
Abstract
Importance
Driving facilitates independence and community engagement, especially in Saudi Arabia, where most people rely on cars. Medical conditions can impair driving ability, and occupational therapists play a key role in evaluation and rehabilitation. However, guidance and services to support safe return to driving in Saudi Arabia remain limited.
Objective
To explore current practices and challenges in driver assessment and rehabilitation as perceived by occupational therapists in Saudi Arabia.
Design
This descriptive qualitative research involved semi-structured individual interviews with participants. Data were analysed using reflexive thematic analysis, guided by the Behaviour Change Wheel (BCW) framework.
Setting
Interviews were conducted either in-person or virtually at each participant's preferred time and location.
Participants
Thirteen licensed occupational therapists with at least one year of experience in a rehabilitation setting in Saudi Arabia.
Results
Six themes were identified: (1) insufficient knowledge and practical skills, (2) lack of training and supporting infrastructure, (3) motivation [but it is hard], (4) recommended interventions, (5) recommended changes in policies and (6) collaboration.
Conclusions and Relevance
Addressing the identified gaps in knowledge, skills and infrastructure through the suggested interventions and policy changes could enable occupational therapists in Saudi Arabia to contribute effectively to driver assessment and rehabilitation services for at-risk drivers, as well as promote road safety for all within Saudi Arabia. Collaborative efforts of occupational therapists and other stakeholders are essential to further leverage study findings in co-creating solutions to address safe return to driving and improving road safety in general.
Plain Language Summary
Driving enables people to access desired occupations and community involvement, especially in countries like Saudi Arabia, where many rely heavily on cars for transportation. Guidelines and services in Saudi Arabia to determine if people with medical conditions can safely return to driving are limited. This study explored occupational therapists’ perspectives on driver assessments and rehabilitation in Saudi Arabia, highlighting significant gaps in knowledge, skills and infrastructure. The occupational therapists recommended providing specialised training for driver assessment and rehabilitation, clear guidelines and improved policy support. Implementing these recommendations requires the collaborative efforts of occupational therapists and other stakeholders to better assist individuals in safely returning to driving, and ultimately to enhance road safety and community participation for all in Saudi Arabia and in other countries with similar contexts.
Introduction
Driving enables people to access their desired occupations, such as social activities, shopping and work or study (Spinney et al., 2020). According to Mouratidis (2025), car drivers have better health, lower anxiety and an overall increase in life satisfaction compared with non-drivers. Furthermore, driving is considered a crucial activity for many people because it allows them to meet many life expectations (Raber et al., 2012). This is especially true in car-centric societies such as Saudi Arabia, where the current infrastructure relies heavily on driving and offers limited alternative transportation options (Shaik et al., 2025).
Driving is a complex activity that demands multiple physical capabilities like strength, endurance, balance and fine motor coordination. It also demands visual abilities, including visual acuity, peripheral vision, contrast sensitivity, tracking and cognitive skills such as memory and decision-making (AOTA, 2020; Driver and Vehicle Licensing Agency, 2018; Pellerito & Burt, 2006). Therefore, individuals diagnosed with medical conditions or disabilities that may affect their driving ability should undergo specialised evaluations.
It is reasonable to claim that there is international agreement on the importance of determining fitness to drive among medically at-risk drivers. In Australia, the United Kingdom, Canada and the United States, published medical guidelines regarding driving assessments are available to inform health professionals and regulate medical practice (American Geriatrics Society, 2016; Austroads & National Transport Commission, 2022; Canadian Council of Motor Transport Administration, 2017; Di Stefano & Ross, 2018; Driver and Vehicle Licensing Agency, 2018 The Association for Driver Rehabilitation Specialists, 2016). Driving assessment and rehabilitation is considered a specialised practice area requiring specific knowledge (The Association for Driver Rehabilitation Specialists, 2016). In Australia, Canada and the United States, most occupational therapists working in driver assessment and rehabilitation have undertaken specialised education and training in addition to their qualifications as occupational therapists.
In comparison, in Saudi Arabia, the field of driver assessment and rehabilitation is undeveloped, as there is no published information or evidence regarding the involvement of occupational therapists in this practice area, nor are there any existing guidelines or formal processes for driver assessment. Therefore, this study was aimed to explore the current practice of occupational therapists in addressing safe return to driving and provide suitable recommendations for the Saudi Arabian context to enhance future occupational therapy practice in this unique area.
Method
Study Design
A qualitative descriptive approach was employed to explore current practices and challenges in driver assessment and rehabilitation as perceived by occupational therapists in Saudi Arabia. The Behaviour Change Wheel Framework (BCW) was used to propose actionable improvements (Michie et al., 2011). The BCW framework provides a structured approach to identifying factors that influence successful behaviour change interventions. As shown in Figure 1, its core emphasises the importance of understanding three key conditions: capability, opportunity and motivation (also referred to as the COM-B model), as central to addressing any change (Michie et al., 2014). Further, it describes nine intervention functions, for taking action to address these conditions, shown in the middle layer of Figure 1, and seven types of policy measures, shown in the outer layer, that may enable the interventions to be implemented (Michie et al., 2014).
