
Abstract
Importance
Poor prosthetic satisfaction in individuals with upper limb loss has been linked to delayed or nonspecific rehabilitation. The Suitcase Packing Activity (SPA) is a functional outcome measure which has been validated in healthy individuals and assesses bimanual and unilateral upper limb function through a goal-directed task.
Objective
To validate the SPA by investigating the relationship between SPA scores and patient-reported outcomes (PROs).
Design
Cross-sectional cohort study.
Setting
Military treatment facilities, community events, and prosthetic clinics.
Participants
Individuals over the age of 18 with major upper limb loss or limb difference who could speak/read English.
Outcomes and Measures
Participants completed the SPA and questionnaires on patient characteristics, Patient-Reported Outcomes Measurement Information System (PROMIS®), and Disabilities of the Arm, Shoulder and Hand (DASH). SPA categories are time, accuracy, and efficiency. Pearson correlations evaluated relationships between SPA subscales and continuous variables. Linear regression determined if DASH score and age could predict SPA scores. Commonality analyses determined the unique, common, and total variance of SPA subscales explained by predictor variables.
Results
Twenty-nine individuals with upper limb loss and limb difference (18 M, age:37.8 ± 12.0, time since amputation:15.7 ± 14.7years) participated in this study. Age, PROMIS® Social Subscale, and DASH were associated with SPA scores. Age and DASH predicted SPA Time and Efficiency.
Conclusions and Relevance
SPA scores align with better PRO scores and demonstrate that the SPA has sufficient concurrent validity to evaluate function in patients with limb loss. Further investigation is warranted to use this measure to compare baseline function or changes over time.
Plain Language Summary
Individuals with upper limb loss and limb difference often need to adapt and use creative strategies to perform activities of daily living. The findings from this study indicate that the SPA may be a useful tool for occupational therapists to evaluate their patients’ abilities to perform salient tasks, such as packing a suitcase, even if they are using unique strategies to perform that task.
Introduction
Poor prosthetic satisfaction in individuals with upper limb loss or difference has been linked to delayed rehabilitation or the utilization of a nonspecific rehabilitation program which does not reflect the individual's needs (Resnik et al., 2012). Previous studies of Veterans with upper limb loss found that 52.3% of male and 76.5% of female veterans reported abandoning their upper limb prosthesis due to dissatisfaction with their device (Resnik et al., 2020). As such, it is essential for clinicians to have access to clinical outcome measures which can quickly and accurately assess the needs of individuals with upper limb loss and limb difference to help bridge the gap between rehabilitation and optimal upper limb function.
Although a wide variety of outcome measures have been validated for individuals with upper limb and limb difference, there is limited evidence to support any one gold standard metric for evaluating physical function and guiding clinical practice in this group (Crunkhorn et al., 2023). Of the 16 functional outcome measures recommended by Veterans Affairs/Department of Defense Clinical Practice Guideline for the Management of Upper Limb Amputation Rehabilitation, all but one requires that the patient be in the prosthetic phase of rehabilitation (Crunkhorn et al., 2023). Many of these metrics have strong psychometric properties and can easily be performed in a clinical setting, however, they often rely on symmetry or bilateral limb engagement as a metric of success (Crunkhorn et al., 2023; Rapin et al., 1966; Resnik et al., 2013), making them less useful for individuals who either do not use an upper limb prosthesis or who use a prosthesis, such as a hook, which do not match the contralateral limb function or anatomy. Other metrics include tasks that aren’t salient to the patient and require expensive specialized equipment to perform (Hebert & Lewicke, 2012; Rapin et al., 1966; Resnik et al., 2023; Surrey et al., 2003).
The Suitcase Packing Activity (SPA) is a functional outcome measure which assesses bimanual and unilateral upper limb function through the goal-directed task of packing a suitcase (Baumann et al., 2017). Both fine and gross motor tasks are incorporated into this low-cost outcome measure through salient tasks, such as rolling a belt into a coil, placing different colored beads into a 7-day pill bottle, and attaching a luggage tag to the packed suitcase (Baumann et al., 2017). Scoring on the SPA is based on the ability and time to complete a task, rather than upon the strategy used to perform that task, making it a potentially useful tool for evaluating upper limb function with or without the use of a prosthesis for individuals with upper limb loss. The SPA was established as a reliable tool for evaluating healthy individuals (Baumann et al., 2017) and after burn injury (Cancio et al., 2024). However, the utility of this outcome measure for evaluating physical function in individuals with upper limb loss has not been established.
