
Abstract
Importance
Preterm infants frequently experience difficulty with the transition from full tube to independent oral feeding. The influence of extrinsic environmental factors, defined as causes external to the infant, that may affect this transition remains poorly understood.
Objective
To examine the association between extrinsic environmental factors and attainment of independent oral feeding in preterm infants.
Design
A retrospective cohort study was conducted.
Setting
Data were collected from a tertiary care, level II/III neonatal intensive care unit. Guided by the Oral Feeding in Preterm Infants Conceptual Model, extrinsic environmental factors were selected for analysis.
Participants
A total of 282 preterm infants (31.2 ± 2.4 weeks gestation) were included.
Methodology
Factors including maternal medical history, type of medical condition, maternal substance use, non-nutritive sucking, skin-to-skin contact, feeding therapy, and days of hospitalization prior to initiating oral feeding were extracted from electronic medical records. Simple linear regressions identified potential external variables, which were entered into a multiple linear regression model.
Results
In the final multiple linear regression model, maternal medical history, non-nutritive sucking, and skin-to-skin contact were significant predictors of time to independent oral feeding. Maternal age, substance use, feeding therapy, and days in hospital prior to starting oral feeds were not significant.
Conclusion and Relevance
Maternal health and engagement, reflected in maternal medical history, opportunities for non-nutritive sucking, and skin-to-skin contact, are key extrinsic environmental factors influencing the transition to independent oral feeding. Integrating these maternal factors into occupational therapy management may enhance the attainment of independent oral feeding in preterm infants.
Plain Language Summary
Preterm infants frequently experience difficulty with the transition from full tube to independent oral feeding. This retrospective cohort study investigated the influence of extrinsic environmental factors, defined as causes external to the infant, that may impede this transition and found that maternal medical history, non-nutritive sucking, and skin-to-skin contact were significant predictors of time to independent oral feeding in preterm infants. This extrinsic factors can be used in clinical practice to optimize preterm infant oral feeding outcomes.
Keywords
Oral feeding is a critical developmental milestone necessary for adequate growth and development for all infants (Bolea et al., 2025; Robinson et al., 2022). Preterm infants born before 34 weeks’ gestation are typically unable to feed by mouth (orally), and therefore receive their nutrition through a nasogastric or orogastric feeding tube until they are developmentally ready to begin oral feeding (Kowalska et al., 2025). Although some preterm infants can transition from full tube feeding to independent oral feeding relatively easily, up to 40% experience difficulties during this transition (Dodrill et al., 2008; Hawdon et al., 2000; Muir & Fucile, 2022). The process of transitioning from tube to independent oral feeding is complex and influenced by a wide range of intrinsic and extrinsic factors (Bolea et al., 2025; Fucile & Geleynse, 2020). However, there is limited evidence identifying which extrinsic factors influence the transition from full tube to independent oral feeds. This knowledge gap underscores the need for further investigation into the various determinants of attainment to independent oral feeding outcome in preterm infants in the neonatal intensive care unit (NICU).