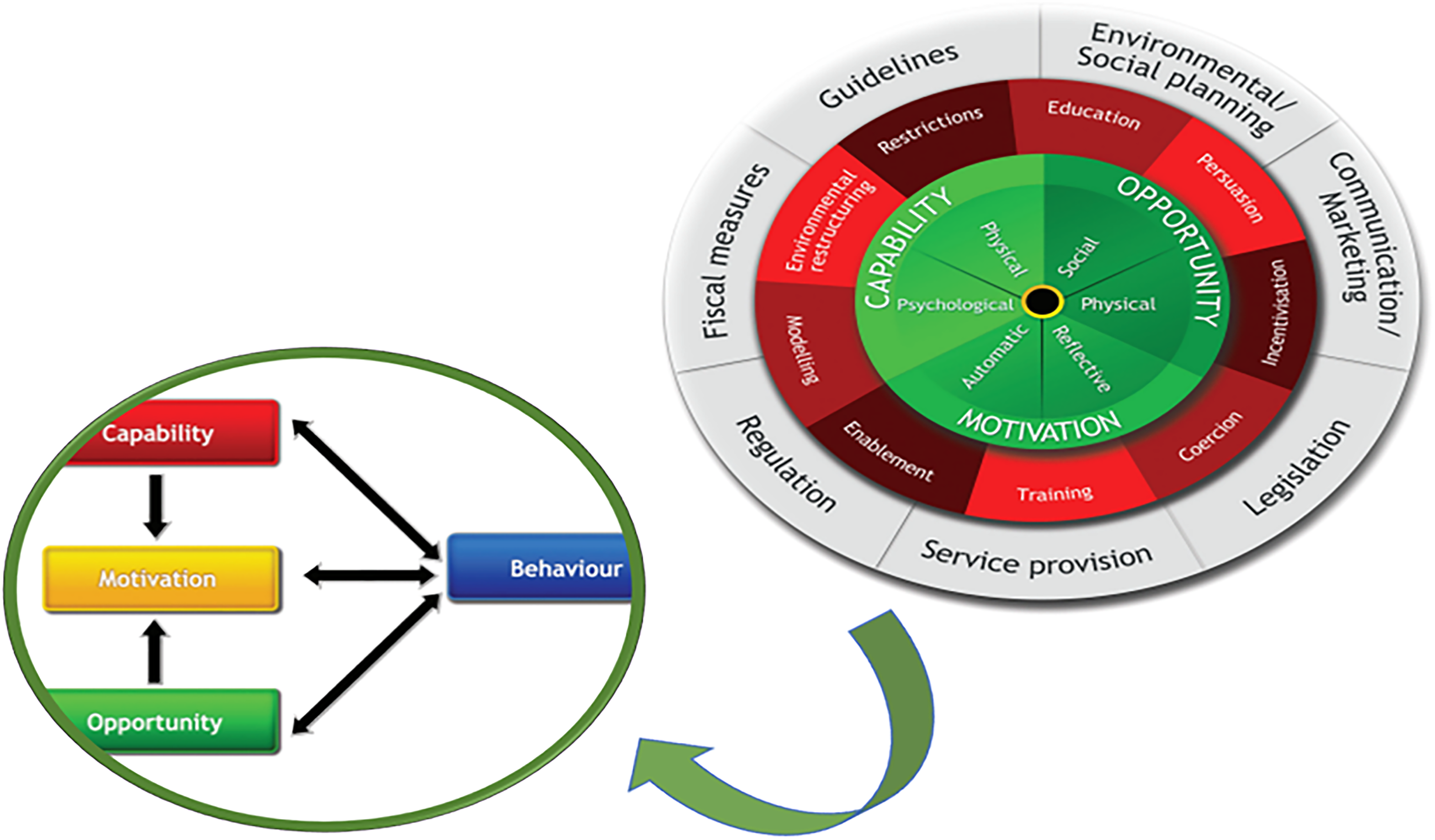
Behaviour change wheel and the COM-B model (the core of the wheel). Reproduced from Michie et al. (2014).
Recruitment and Setting
Licensed occupational therapists in Saudi Arabia with at least 1 year of professional experience were purposefully selected to ensure the collection of in-depth and relevant data (Korstjens & Moser, 2018). Occupational therapists currently working in a rehabilitation facility and those providing care for adult patients in a private or public health care setting were included, given that the field of driving rehabilitation is undeveloped in Saudi Arabia, and these are the practice settings in which occupational therapists encounter patients with return to driving issues. Occupational therapists with less than 1 year of professional experience or working with a paediatric or geriatric population were excluded. An estimated sample size of 10–20 participants was expected to achieve adequate information power (Malterud et al., 2016). This sample size was guided by Hennink and Kaiser's (2022) recommendation that data saturation in qualitative research using in-depth interviews is generally reached with approximately 9–17 participants. From 16 therapists who expressed interest, 13 consented and participated. Written informed consent was obtained from all participants. Recruitment began in July 2022 through social media platforms managed by the Saudi Occupational Therapy Association (SOTA). To expand the sample, snowball sampling was employed from August to November 2022 and concluded in December 2022. Ethical approval was granted by the Monash University Human Research Ethics Committee (Project ID: 31317).
Materials
Informed by literature review findings and the BCW framework (see Figure 1), a semi-structured interview guide was developed for this study (see Appendix 1, Table A1). All questions were posed during the one-on-one semi-structured interviews, and probing methods were employed to elicit detailed responses (McGrath et al., 2018). To aid in the organisation and management of the data, all interview transcripts were uploaded into NVivo version 2020.
Data Collection
Participants took part virtually or in-person, based on their preferences. Interviews were conducted by the first author in English, audio-recorded, and transcribed verbatim. The interviewer, who is from Saudi Arabia and has a background in occupational therapy, engaged in reflexive practice during and post interviews.
Data Analysis
Clarke and Braun's (2021) six-phase methodology for reflexive thematic analysis (TA) guided the analysis. Reflexive TA was used to provide flexibility and acknowledge the researcher's potential biases in data interpretation. In phase 1 (data familiarisation), transcribed data was reviewed to understand the data better, taking notes on potential patterns. An inductive coding approach was utilised to identify meanings in phase 2 (coding). Preliminary codes were created by selecting segments of raw data and labelling them to reflect their meaning. Three authors (DA, AL, EF) met several times to refine codes and to generate and develop themes (as per phases 3 and 4). Theme development was guided by the BCW Framework and the COM-B model (see Figure 1). The capabilities, opportunities, and motivations of occupational therapists to participate in providing driver assessment and rehabilitation services were identified. Then, the participants’ suggestions were mapped to the BCW framework recommendations to inform an improved approach to driver assessment and rehabilitation services, guiding suitable intervention functions and policy practices (Clarke & Braun, 2021). DA, EF and AL further reviewed relevant codes and data to enhance the identified themes. Subsequently, DA refined the themes throughout the writing process in phases 5 and 6 (refining themes and writing up). Finally, all members of the research team collaborated to finalise the presented themes.
Trustworthiness
As outlined by Polit (2018), credibility refers to the truth value of the data and its interpretations. In this study, a prolonged engagement strategy was employed to enhance credibility. The first author's experience working in rehabilitation settings in Saudi Arabia effectively helped build rapport with the participants and elicited their responses efficiently. Furthermore, the interviews lasted at least 60 min and included constant clarification of participants’ statements through summarisation, paraphrasing and follow-up questions to ensure that the collected data was accurately understood.
Two strategies were employed to enhance the dependability of the research: audit trails and reflexive writing. Audit trails were implemented to maximise transparency in the data collection and analysis processes. Each research procedure was clearly detailed and closely followed the six steps of the reflexive thematic analysis approach. Reflexive writing involves critically examining how one's own experiences, emotions and presence influence the research process(Clarke & Braun, 2021). Reflexive writing was used both before and after conducting the interviews, as well as throughout the processes of listening to and transcribing the audio recordings, coding, and writing themes. Together, reflexive writing and the audit trail helped to track the development of concepts and themes effectively.
The specific context of the rehabilitation settings where the therapists worked was not described due to privacy concerns. The interview procedure, questions and analysis process were detailed to provide enough insight for readers to evaluate the potential transferability of the study's findings to other contexts.
Two main strategies were used to enhance the confirmability of the study: peer review and in-vivo coding. Peer review involved regular discussions with two team members regarding the analysis, code interpretation and the emergence of themes. These discussions led to repeated data coding and clustering, as well as the development and refinement of themes. In-vivo coding utilised participants’ actual wording during the coding process. This approach minimises the likelihood that data is misinterpreted by ensuring that it is represented in the participants’ actual words as far as possible (Korstjens & Moser, 2018).