Average Demographics and Outcome Measures Data Across Participants.
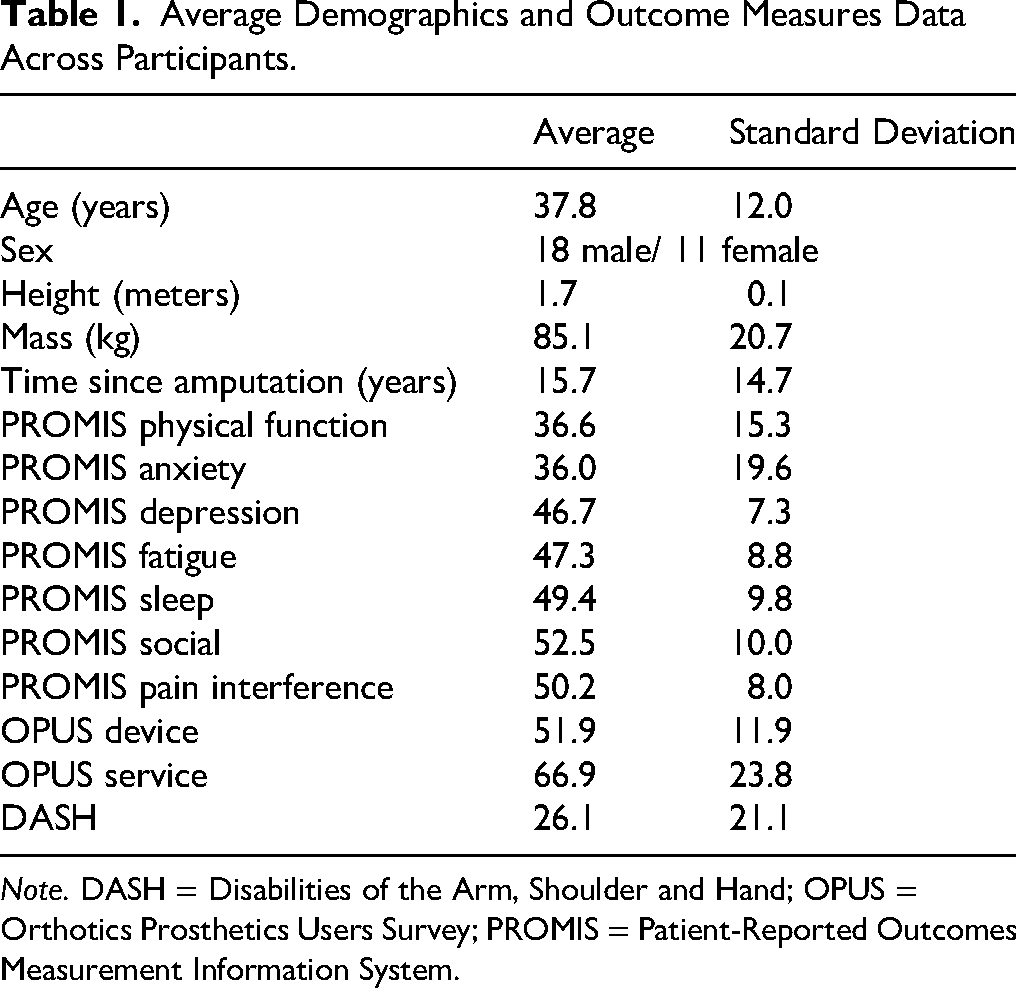
Note. DASH = Disabilities of the Arm, Shoulder and Hand; OPUS = Orthotics Prosthetics Users Survey; PROMIS = Patient-Reported Outcomes Measurement Information System.
As the SPA has not been validated in the upper limb loss population, this study aims to investigate the relationship between SPA scores and patient-reported outcomes (PROs) validated to assess upper limb function, global health, and psychosocial constructs in individuals with limb loss. The authors hypothesized that demographic characteristics, including younger age and shorter time since amputation, and better scores on previously validated PROs would be predictive of better SPA scores.