To gain a deeper understanding of the complexities of the oral feeding process in preterm infants, Fucile and Geleynse (2020) proposed an Oral Feeding in Preterm Infants Conceptual Model. This model was developed to describe how both intrinsic neurophysiological factors and extrinsic environmental influences can affect oral feeding performance in preterm infants in the NICU. This model, adapted from the Canadian Model of Occupational Performance and Engagement and the International Classification of Functioning, Disability, and Health, depicts oral feeding performance as a dynamic interplay between intrinsic neurophysiological factors and extrinsic environmental influences, all of which are closely interrelated (Fucile & Geleynse, 2020). At its core are the essential skills of sucking, swallowing, and breathing, dependent on the proper functioning and coordination of intrinsic neurophysiological systems. Intrinsic neurophysiological factors refer to biological and neurological characteristics inherent to the infant that influence the development and coordination of oral feeding. These intrinsic factors reflect the maturation and integrity of the infant's neurological, sensory, and motor systems that support the complex coordination of sucking, swallowing, and breathing required for safe and efficient oral feeding. Intrinsic factors include the musculoskeletal, gastrointestinal, respiratory, cardiovascular, behavioral, and neurological systems. Immaturity or impairment in any of these systems has been shown to affect the acquisition of independent oral feeding in preterm infants (Crapnell et al., 2013, 2015; Dodrill et al., 2008; Fucile et al., 2020; Jadcherla et al., 2010). According to this model extrinsic environmental factors in the NICU also influence oral feeding performance. Extrinsic environmental factors refer to external causes that influence infant development and feeding but are not inherent to the infant. These factors include physical surroundings, institutional policies, parental attributes, healthcare provider practices, and feeding equipment. According to the Oral Feeding in Preterm Infants Conceptual Model, such environmental influences play an important role in shaping oral feeding outcomes in preterm infants. More specifically, the Oral Feeding in Preterm Infants Conceptual Model describes how aspects of the physical surroundings, such as noise level, bright lighting, and unit design can increase infant stress and disrupt physiological stability, including heart rate, oxygen saturation, and respiratory patterns. These physiological disturbances can interfere with the infant's ability to coordinate sucking, swallowing, and breathing, thereby negatively affecting oral feeding performance (Park et al., 2015). NICU policies and practices, such as family-centered care, demand- versus cue-based feeding approaches, and opportunities for non-nutritive sucking on a pacifier or emptied breast and skin-to-skin contact promote parental engagement and provide infants with frequent, positive interactions. These interactions support the development of oral-motor skills and physiological regulation required for successful oral feeding (Fucile & Dow, 2021; Karimi et al., 2020; Lau et al., 2018; O'Brien et al., 2018; Park et al., 2015; Zhang et al., 2024). Healthcare provider practices, including consistency of care teams and coordinated multidisciplinary approaches, further enhance oral feeding outcomes by ensuring developmentally supportive care (O'Brien et al., 2018). Parental attributes refer to the physical, mental, and emotional characteristics of the parent, including health status, availability, responsiveness, and engagement, which influence the frequency, quality, and effectiveness of caregiving interactions, such as non-nutritive sucking on an emptied breast or skin-to-skin contact, that support the infant's oral feeding outcomes (Muir & Fucile, 2022).
Finally, feeding equipment, including bottle and nipple designs or nipple shields can directly support the infant's ability to coordinate sucking, swallowing, and breathing, optimizing oral feeding performance. Collectively, these extrinsic factors create a supportive environment that facilitates attainment of independent oral feeding.
Evidence on extrinsic environmental factors affecting oral feeding in preterm infants is limited (Bolea et al., 2025; Briere et al., 2015; Fucile & Geleynse, 2020; Park et al., 2015; Pickler et al., 2013). Furthermore, most studies examine extrinsic environmental factors in isolation, and there is limited understanding of the combined influence of external environmental factors on oral feeding outcomes in preterm infants. An integrated evaluation within a conceptual model provides a deeper understanding of extrinsic influences and their clinical relevance. The objective of this study is to examine the relationship between extrinsic environmental factors and attainment of independent oral feeding in preterm infants. We hypothesize that favorable extrinsic environmental influences in the NICU are associated with earlier attainment of independent oral feeding in preterm infants. Favorable extrinsic influences include physical surroundings, institutional policies, parental attributes, healthcare provider practices, and feeding equipment that support infant feeding.
Methods
Design and Setting: A retrospective cohort study was carried out using data from levels II and III NICU at Kingston Health Sciences Centre (KHSC) in Ontario, Canada. The NICU is a tertiary care center and has a maximum capacity of 26 beds. The study received ethical approval from the Queen's University and Affiliated Hospitals Human Research Ethics Board. The unit transitioned from a scheduled feeding approach to a family-integrated, cue-based approach around 2015, when data collection for this study began. In this approach oral feedings are initiated and advanced based on the infant's behavioral and physiological cues, with parents actively involved in the process. A multidisciplinary team, including nurses, occupational therapists, and neonatologists, collaborates with parents to guide the initiation and progression of oral feeding in preterm infants.
Participants: The retrospective study included preterm infants who met the following criteria: born before 34 weeks’ gestation because most infants at this gestational age are not receiving oral feeding; and born without congenital anomalies affecting the oral structures or genetic syndromes because of the high likelihood of encountering oral feeding difficulties.