Results
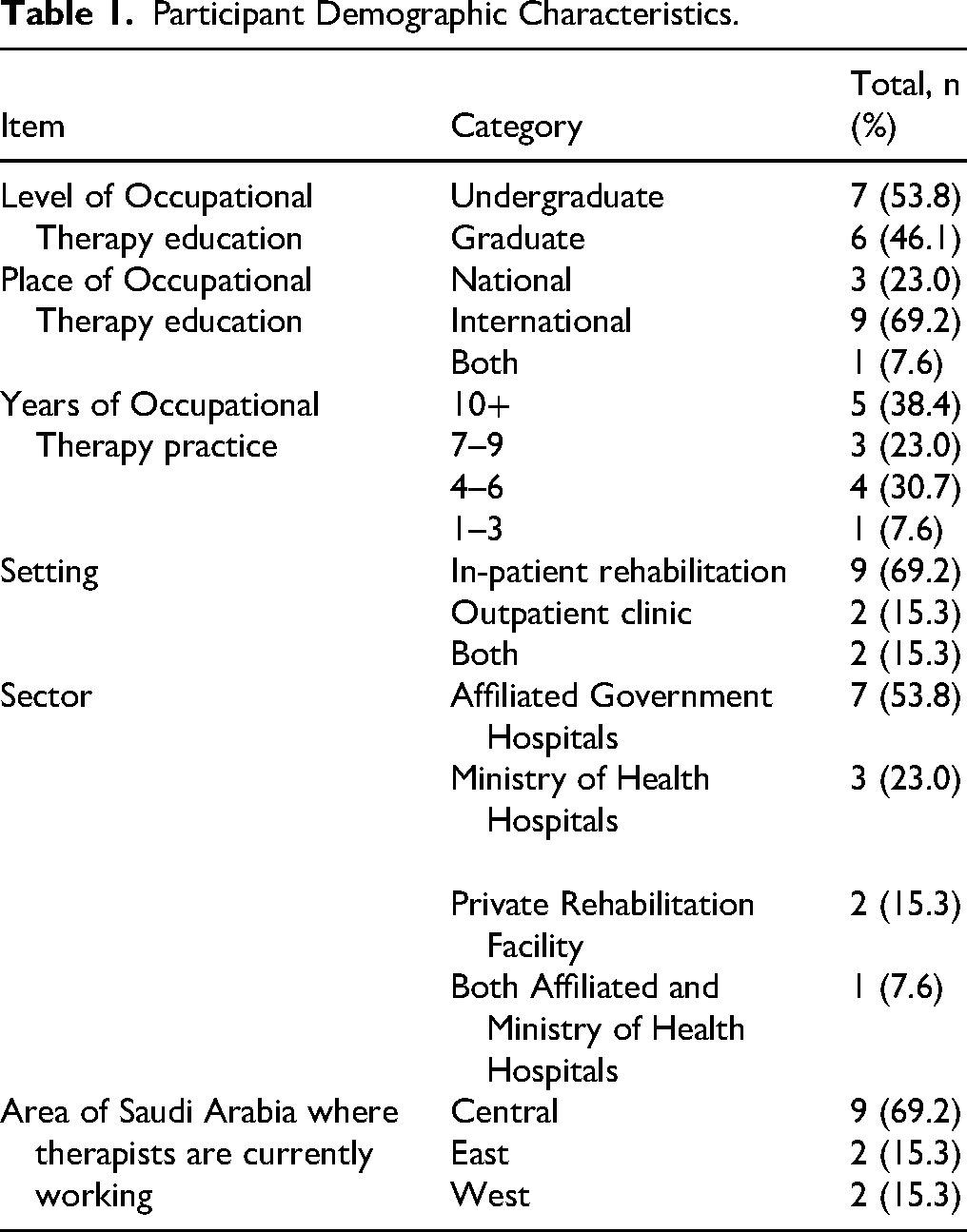
Thirteen occupational therapists participated in the study and key demographic characteristics are presented below (see Table 1).
Participant Demographic Characteristics.
Themes
Themes associated with the components of the COM-B model (the green core of the BCW including capabilities, opportunities, and motivation), were identified. Then, themes associated with the outer layers of the BCW framework, describing interventions in red and policies in grey, recommended by the participants, were identified to bring about potential changes in driver assessment and rehabilitation practice in the context of Saudi Arabia.
Additionally, collaboration, the sixth and final theme, described the range of stakeholders with whom the participants suggested collaborating with to effectively change practices and services for at-risk drivers to receive assessment and rehabilitation.
Figure 2 summarises the BCW's application to the study findings. Following this, detailed presentations of the findings are provided within each key theme/sub-theme.