Methods
This cross-sectional cohort study consisted of 29 individuals who participated in a larger study assessing the differences in function and wellness of community-dwelling individuals with limb loss and limb difference. Participants were included if they had major upper limb loss or limb difference, could speak/read English, and were at least 18 years of age at the time of data collection. Participants were recruited from Military treatment facilities, community events, and local prosthetic clinics. The three Military treatment facilities included Naval Medical Center San Diego, Walter Reed National Military Medical Center, and Center for the Intrepid/Brooke Army Medical Center. Community events included the Amputee Coalition National Assembly, events with the Challenged Athletes Foundation, and the American Orthotic and Prosthetic Association National Assembly. Eligible participants provided written consent approved by the Naval Medical Center San Diego Institutional Review Board (NMCSD.2017.0039).
Data was collected in person over one session via questionnaires and the SPA. Questionnaires entailed patient characteristics, as well as standardized patient-reported outcomes. Participant characteristics included demographics and limb loss characteristics, which included time from amputation to testing, cause of amputation, and amputation level. For individuals with limb difference, their “time since amputation” was reported as their time since birth and their “cause of amputation” was defined as congenital.
Patient-Reported Outcomes
Patient-Reported Outcomes Measurement Information System (PROMIS®-29) ( Hafner et al., 2017 ; Hays et al., 2024 ; Horn et al., 2020 ; Sperring et al., 2021 ). PROMIS® is intended for clinicians and researchers in various disciplines who are interested in measuring physical, mental, and social health among individuals with various chronic conditions. The PROMIS®-29 is comprised of seven different subscales (physical function, anxiety, depression, fatigue, sleep, social, and pain interference) which are scored separately. All PROMIS® scores are reported on a T-score metric with a T-score of 50 aligned with the general population mean and a standard deviation of 10. Higher scores indicate more of the quantity being assessed. The PROMIS® has shown to have excellent reliability and moderate to high responsiveness. The minimal clinically important difference for PROMIS® domains ranges from 1.9 to 3.4.
Orthotics Prosthetics Users Survey (OPUS) ( Heinemann et al., 2003 ). OPUS-Satisfaction is a 21-item questionnaire that assesses satisfaction with constructs relevant to prosthesis and/or orthosis users and can be broken into two subscales: Satisfaction with Devices (items 1–11) and Satisfaction with Services (items 12–21). Each item is scored on a Likert scale ranging from 1 (“strongly agree”) to 6 (“strongly disagree”) with an additional “not applicable/don’t know” option available that is not scored; scores are summed, and higher scores on each subscale indicate greater satisfaction with the prosthetic or orthotic device and related services, respectively. An MDC90 value of 15.7 points has been reported among adults with lower limb loss.
Disabilities of the Arm, Shoulder and Hand (DASH) ( Beaton et al., 2001 ; Franchignoni et al., 2014 ; Galardini et al., 2024 ). The DASH is a 100-point scale widely used for the assessment of individuals with musculoskeletal disorders of the upper limb, consisting of 30 questions; 0 indicates no upper extremity disability or difficulty. MCIDs range from 8.3 to 18.0; pooled MCID is 11.00 points (95% confidence interval [CI] = 8.59–13.41; I2 = 0%). The pooled MDC90 is 9.04 (95% CI = 6.46–11.62; I2 = 0%).
Suitcase Packing Activity (SPA) ( Baumann et al., 2017 ). The SPA is a 20-item functional outcome measure which assesses an individual's ability to perform tasks on a step-by-step packing list. Scoring is based on three categories: time, accuracy, and efficiency. Time scoring is based on the amount of time it takes for the individual to complete all components of the outcome measure, with lower scoring indicating the individual completing the outcome measure more quickly. Accuracy scoring is based on the number of tasks that the individual accurately completed, with a score of 1 indicating a complete task and a score of 0 indicating an incomplete or incorrectly completed task. Accuracy scoring is on a scale of 0 to 20, with higher scoring indicating greater accuracy. Efficiency scoring is the difference between time and accuracy scoring, with a lower score indicating better overall SPA performance. When evaluated in healthy individuals, the SPA was found to have good to excellent interrater reliability (ICC3,1 ≥ 0.91) (Baumann et al., 2017). Additionally, SPA scores were found to be moderately correlated with other hand evaluations including the Southampton Hand Assessment Procedure (SHAP) and Minnesota Manual Dexterity Test (MMDT) (Baumann et al., 2017).
