OT's scalability and sustainability within VA mental health care.
Supplemental Material
sj-docx-1-aot-10.1177_19437676261464048 - Supplemental material for Implementation of Metacognitive Reflection and Insight Therapy for Occupational Therapy (MERIT-OT) to Support Veterans Receiving Occupational Therapy Mental Health Services
Supplemental material, sj-docx-1-aot-10.1177_19437676261464048 for Implementation of Metacognitive Reflection and Insight Therapy for Occupational Therapy (MERIT-OT) to Support Veterans Receiving Occupational Therapy Mental Health Services by Sally Wasmuth, Samantha Randolph, Benjamin Triplett, Anya Kamara, Stephanie M. Rehling, Allison L. Taylor, Caitlin Bunch and Elizabeth Karan in American Journal of Occupational Therapy
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Expanding expertise Through E-health Network Development (EXTEND) Quality Enhancement Research Initiative (grant number QUE HX0003205-01).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.