1. Insufficient knowledge and practical skills (capabilities) This theme examines the self-reported capabilities of occupational therapists in conducting driver assessments and providing best-practice rehabilitation for patients with medical conditions that impact their driving abilities. The findings highlight a notable perceived gap in their knowledge and practical skills within this practice area. Therapists described their current practice, explaining that their primary focus is usually on attempting to address safe transfers into cars only. As one therapist summarised, ‘We are mostly … transferring the patient to a car’ (P1). Therapists further expressed a lack of confidence in assessing a person's ability to drive safely or to make an informed decision about driving, with one therapist sharing, ‘I’ll be totally transparent with you. If I received a referral officially asking me to assist the patient's ability to drive or do like a driver and assessment, I would not be able to do that’ (P9). This was generally either because they were unaware of this as an area addressed in practice or they deemed it an area of practice for which they had no education or training. For example, three therapists expressed as follows: ‘I’ve never done anything to help the patient drive easily. I’ve never seen that [in my practice]’ (P7). ‘I don’t remember receiving anything about driving [in my education]’ (P6). ‘This is not something that is addressed [in practice/in our education]’ (P8). ‘We came up with a form. It is not standardised … the therapists gathered and talked about what we needed to know and gather from research and stuff’ (P3). 2. Lack of training and supporting infrastructure (opportunities)
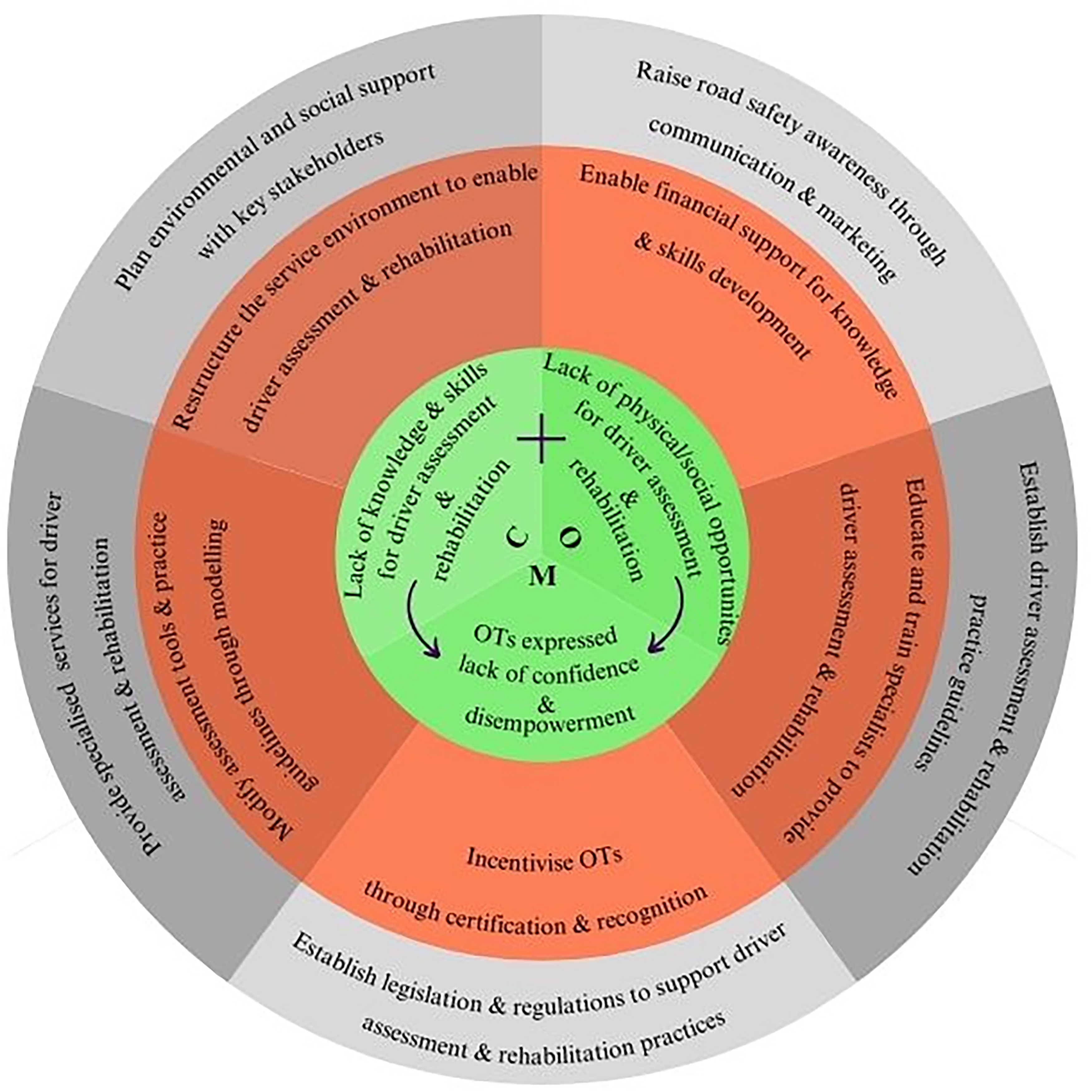
BCW application to the study findings: green represents the behaviour source through the COM-B model, orange represents the intervention functions, and grey represents the policy categories.
This theme concerns external factors that therapists viewed as affecting their ability to engage in driver assessment-related practice, specifically (i) lack of educational and practice opportunities and (ii) lack of supporting infrastructure.
Lack of Educational and Practice Opportunities
Most therapists reported that they had not been exposed to driver assessment and rehabilitation during their occupational therapy studies at university. Therefore, therapists not only lacked the opportunity to learn about it during their educational journey, but also lacked access to educational resources and training opportunities: ‘During my study for the bachelor's degree, I have never been exposed to this subject’ (P4). ‘If I had the proper training, if I knew the proper assessment, if I had the proper equipment to conduct these assessments like, you know, I should be able to conduct that assessment’ (P9). ‘The doctors have a big role to play in this because normally they would have to write medical forms for the patients to inform them about the safety issue, and then a patient can be referred to OT for further assessment. Unfortunately, this is not something that physicians address’ (P8).
Lack of Supporting Infrastructure
This includes the physical/environmental and the social infrastructure needed for conducting driver assessments and rehabilitation in Saudi Arabia.
i Inadequate physical environment and equipment
Therapists identified the lack of suitable physical spaces and equipment necessary for driver assessment and rehabilitation, explaining, ‘There is not enough space or equipment to facilitate the driving assessment and rehabilitation’ (P12). Also, several therapists noted that the cost of equipment is a significant barrier; for example, one therapist said: ‘The company that has the pieces of [car modification] equipment or the advanced systems, there's not a lot in Riyadh, only one. It was costly’ (P7). There was also some suggestion that therapists experienced funding delays if modification is required: ‘There could be available funds, but then the waiting time is prolonged’ (P8).
ii Inadequate social infrastructure
The therapists’ experience suggests that the social infrastructure in Saudi Arabia does not currently provide adequate support for them in conducting driver assessments and rehabilitation.
First, there are no clear clinical guidelines available; therefore, therapists expressed frustration at having no clear guidelines, leaving their role in assessing medically at-risk drivers ambiguous. One therapist emphasised this point: ‘We need to make guidelines. A clear pathway for going to drive again, it is not feasible for you to implement something that is not clearly defined as your role’ (P12).
Second, there is a lack of clear policies and regulations for safely returning medically at-risk drivers to the road. One therapist stated, capturing this gap: ‘The health system and the legislation, not much covered in terms of what the legislation and regulations are for persons with a disability to go back on the road’ (P10). Another participant's response reinforced this point, highlighting the confusion and lack of clarity even among authorities: ‘First of all, there are no rules or regulations that are clear to us on how to integrate them in this society and make them drive safely. From like authorities and police, it's not clear for us, not clear to them too’ (P2).
Despite these challenges, therapists generally maintained a sense of optimism. They recognise the rapid evolution of the government and the positive changes being made, especially regarding road safety, which is reflected in their hopeful statements about future improvements, indicating an expectation of increased governmental support and adaptability in addressing these issues. ‘This is what I’m hoping with the current changes that are happening now in the Saudi and the kind of integration of the disabled people within the community to have those things to be addressed’ (P3). ‘I think governmental support will be big’ (P4). ‘I think one big facilitator is the flexibility of the government around changing stuff in the recent years’ (P1).
3. But it is hard (Motivation)
The therapists acknowledge their role in assisting at-risk drivers but expressed that their motivation to take on that role is challenged due to two key factors: (i) their lack of knowledge and skills, and (ii) inadequate social infrastructure to provide driver assessment and rehabilitation services to those in need. Both are associated with low confidence and feelings of disempowerment.