Statistical Analysis
Demographic and PRO data was reported as means and standard deviations. Pearson correlations determined the relationships between SPA subscales and continuous variables (age, height, mass, time since amputation, and other patient-reported outcomes). Linear regression determined if DASH score and age could predict each SPA subscale score. Commonality analyses determined the unique, common, and total (unique + common) variance of each SPA subscale explained by predictor variables. Commonality analysis is a nonparametric test which decomposes the total R2 of a regression model into the percent of variation attributable to each variable and each pair of variables, called a commonality coefficient. Commonality coefficients can be further divided into a positive and a negative effect, where the positive effect is the expansion of explained variation attributable to the addition of the variable and the negative effect is the reduction of explained variation of the other variables in the model when said variable is introduced. For the Pearson correlations and linear regression, significance was set a priori to α=0.05. All analyses were performed in R version 4.3.2 (2023-10-31) programming software.
Results
Twenty-nine individuals with unilateral or bilateral upper extremity amputations participated in this study (Table 1). Levels of amputation were: partial hand (2), bilateral partial hand (1), shoulder disarticulation (1), transhumeral (6), transradial (12), transradial/transhumeral (2), bilateral transradial (1), and wrist disarticulation (4). Causes of amputation were: blast (2), cancer (1), congenital/limb difference (6), disease (1), electrocution (5), motor vehicle accident/motorcycle accident (3), and trauma (10). Participant characteristics and patient-reported outcomes are described in Table 1.
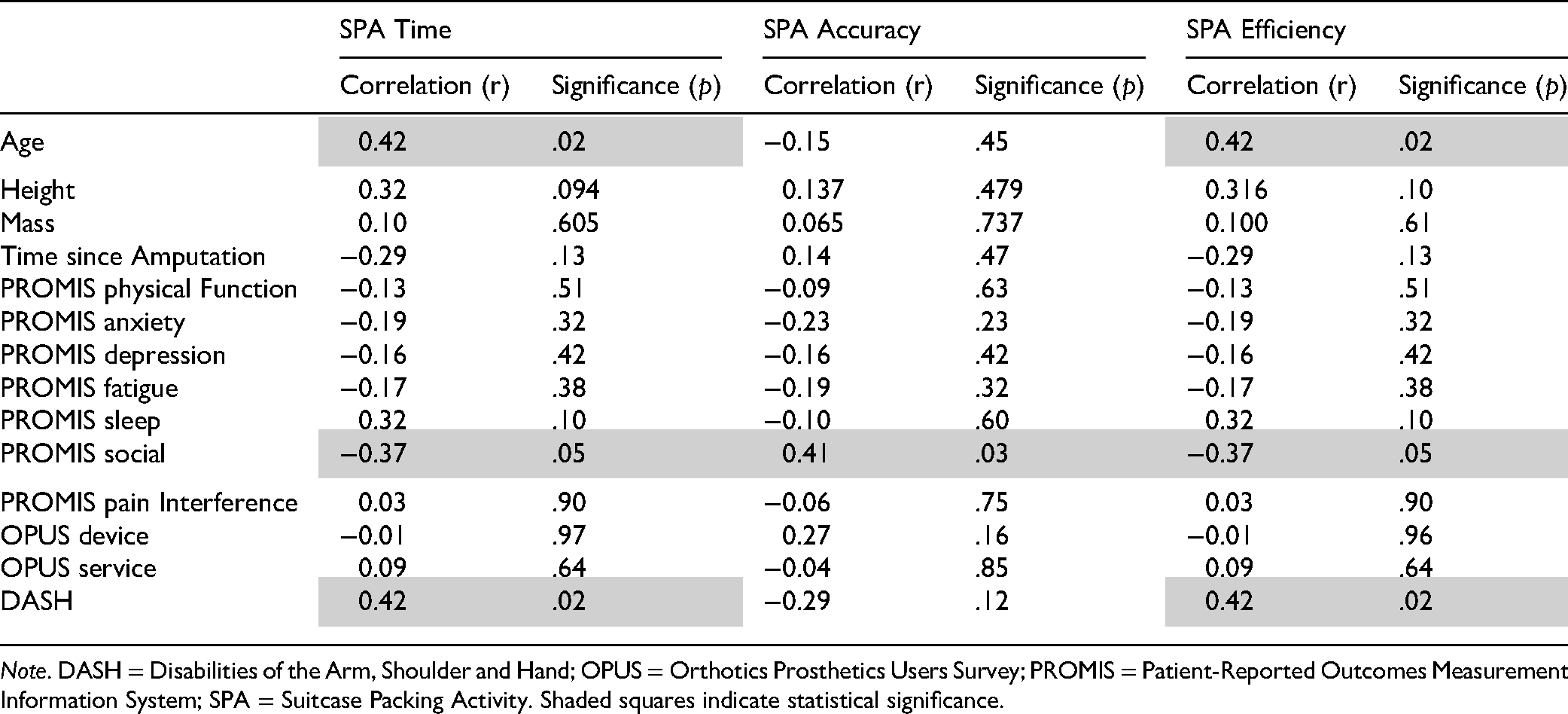
Correlations (r) and Significance (p) Between the SPA Subscales, Demographic and Morphological Data, and Patient Reported Outcomes.
On average participants completed the SPA in 627.7 ± 304.5 s, with accuracy and efficiency scores of 19.1 ± 1.5 and 608.6 ± 304.8, respectively. Participants most struggled with filling a small, 3 ounce shampoo bottle from a larger shampoo bottle (10.5% of participants), moving beads from a pill bottle into a 7-day of the week pill box (13.2% of participants), and putting toiletry items into a toiletry bag and sealing it closed (21.1% of participants).