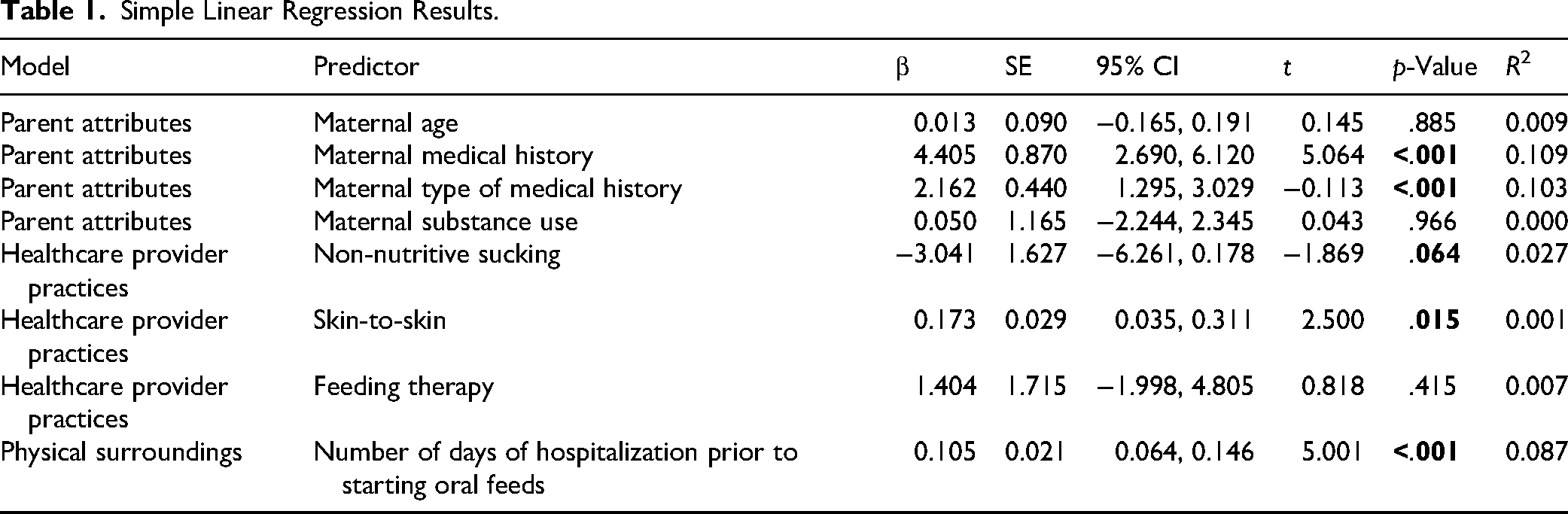
Variables: Extrinsic environmental factors which may influence attainment to independent oral feedings were identified using the Oral Feeding in Preterm Infants Conceptual Model as a guiding framework. In addition, variables were selected based on their availability for abstraction from the medical record, as these data are routinely documented by neonatal staff as part of standard care. Based on this model, study variables included maternal age, maternal history of a medical condition as well as type of condition (physical health or mental health or both), maternal substance use (licit or illicit substances), non-nutritive sucking on an emptied breast, skin-to-skin contact, feeding therapy (occupational therapy, physical therapy, or speech language pathology related to oral feeding assessment and intervention), and number of days in NICU prior to starting oral feeds. Table 1 outlines the corresponding extrinsic system associated with each of these outcome variables. We also collected baseline characteristics of the cohort (Table 2), including infant gestational age, birthweight, sex, 1- and 5min Apgar scores, time to achieve independent oral feedings, length of hospital stay, and maternal age.
Simple Linear Regression Results.