Low Confidence in Knowledge, Skills and Experience
Therapists recognise the importance of their role in driver assessment, but many feel unprepared to undertake it effectively. This sentiment is encapsulated in statements such as, ‘We know that it's our role. We know that we should do it, but we don’t know how. We don’t have experience’ (P6), highlighting a significant gap between understanding their role and being able to execute it. This lack of confidence and experience leads to feelings of uncertainty and helplessness, as reflected in remarks like, ‘I felt powerless. I wasn’t sure where to refer her for help’ (P8) and ‘I feel I am lost and do not know how to start the driving process’ (P11).
Disempowerment due to Inadequate Social Infrastructure
Even if occupational therapists were to gain the necessary knowledge and skills, many still reported facing challenges due to a lack of structured guidelines and regulatory support. One therapist voiced this dilemma, saying, ‘I’m not authorised to do it. My voice will not be considered, so why waste my time’ (P3). The critical need for formal guidelines and services is further stressed in comments such as, ‘We don’t have established guidelines or established services. It is not feasible to implement something that is not clearly defined as your role’ (P4) and ‘We cannot do much if the regulations are not in place to support us’ (P10).
4. Recommended Interventions
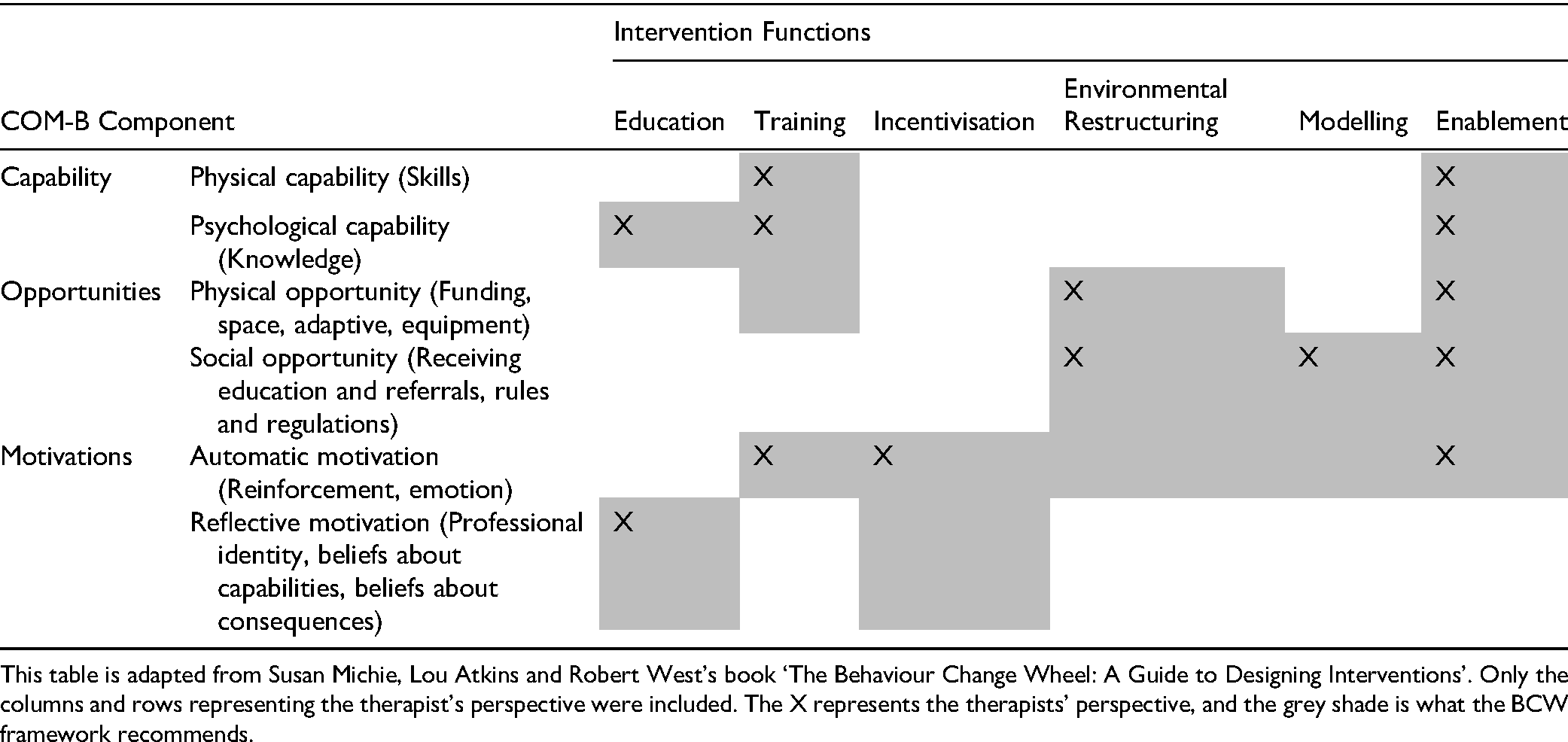
Table 2 provides an overview of the interventions recommended by therapists mapped to the BCW framework, followed by descriptions of the recommendations.
A Visual Matrix of the Intervention Functions Recommended by the Therapists Mapped to the BCW Framework.
Education and Training Provision
Therapists suggested that the priority could be to provide a training programme that would upscale their capabilities, including knowledge and skills, to enable them to integrate driver assessment and training into their practice. As these therapists said: ‘Provide OTs opportunities to get knowledge and be certified in driving rehabilitation for people with disabilities. This is the first thing’ (P11). ‘I think if there is a certain training for OTs around the country, we’ll take this role quickly’ (P4). ‘Finding the well-developed resources around the world to provide the training for the OT’ (P12). ‘Sending OTs to these countries will help start this process’ (P4).
Support through funding and recognition
Therapists emphasised the critical need for support through funding and paid time off work to make such opportunities a reality: ‘We need the sponsorship, for the financial requirement, and also for educational leave. These are the most important things’ (P5). ‘OTs have to travel abroad to learn about driving rehabilitation and get certified. It can cost a lot of money unless the person can be funded by a certain governmental or private facility to allow us to be certified’ (P11).
Assessments and Guidelines Modification to Model the Best Available Evidence
This theme highlights the perspective of occupational therapists on the need to adapt existing driver assessment and rehabilitation tools to suit the local context. This need arose from the recognition that most existing tools are standardised based on Western populations, which may not align well with the uniqueness of Saudi Arabia. There was a clear consensus among therapists that modifying international guidelines to fit the context of Saudi Arabia is vital.
One therapist highlighted the necessity of having ‘certain assessment tools that apply to our country, that can be translated into Arabic language, so it will be easier for therapists to use, and also it would be easier if the client had to get involved in the assessment’ (P11). This statement underscores the significance of language and cultural relevance in developing appropriate and relevant assessment tools. Another therapist suggested, ‘adaptations should reflect the society and the culture of the service’ (P10).