Age, PROMIS® Social Subscale, and DASH were associated with SPA scores; no other associations were identified between SPA scores and patient-reported or demographic data (Table 2). Based on these findings, age, and DASH scores were identified to be included as predictor variables in the regression analysis (Figure 1).
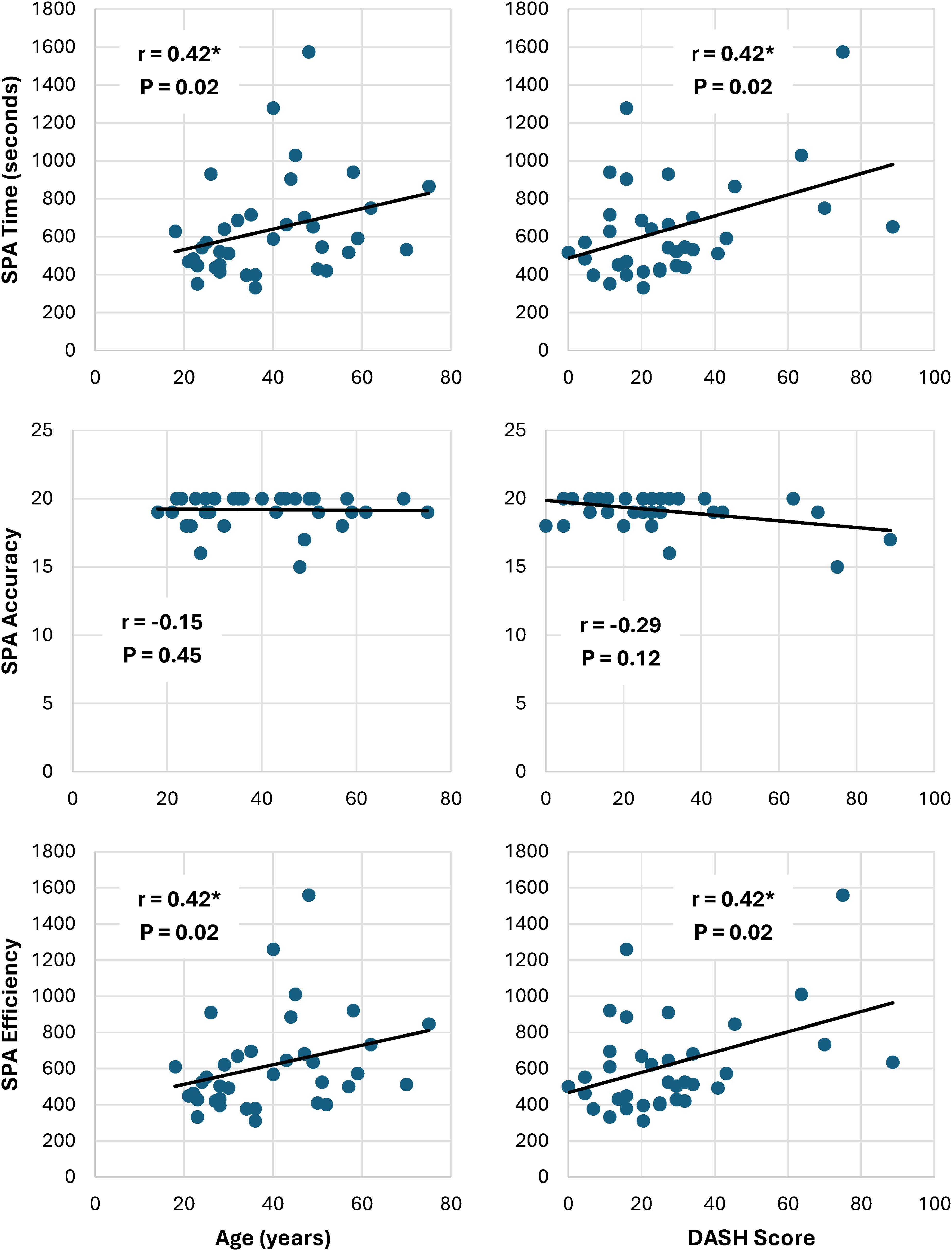
Correlations between the SPA subscales and demographic and patient reported outcomes data included in the regression model. For SPA Time and Efficiency scoring, a greater value indicates poorer performance, and for SPA Accuracy scoring, a lower value indicates poorer performance. Higher scoring on the DASH indicates greater disability or difficulty. Correlation coefficients (r) and significance (p) are reported in corner of each scatter plot; *indicates statistical significance. Note. DASH= Disabilities of the Arm, Shoulder and Hand; SPA= Suitcase Packing Activity.
Results From the Commonality Analyses Between Age and DASH Scores.
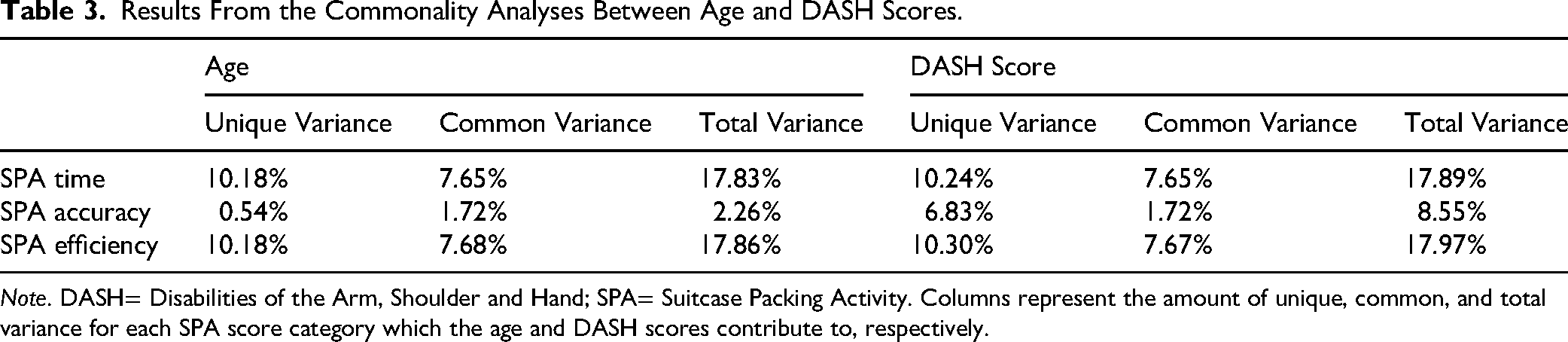
Note. DASH= Disabilities of the Arm, Shoulder and Hand; SPA= Suitcase Packing Activity. Columns represent the amount of unique, common, and total variance for each SPA score category which the age and DASH scores contribute to, respectively.