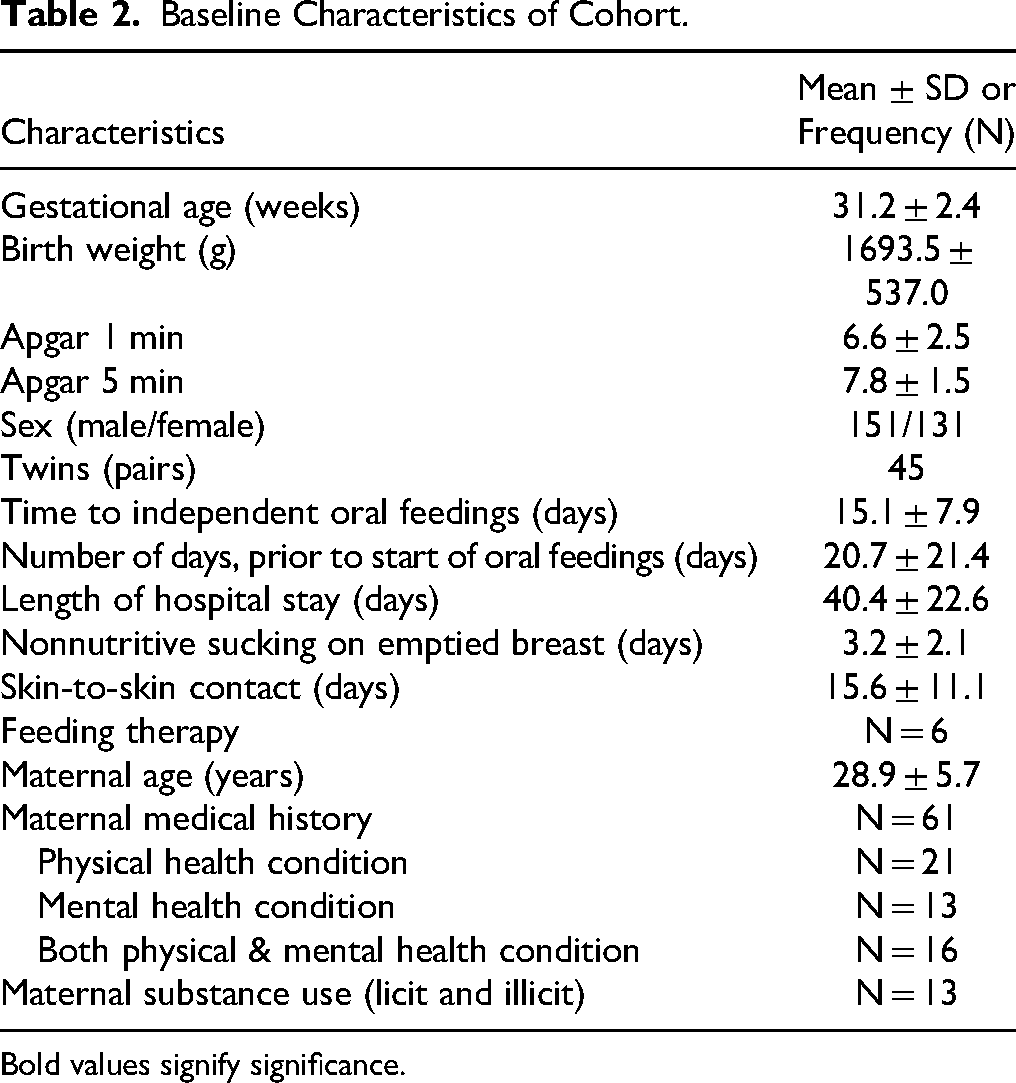
Baseline Characteristics of Cohort.
Bold values signify significance.
The target sample size was determined to ensure adequate power for the planned multiple linear regression analyses. Following the general recommendation of at least 10 to 15 participants per predictor variable and anticipating up to eight possible predictors in the model, approximately 120 participants was required. To account for potential missing data, the sample was increased by approximately 50%, resulting in a final target of 236 infants. This sample size was considered sufficient to detect clinically meaningful associations between intrinsic neurophysiological factors and attainment of independent oral feeding with a significance level of p < .05.