In achieving this, the role of the SOTA was considered pivotal. SOTA is seen as an ideal body to ‘guide the development of guidelines for Saudi Arabia in this particular field, through well-developed resources’ (P12). All participants emphasised the need for resources that are not only internationally informed but also locally adapted and sensitive to the specific requirements of the Saudi Arabian population.
5. Recommended Changes in Policies
On a broader policy level, therapists advocated raising awareness about broader road safety and service developments and establishing clear policies and legislation. Table 3 provides an overview of the recommended policy changes and approaches by therapists mapped to the BCW framework. These are described in more detail in the following sections.
Visual Matrix of the Policies Recommended by the Therapists Mapped to the BCW Framework.
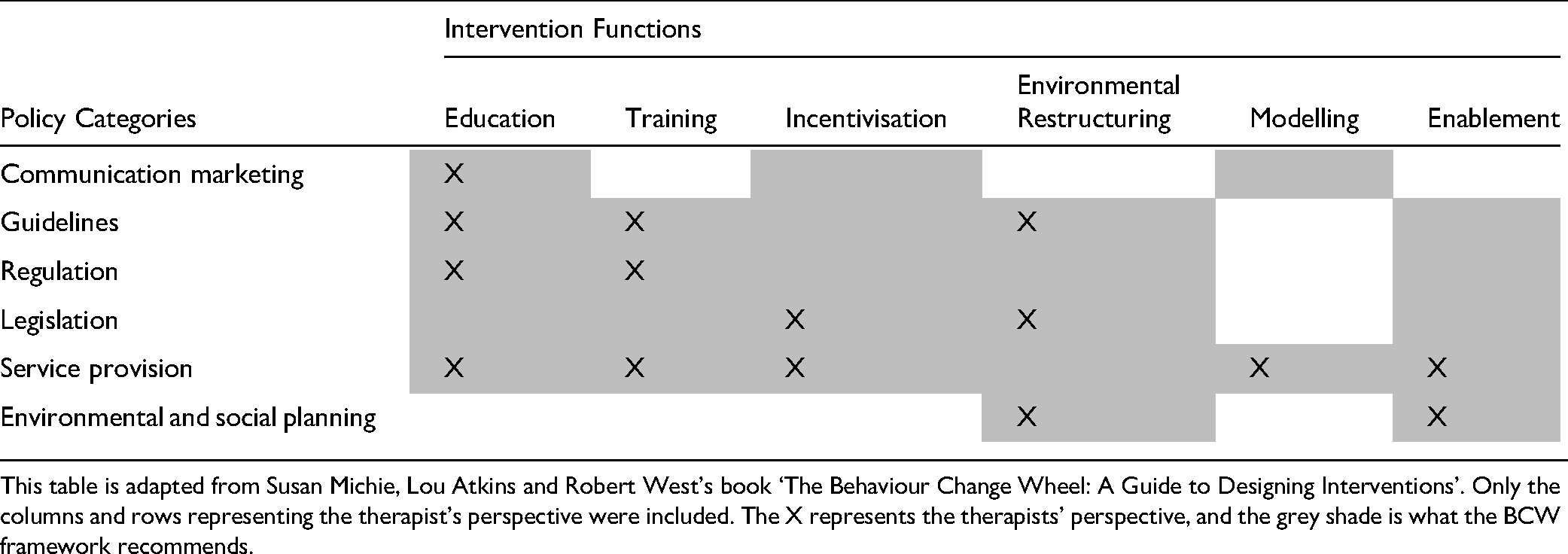
i Increased awareness to tackle road safety issues
Policies that guide increased community awareness, particularly the adoption of safer driving practices, were identified as an important aspect of tackling road safety as a prevention strategy since most trauma patients with severe injuries, such as traumatic brain injuries and spinal cord injuries, were involved in car crashes. As noted by one therapist: ‘As I told you, the vast majority of the conditions received daily are road traffic injuries, mostly young adults. They usually want to be independent again, and driving is one of the main domains that need to be addressed as it is considered the only way of transportation in Saudi Arabia’ (P4).
Therapists also suggested that at-risk drivers should be aware of the dangers behind driving without seeking a professional assessment. ‘Some community education about driving and the risks of driving while you have impairments, how would that affect the safety not only of other people around you but also your family and loved ones who could also be involved in an accident, that could then lead to serious injuries or death’ (P8).
ii. Advocating for policy change and legislative reform in driving assessment and rehabilitation
Therapists clearly stated they ‘need to advocate loud and clear about the legislation’ (P10). They see this as the cornerstone to initiating a dependable driver assessment and rehabilitation practice in Saudi Arabia. For example, therapists noted that: ‘When you change things on the policy level, it really changes the way things work’ (P1), and ‘until things are cleared in terms of legislation, people will not take driving assessment or driving rehab very seriously’ (P10).
Therapists suggested that policy changes should prioritise mandating fitness to drive assessment for at-risk drivers and recognise the occupational therapists’ role in the fitness to drive assessment process. They also pointed out a significant gap in current practices – drivers who have acquired their licence before an injury are not re-evaluated post-injury, which leads to them resuming driving without an assessment of their current abilities. As noted by (P3), ‘Sometimes they get the licence before the injury, no re-evaluation or re-assessment after the injury, and they will get back to driving regardless! so government regulations need to be strict’.
Moreover, most therapists explained that they currently lack the legal empowerment to make critical decisions regarding a patient's ability to drive safely. Therapists believe that they should be able to suggest regular evaluations if needed or even recommend licence suspension. They aspire to a system where ‘the police or traffic authority will support the OTs’ decision and report [if the driver should be restricted] as restrictions on the driving licence’ (P2). They also hope to have an integrated system where occupational therapists can directly work with the licensing authority; as (P11) suggested ‘having an occupational therapist that actually works with the licensing authority’ to bridge this gap.
iii Service development
This subtheme outlines a pragmatic approach the therapists suggested to introduce and scale-up driver assessment services in occupational therapy. They advocated for an initial manageable pilot programme to test and refine the service, followed by a thoughtful expansion to other areas. Central to their suggested approach is the formation of specialised teams, distinguishing between general screening by all occupational therapists and more in-depth assessments conducted by specially trained personnel.
Progressive Service Implementation
The therapists highlighted the need to advocate for change, ‘We should advocate for that service to be promoted’ (P9). Another therapist pointed out, ‘We should not just wait for the perfect moment to start everywhere, this is unrealistic’ (P2). This statement encapsulates the ethos of moving forward with service provision using available resources rather than awaiting ideal conditions.