From the regression analyses, age, and DASH were able to predict SPA Time, F = 4.88, adjusted R2 = 0.22, p = .02. SPA accuracy could not be predicted from age and DASH (p = .30). Age and DASH were also able to predict SPA Efficiency, F = 4.90, adjusted R2 = 0.22, p = .02. Results from the commonality analyses are reported in Table 3.
Discussion
This study aimed to define the relationship between SPA scores and previously validated PROs in individuals with upper limb loss and limb difference. In alignment with our hypothesis, younger participant age and better DASH scoring were predictive of better SPA Time and Efficiency Scores, thereby establishing concurrent validity for evaluating upper limb function with the SPA in individuals with upper limb loss and limb difference. However, SPA Accuracy could not be predicted from DASH scoring or age. Additionally, no other demographic or patient-reported outcome data were correlated with SPA scores.
The SPA is intended to be an objective and composite measure of an individual's bimanual and unilateral hand function (Baumann et al., 2017). Many of the functional tasks included in this metric are similar to or touch on the same motor capabilities as the questions asked in the DASH. For example, the DASH asks individuals the level of difficulty for them to open a tight jar, write (Gummesson et al., 2003), or prepare a meal while the SPA asks individuals to open pill bottles and transfer them into a 7-day pill bottle, write their name and destination on a luggage tag, and compile a set of toiletry items and place them in a toiletry bag (Baumann et al., 2017). Previous studies have determined the DASH and its shortened version (QuickDASH) to have sufficient concurrent validity to evaluate disability and reported upper limb function in individuals with upper limb loss (Pyörny et al., 2024; Resnik & Borgia, 2015; Resnik et al., 2022; Resnik et al., 2021). As such, this overlap in tasks evaluated and the relationship found between DASH and SPA Time and Efficacy scores established in this study support the utility of the SPA for evaluating upper limb function individuals with upper limb loss.
Similarly, the relationship between age and SPA Time and Efficacy scores provide support for the utility of this metric. Previous studies have identified a relationship between increased age and a decline in upper limb dexterity and function (Martin et al., 2015). With this loss of dexterity, many of the fine motor tasks included in the SPA, such as picking up beads and placing them in a pill box (Baumann et al., 2017), are likely to become more difficult. For individuals with upper limb loss or limb difference, this decline in dexterity and physical function is important to capture and address early as these individuals typically demonstrate markedly less manual dexterity compared to intact individuals at baseline (Resnik et al., 2022).
Previous studies have identified a high prosthetic rejection rate in individuals with upper limb loss and limb difference (Resnik et al., 2020). The lack of association between scoring on the SPA and OPUS device and services satisfaction surveys identified in this study are likely a reflection of this trend. Many of the participants who performed well on the SPA in this study did so without the use of a device. These individuals did not use a prosthesis at baseline, either because they never felt that they needed one or because they were more functional without one. The OPUS device and services satisfaction surveys include questions such as “My prosthesis/orthosis is comfortable throughout the day” and “I am satisfied with the training I received in the use and maintenance of my prosthesis/orthosis” (Heinemann et al., 2003). For individuals who do not regularly use a prosthesis or who feel more functional without one, they would likely score poorly on these questions, regardless of how functional they are without a device. As such, this measure may not be the most appropriate to evaluate function in individuals with upper limb loss or limb difference.
Similarly, the limited association between SPA scoring and the PROMIS® subscales, including the PROMIS® Physical Function subscale, may be an artifact of what this patient-reported metric evaluates (Hafner et al., 2017; Hays et al., 2024; Horn et al., 2020; Sperring et al., 2021). The PROMIS® Physical Function subscale evaluates an individual's self-reported mobility as well as their ability to perform activities of daily living. It includes a set of four questions including, “Are you able to go up and down stairs at a normal pace?” and “Are you able to walk at a normal pace?” (Hays et al., 2024) which are important clinically but are unrelated to an individual's ability to perform the activities included the SPA quickly and efficiently.