Procedure: All data were obtained through a retrospective chart review of infants admitted from 2015 to 2024. Infants who met the eligibility criteria were included consecutively until the target sample size was reached. Two researcher assistants, with backgrounds in occupational therapy, were trained in data abstraction. Each research assistant was responsible for abstracting data from the electronic medical records from 2015 to 2024. To ensure accuracy, the data collected was cross-referenced with the other researcher. The following procedure was followed to ensure ethical conformity and eligibility: (1) the research assistants first reviewed electronic medical records from the study period to determine eligibility for inclusion in the study. (2) Following this, the research assistants also verified that each participant had provided their consent for the use of their data from their electronic medical chart for research purposes. (3) Data for attainment to independent oral feedings as well as the extrinsic factors outcomes were abstracted from electronic medical records. (4) To ensure accuracy, all data collected was cross-referenced by the other research assistant.
Statistical Analysis
Descriptive statistics were used to summarize baseline sample characteristics (Table 2). To evaluate the influence of each extrinsic environmental factor on attainment to independent oral feedings, a single linear regression was first performed for each variable. A threshold of p < .07 was set a priori and was deemed clinically relevant. Variables meeting this significance threshold were then entered into a multiple linear regression model. Statistical significance was set as p < .05. All data analysis was conducted using the IBM Statistical Product and Service Solution (SPSS) Version 29.0 program.
Results
Baseline: Table 2 illustrates the baseline characteristics of the sample. A total of 282 infants met the eligibility criteria, exceeding the anticipated target. The mean gestational age was 31.2 ± 2.4 weeks, and the mean birth weight was 1693.6 ± 437.0 g. The mean Apgar score at 1 and 5 min was 6.6 ± 2.4 and 7.8 ± 1.6, respectively. The infant's sex was proportionally distributed (151 males, 131 females). There were 45 pairs of twins. The mean time to attainment to independent oral feeds was 15.1 ± 7.9 and mean length of hospitalization was 40.4 ± 22.6. The mean maternal age of the samples was 28.9 ± 5.7 years old.
Simple Linear Regression: Table 1 illustrates the simple linear regression results. The following variables met the set threshold: maternal medical history (β = 4.405, p < .001), maternal type of medical history (β = 2.162, p < .001), non-nutritive sucking (β = −3.041, p = .064), skin-to-skin (β = 0.173, p = .015), and days in the NICU prior to oral feedings (β = 0.105, p < .001). The remaining variables, including maternal age, maternal substance use, feeding therapy were not significantly associated with attainment to independent oral feeds.
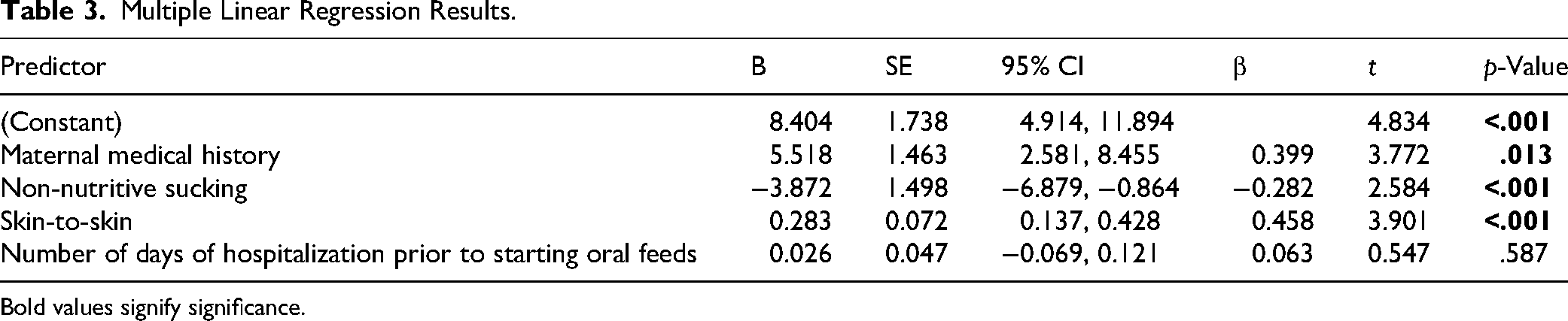
Multiple Linear Regression Model: A multiple linear regression analysis was conducted to identify predictors of time to achieve independent oral feeding. Table 3 demonstrates the multiple linear regression results. The independent variables entered in the model included maternal medical history, non-nutritive sucking, skin-to-skin, numbers of days in hospital prior to oral feedings. Maternal type of medical history was not included in the model a priori due to its strong correlation with maternal medical history. The overall model was statistically significant, F(14.648) =, p < .001, explaining approximately 46% of the variance in days to independent oral feeding (R2 = 0.461, adjusted R2 = 0.419). Among the predictors, maternal medical history, non-nutritive sucking, skin-to-skin contact were significant. Number of days of hospitalization prior to oral feeding started was not significant.