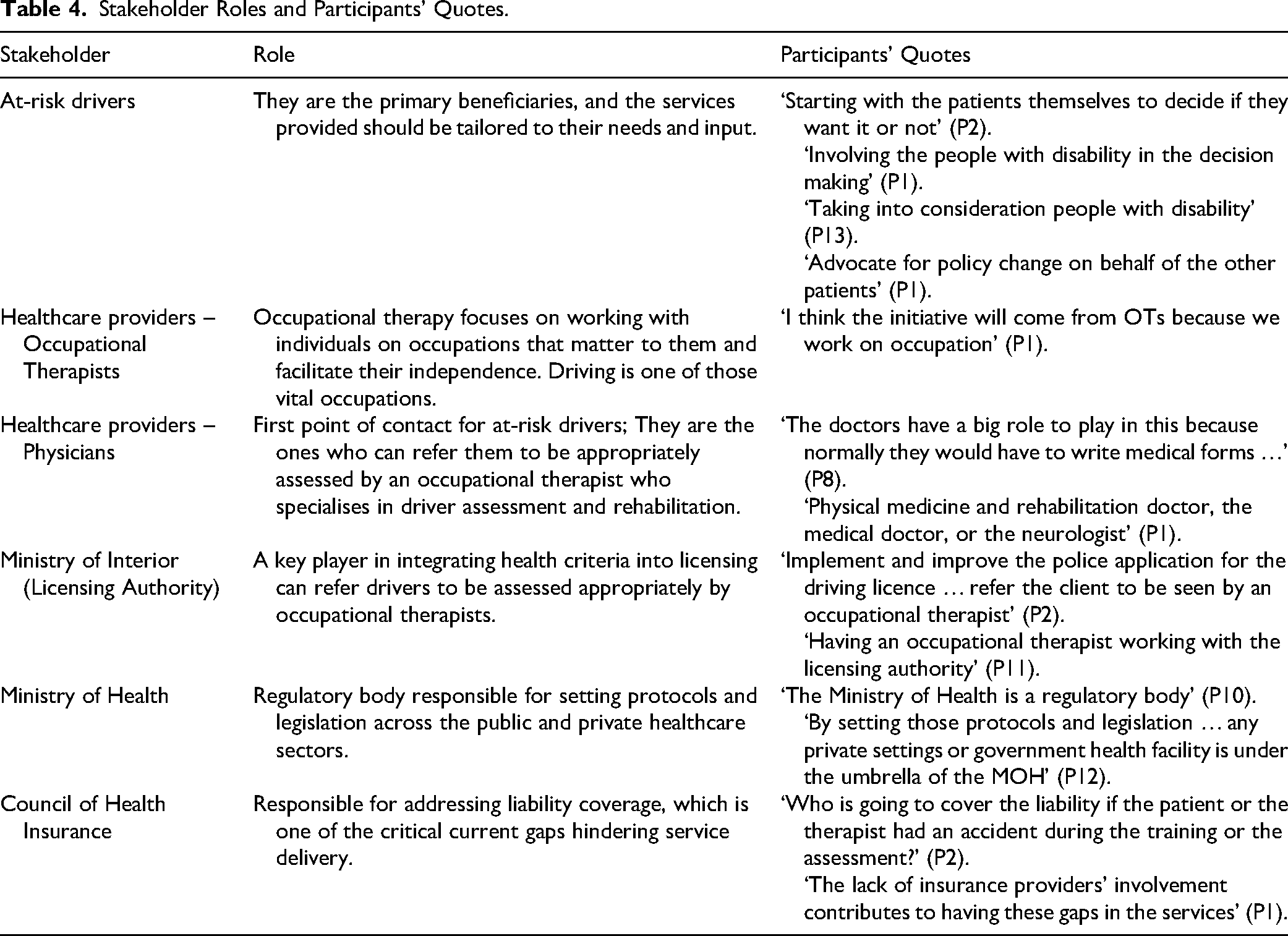
6. Collaboration
This theme emerged from the therapists’ perspectives on the significance of collaborative engagement with various stakeholders to improve driver assessment and rehabilitation services in Saudi Arabia. It highlights their opinion on the stakeholders’ diverse roles and contributions from service users to healthcare professionals, government bodies and insurance companies in shaping effective, user-centric and legally compliant driver assessment and rehabilitation practices. As noted by one therapist: ‘People need to have communication and proper networking to know from where to get what’ (P1).
One therapist illustrates the breadth of the collaborators’ background, saying, ‘We need further communication between different authorities … it's going to be not only interdisciplinary, but also it should be multidisciplinary, and it should involve different stakeholders’ (P12).
These stakeholders include at-risk drivers, healthcare providers and government bodies. The findings regarding each stakeholder's role as perceived by the participants are presented in Table 4.
Stakeholder Roles and Participants’ Quotes.
Discussion
Study participants acknowledged that they needed further training to be equipped with sufficient knowledge and practice skills. Similar findings regarding the need for additional training in this specialised area of practice were reported by Swedish occupational therapists in a survey exploring their involvement in driver assessment (Larsson et al., 2007). In addition, Scott et al. (2021) reported a lack of knowledge and confidence regarding returning to driving assessment and available tools among Australian occupational therapists who have not received training in driver assessment. Similarly, this study's findings suggest that many occupational therapists in Saudi Arabia are neither confident nor motivated to provide driving-related services. This is not surprising considering that the profession of occupational therapy is relatively new in Saudi Arabia, compared with in Australia, where both the occupational therapy profession and the field of driver assessment are well-established.
An Australian study suggested that educating occupational therapists about the competency standards for assessing at-risk drivers is associated with increased adherence to these standards in clinical practice (Fields et al., 2023). Another Canadian study suggested that continuing education initiatives provide opportunities to enhance clinicians’ skills and knowledge, thereby building their capacity (Vander Veen et al., 2023).
Enable and Incentivise Clinicians to Engage in Education and Training Opportunities
The ‘Motivation’ component of the COM-B model (Michie, 2011) targets the therapists’ conscious and unconscious decision-making process along with their impulses, drives and values. Study participants suggested there could be some benefits in motivating clinicians to undertake training and education through financial and non-financial means, such as funding, paid leave and certification and recognition. These suggestions reflect the enabling and incentivisation intervention functions recommended by the BCW (Michie et al., 2014). The therapists’ opinions are well supported by previous research. For example, a review of incentives for motivating health workers emphasised the importance of supporting education, training and professional development through financial and non-financial means (Henderson et al., 2008).
Professional certification and recognition are also supported in the literature, and countries such as Australia, the United States and Canada have offered specialised education and training programmes for occupational therapists in driver assessment for many years (Unsworth, 2012). Therefore, the therapists’ suggestion regarding establishing education and training programmes with certification in Saudi Arabia is recognised as an essential step towards enabling clinicians to be confident in addressing the return to driving safely within their scope of practice.