Compared to previous analyses of healthy individuals, the participants in this study had poorer SPA Time and Efficiency scores, with up to a 359.3 s difference in SPA Time and 359.1 point difference in SPA Efficiency scores (Baumann et al., 2017). This finding is in alignment with previous literature which established that individuals with upper limb loss have markedly impaired dexterity compared to healthy, age matched individuals (Resnik et al., 2022). However, there appears to be less than 1 point difference in SPA Accuracy scores between healthy individuals and the individuals with upper limb loss and limb difference included in this study, with both groups scoring greater than an 18 of 20 on average (Baumann et al., 2017). Scoring for the SPA Accuracy subsection is binary, based on the individual's ability to complete the task without providing any weight to the strategy chosen to complete the task. Although this appears to limit the statistical significance of this subsection, it allows clinicians to evaluate the best strategy for each patient based on their specific needs. Many of the participants included in this study opted to use a simpler prosthetic device, or no device at all based on their needs and preferred methods for completing activities of daily living. For example, some participants with transradial amputations preferred not to use a prosthesis to open the pill bottles in task 7, because the friction provided by a prosthesis was much less than the skin grip from the crook of their elbow, making it harder to grip and open the bottle. Using the SPA, clinicians can identify which items their patients are struggling with and why. By placing higher priority on the time to complete each task in the overall SPA scoring, clinicians could prioritize the best strategy for each patient, without imposing preconceived notions based on previous experience. Factors such as device weight (Crunkhorn et al., 2023; Dizon et al., 2025; Salminger et al., 2022) and prehension ability (Bouwsema et al., 2010; Crunkhorn et al., 2023) could then be identified as limiting factors and clinicians could provide feedback onto the best strategy for each individual to efficiently perform functional tasks.
This study is the first to investigate the utility of the SPA outcome measure in individuals with upper limb loss and limb difference; however, there are several limitations worth commenting on. Firstly, it should be noted that the group included in this analysis represents a sample of convenience, with considerable variability in baseline characteristics, such as amputation level, prosthetic componentry, or rehabilitation history. As such, this research represents preliminary data which should be built upon in the future to determine if this measure is more or less useful in any subgroup or distinguish between subgroups of individuals with upper limb loss or limb difference. Additionally, given the cross-sectional study design, the authors were unable to evaluate changes over time. Future investigation is therefore needed to effectively use this measure in a clinical or research setting to evaluate baseline function or changes over time in upper limb function in this group. Finally, it should be noted that there is a potential for socioeconomic status bias built into the SPA given that some individuals may not have had the financial means to travel and therefore may not have previously packed a suitcase.
Implications for Occupational Therapy
The SPA measures an individual's physical function through their ability and the time it takes to perform the salient task of packing a suitcase, rather than focusing on their symmetry or ability to perform tasks unrelated to what they would typically perform in the community. Additionally, it is low cost as the components can be purchased at any retailer as long as the specifications are met, rather than requiring the use of a specific “kit.” Given that individuals with upper limb loss tend to use different strategies to perform activities of daily living, depending on factors such as their level of amputation, whether they use a prosthetic device, and their overall strength and mobility, occupational therapists need to have access to outcome measures which measure their patients’ ability to perform activities of daily living, even if they perform those activities using unique strategies. The findings from this work indicate that the SPA may be a useful clinical outcome measure for occupational therapists to evaluate their patients with limb loss and limb difference. However, further investigation is warranted for clinicians to effectively use this measure to evaluate their patients’ baseline function or changes in function over their course of treatment.
Conclusions
The SPA is a clinically useful tool for evaluating bimanual and unilateral upper limb function. The findings from this study indicate that SPA scores align with younger age and better scores on previously validated PROs. They also demonstrate that the SPA has sufficient concurrent validity for evaluating upper limb function in individuals with upper limb loss and limb difference. This indicates that the SPA may be a useful clinical outcome measure for evaluating and identifying opportunities to improve functional mobility in individuals with upper limb loss and limb difference.
Disclaimer
The views expressed in this manuscript are those of the authors, and do not necessarily reflect the official policy of the Uniformed Services University of the Health Sciences, Brooke Army Medical Center, Departments of the Air Force, Army, Navy, Defense, Veterans Affairs, nor the United States Government. The identification of specific products or scientific instrumentation does not constitute endorsement or implied endorsement on the part of the authors, Department of Defense, or any component agency.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.