Multiple Linear Regression Results.
Bold values signify significance.
Discussion
This study's objective was to identify extrinsic environmental factors associated with the attainment of independent oral feeding to help guide clinical practice. The findings from the multiple linear regression model reveal that maternal medical history, non-nutritive sucking, and skin-to-skin contact were significant predictors of time to achieve independent oral feeding.
The prominent role that maternal medical history, including maternal physical, mental or both health conditions, associated with attainment to independent oral feeding is consistent with other research (Crapnell et al., 2015; Muir & Fucile, 2022; O'Brien et al., 2015). Mental health disorders, in particular, maternal depressive symptoms can disrupt maternal–infant interaction and maternal responsiveness to infant cues during oral feeding which has been associated with shorter direct breastfeeding duration and longer transition to independent oral feedings (Burnett et al., 2018; Muir & Fucile, 2022). Furthermore, maternal distress has been linked with less developmentally supportive oral feeding interactive behaviors which delay the transition to independent oral feeding (Muir & Fucile, 2022; Zhang et al., 2024). Maternal physical health issues, such as diabetes, has been associated with infant low muscle tone and low energy level affecting their oral feeding abilities (Doughty & Taylor, 2021; Gunderson et al., 2018). Together, these findings suggest that maternal medical history is a significant determinant of infant oral feeding competence.
The findings of this study also reveal that non-nutritive sucking on emptied breast opportunities are associated with transition from full tube to independent oral feedings. These results are consistent with previous systematic reviews (Lu et al., 2025; Zhao et al., 2024). These results highlight the role of non-nutritive sucking as a training strategy to strengthen the oral-motor skills necessary to generate and coordinate suck–swallow–breathe sequence necessary for competent oral feeding (John et al., 2019; Pineda et al., 2019). Structured interventions to promote non-nutritive sucking, such as sucking on an emptied breast has been shown to advance the acquisition of independent oral feeding milestones and reduce NICU length of stay (Fucile & Dow, 2021; John et al., 2019; Lu et al., 2025; Zhao et al., 2024). In our NICU, a pacifier is often provided in a nonstandardized approach. Therefore, there is no protocol to capture pacifier use in the electronic medical record, so its frequency is unknown. In contrast, non-nutritive sucking on an emptied breast is usually offered once daily when infants are tolerating full enteral feeding, and these sessions are consistently documented in the medical record. The predictive strength of non-nutritive sucking on an emptied breast in this study underscores its value as a target for early intervention to enhance the transition from full tube to independent oral feeding. The results of this study indicated that skin to skin contact is also associated with transition from tube to independent oral feedings. This finding is supportive of a systematic review on skin-to-skin contact which shows it enhances direct breast feeding establishment in the NICU and with moderate effect on the transition to independent oral feedings (Casper et al., 2018; Karimi et al., 2020). In our unit, skin-to-skin contact is provided daily when infants are clinically stable. This practice facilitates earlier independent oral feeding by supporting sensory and neuromotor development, which is critical for the coordination of suck–swallow–breathe patterns. Skin-to-skin contact also strengthens maternal–infant bonding, increases maternal sensitivity to feeding cues, and promotes more frequent feeding practice at the breast (Casper et al., 2018; Karimi et al., 2020). Together, these factors contribute to improved oral feeding performance and a faster transition from tube to independent oral feeding. One predictor that was not significantly associated with the attainment of independent oral feeding in this cohort was the number of days infants spent in the hospital before beginning oral feeding. Although it is often assumed that a longer exposure to the NICU environment may delay feeding readiness, an expectation reflected in the Oral Feeding in Preterm Infants Conceptual Model and supported by previous research (Park et al., 2015), our findings did not demonstrate this relationship. A likely explanation is that days in hospital prior to initiating oral feeding is context-dependent rather than a marker for oral feeding ability. Specifically, the timing of oral feeding initiation is strongly influenced by clinical decision making, infant medical stability, and unit practices, all of which can vary widely. As a result, this measure may capture institutional or oral feeding management differences rather than true infant feeding capacity. Consequently, it does not reliably predict the infant's attainment of independent oral feeding.