Develop a Contextually Adapted Driver Assessment and Rehabilitation Framework for Service Provision
The BCW framework also identifies potential barriers to a specific behavioural change beyond the person's capabilities and motivations (Michie, 2011). Therefore, a change in the environment, including social and physical contexts, may facilitate the person's opportunities to participate in the desired behaviour.
Study participants emphasised the need to establish practice guidelines to support clinicians and other stakeholders in addressing safe return to driving issues. They also noted the need to modify these guidelines, including the assessment tools used in the evaluation process to suit the Saudi Arabian context, which supports the findings of Alhashmi et al., (2023) noting that clinical assessment tools and on-road assessments should be prioritised for modification to suit the Saudi Arabian context. Modelling and guidelines establishment are two of the BCW's compatible and effective strategies to support the therapists’ recommendations (Michie et al., 2011). Various established resources could be modelled and utilised to create Saudi Arabian-specific practice guidelines.
The therapists also highlighted the need for adequate physical and social context to facilitate the driver assessment and rehabilitation practice in Saudi Arabia. They emphasised the critical role of clear legislation and regulations to guide the practice of driver assessment and rehabilitation and facilitate service delivery. More importantly, the therapists acknowledged the need to involve key stakeholders, including at-risk drivers, governmental bodies and health professionals, to achieve the needed change within Saudi Arabia.
As therapists in the present study stressed, the service provision should be client-centred, and it was suggested that at-risk drivers should be part of the process before initiating driver assessment and rehabilitation services. At-risk drivers have lived experience of driving and driver safety issues. They can have meaningful input regarding what they need regarding driver assessment and rehabilitation service provision. Consumer involvement is well-supported in the healthcare literature across various disciplines and has led to more efficient and sustained implementation of healthcare services (Lowe et al., 2021). The active participation of at-risk drivers ensures that services are tailored to their unique situations and aligned with their specific needs and expectations. It also fosters a sense of ownership and empowerment among individuals, resulting in more successful and sustainable outcomes in health service implementation (Lowe et al., 2021).
Therapists also emphasised that practice models must be tailored to the specific context of Saudi Arabia, rather than directly copying models from other countries. The diversity within and across countries regarding healthcare systems, legal frameworks and cultural norms necessitates this tailored approach. Consideration of the unique infrastructure, driving conditions and social factors prevalent in Saudi Arabia is also necessary to ensure any proposed framework is feasible, effective and culturally sensitive within the Saudi context. These guidelines will aid clinicians in making informed decisions, aiming to enhance community mobility and autonomy for at-risk drivers and ensure the safety of all road users in Saudi Arabia (Alhashmi et al., 2023). The conversation about driver assessment and rehabilitation in Saudi Arabia necessitates a multidisciplinary, collaborative effort to design a practical and contextually relevant framework.
Limitations and Future Research Directions
Some limitations of this study include that the sample was small, and there may be selection bias since recruitment was based on advertising via the professional association and snowball sampling. The sample may also not reflect the views of most occupational therapists in Saudi Arabia. This is especially relevant given the recent development of the profession in Saudi Arabia (Aljabri et al., 2024) and the observation that most practising Saudi occupational therapists in rehabilitation are relatively junior and inexperienced. However, insights from these therapists offer a valuable understanding of occupational therapy practices in Saudi Arabia, particularly in driver assessment and rehabilitation. Further research, such as a nationwide survey of all occupational therapists, may help in understanding the overall landscape of driver assessment and rehabilitation service provision in Saudi Arabia. While the generalisability of results to a broader population is not typically the primary aim of qualitative research, contextual information about the study setting helps readers make informed judgments about the extent to which the results are transferable to their context (Fossey et al., 2002). We have presented participant demographics to aid transferability (Kuper et al., 2008). However, since the interviews were designed to enable data collection by telephone, it was not possible to collect detailed contextual information about the rehabilitation service settings where participants worked. A further issue that we encountered was that the interviewed therapists were from different rehabilitation facilities, making it difficult to identify specific sources of the challenges presented.
Future research should adopt a collaborative and participatory approach (Lowe et al., 2021) to advocate for clear policy and legislation regarding the assessment of at-risk drivers in Saudi Arabia. This should include the following actions.
Firstly, qualitative studies should be conducted to enhance our understanding of driving and community reintegration experiences from the perspectives of people with disabilities due to road traffic injuries
Secondly, an understanding of the perspectives of rehabilitation physicians is necessary to comprehend their viewpoint on assessing at-risk drivers in Saudi Arabia, informed by their practice experience with at-risk drivers, the healthcare system and the licensing authority.
Thirdly, a careful review of suitable international driver assessment and rehabilitation models should be conducted to assess their effectiveness and potential adaptability to the Saudi Arabian context. This includes searching and reviewing published manuals, guidelines and academic literature to inform the development of a draft policy framework to be implemented in Saudi Arabia.
Lastly, co-design workshops should be conducted with key stakeholders, including but not limited to at-risk drivers, their families, physicians, occupational therapists and the licensing authority. The perspectives of occupational therapists in this research, as well as those of at-risk drivers, their families and physicians, should be presented, along with the review findings on a practical and adaptable international model for the Saudi Arabian context, so as to co-create a Saudi Arabian-specific driver assessment and rehabilitation policy framework guided by the BCW framework.
In summary, this collaborative research approach can influence various aspects of healthcare, from individual care plans to service provision improvements and even system-wide reforms. By working together, all stakeholders can co-create solutions that are more effective, efficient and aligned with the needs of the Saudi Arabian context.
Implications for Occupational Therapy Practice
Based on our findings, we recommend the following actions to support occupational therapists entering the field of driver assessment and rehabilitation in Saudi Arabia:
Provide specialised education and training opportunities through collaborating with established driver evaluation programmes overseas to guide the development and delivery of workshops or education for occupational therapists, physicians and driver instructors in Saudi Arabia. Incentivise occupational therapists to complete training in driver assessment and rehabilitation through certification and recognition. Occupational therapists equipped with the needed knowledge and skills can take the following actions. Establish driver assessment and rehabilitation practice guidelines. Collaborate with relevant stakeholders to co-create legislation and regulations to support driver assessment and rehabilitation practices. Provide specialised services for driver assessment and rehabilitation.
Conclusion
Through this qualitative inquiry, occupational therapists indicated that their lack of knowledge and skills is not the only barrier to providing driver assessment and rehabilitation in Saudi Arabia; there is a need for clear policy and legislation to support their practice. Without these resources in place, at-risk drivers will continue to be either isolated and unable to re-integrate into their community, or they will resume driving without appropriate assessment and support, potentially endangering themselves and others on the road and creating a vicious cycle of more road traffic injuries.
The findings highlight the need for multidisciplinary and collaborative efforts to enhance driver assessment and rehabilitation practices in Saudi Arabia, as the barriers are multifaceted and cannot be addressed by a single entity.
Footnotes
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.