Our approach and interpretation were guided by the Oral Feeding in Preterm Infants Conceptual Model (Fucile & Geleynse, 2020). This framework emphasizes that the extrinsic environmental factors collectively influence oral feeding outcomes (Fucile & Geleynse, 2020). Consistent with this model, our findings indicate that maternal medical history and early engagement experiences, specifically maternal medical history, non-nutritive sucking and skin-to-skin contact exert a predominant influence on oral feeding progression, even when other external factors are considered. Notably, maternal health (medical history) was identified as a significant external influence. This finding suggests that a mother's overall health, including the absence of physical or mental health conditions, may affect her ability to consistently participate in her infant's care and, in turn, influence the infant's oral feeding trajectory. Maternal depressive symptoms or high levels of stress can reduce emotional availability and responsiveness, limiting opportunities for positive parent–infant interactions and engagement in feeding-related practices. Specifically, when mothers are healthy, emotionally available, and able to engage in practices such as skin-to-skin contact or offering non-nutritive sucking, infants experience more frequent and supportive interactions that facilitate the oral-motor learning required for independent oral feeding (Cheng et al., 2021; O'Brien et al., 2018). These observations highlight the critical interplay between maternal health and maternal engagement factors in the acquisition of independent oral feeding.
Although the multiple linear regression model was statistically significant, explaining 46% of the variance in time to independent oral feeding, these results indicate that additional influences also contribute to feeding outcomes. Intrinsic neurophysiological factors, including maturation and coordination of the musculoskeletal, gastrointestinal, respiratory, cardiovascular, behavioral, and neurological systems play a critical role in the development of safe and efficient suck–swallow–breathe patterns. This finding underscores the complex interplay between intrinsic mechanisms and extrinsic environmental influences on oral feeding outcomes in preterm infants, as described in the Oral Feeding in Preterm Infants Conceptual Model (Fucile & Geleynse, 2020).
These findings have clinical implications for occupational therapy practice. Clinically, at a time when cue-based feeding is becoming predominant in many NICUS across North America, this study reveals that maternal health and engagement, in particular skin-to-skin contact and non-nutritive sucking on emptied breast, are important considerations when managing oral feeding in preterm infants. However, the findings must be interpreted within the broader context of the infant's neurodevelopmental maturity and ability to generate and coordinated suck–swallow–breathe coordinated needed for safe and competent oral feeding (Golmohammadi et al., 2025; Munoz-Gomez et al., 2024; Rhooms et al., 2019; Sheikh-Mohamed et al., 2024). Overall, a comprehensive assessment and intervention plan that incorporates infants’ maturity as well maternal health and engagement can optimize oral feeding outcomes in preterm infants.
This study has several limitations. The retrospective study design made it difficult to cross-reference any errors within the documentation. However, the data were abstracted by one research assistant and independently verified by a second research assistant to ensure the accuracy of the extracted data. Furthermore, the retrospective study design entailed relying only on data included in the infants’ electronic medical charts, and thus some factors were not considered, such as non-nutritive sucking on a pacifier because the data were not available. The single-center design may limit the generalizability of the findings. Future prospective study designs are needed to confirm these results, and to further understand the underlying mechanism of how extrinsic factors influence attainment of independent oral feeding in preterm infants.
Conclusion
This study found that maternal health and engagement, including non-nutritive sucking on an emptied breast and skin-to-skin contact, are key external factors supporting the progression to independent oral feeding. Consideration of these external factors within a developmentally informed care framework may optimize oral feeding outcomes and facilitate smoother transition from full tube to independent oral feeding in preterm infants.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.