
Abstract
Importance
Age-related declines in hearing and vision are common among older adults and are increasingly recognized as key determinants of functional independence. However, limited evidence exists on how sensory function (vision and hearing) shapes longitudinal trajectories of daily functioning over time.
Objective
To examine longitudinal associations between hearing and vision function and the trajectories of activities of daily living (ADLs) and instrumental activities of daily living (IADLs) among community-dwelling older adults.
Design
Longitudinal cohort study using latent growth curve modeling.
Setting
Community-based sample.
Participants
2,961 adults aged ≥ 65 years.
Outcomes and Measures
Self-reported sensory function, and functional performance in ADLs and IADLs.
Results
The mean age of participants was 73.637 years (SD = 5.990; 1,207 men, 1,754 women). Both ADL and IADL performance declined over time, with a steeper declines observed for IADLs (slope = −0.517, p < .001) than for ADLs (slope = −0.317, p < .001). Poorer hearing and vision function were associated with lower functional performance across waves, with stronger associations observed for IADL trajectories (β = 0.063–0.119). All latent growth models demonstrated acceptable fit.
Conclusions and Relevance
Sensory function was associated with adverse longitudinal functional trajectories, particularly for IADLs. These findings highlight the importance of routine sensory screening in occupational therapy (OT) practice and support older adults across the life span in order to help promote functional independence via stage-specific, individualized OT interventions that target the sensory impairment.
Plain Language Summary
As people age, hearing and vision often decline. These changes can make it harder to notice sounds and see details, which may affect daily functioning. This study found that older adults with poorer hearing and vision experienced greater difficulty performing daily activities over time. In particular, complex tasks, such as managing finances, using transportation, and handling medications declined more rapidly than basic self-care tasks (such as eating or dressing). This suggests that sensory decline may have a greater impact on complex daily activities than simple daily activities. Routine hearing and vision screening, along with tailored occupational therapy interventions, may help identify risks early and support older adults in maintaining independence in daily life tasks.
Introduction
The rapid growth of the aging population has increased the proportion of individuals experiencing age-related sensory decline in later life. Accordingly, sensory health among older adults has become a growing focus of public health and societal concern (World Health Organization, 2019, 2021). Vision and hearing are two sensory domains that are typically the most common of the senses to decline (Liu et al., 2022). Changes in these systems can significantly affect older adults’ ability to perceive environmental cues and perform daily activities (Liu et al., 2022; Tseng et al., 2018). Declines in vision and hearing have also been linked to reduced occupational performance and participation (Perlmutter et al., 2010). It contributes to qualitative deterioration in functional performance and poses a substantial threat to healthy aging (Liu et al., 2022; Tseng et al., 2018). From this perspective, sensory decline should not be understood as merely an individual-level concern. Rather, it represents a public health issue that necessitates consideration of both functional independence and caregiving burden in aging societies.
Additionally, declines in sensory function affect more than basic activities of daily living (ADLs), such as dressing and eating. Sensory impairment has been shown to negatively impact complex instrumental activities of daily living (IADLs) (Duran-Badillo et al., 2020). Mueller-Schotte et al. (2019) identified distinct trajectories of IADL decline according to sensory impairment type. Liang et al. (2023) showed that dual sensory impairment was associated with IADL performance. Beyond functional limitations, sensory impairment has been linked to psychological withdrawal, depressive symptoms, reduced quality of life, and elevated risk of disability (Duran-Badillo et al., 2020; Jin et al., 2025; Mueller-Schotte et al., 2019; Tseng et al., 2018; Wang et al., 2022). Moreover, within-person changes in sensory function have been shown to correspond with concurrent changes in functional disability over time (Jang et al., 2023).
Despite this evidence, important gaps remain in the literature. Many studies rely on cross-sectional designs, limiting the ability to examine how sensory impairment shapes functional performance over time (Liu et al., 2022; Tseng et al., 2018). Even among longitudinal studies, functional outcomes using global disability or composite scores, which may obscure distinct patterns of change in ADLs and IADLs (Jang et al., 2023; Mueller-Schotte et al., 2019). In addition, although vision and hearing function in a complementary manner in daily activities, most studies examine these sensory modalities independently, with limited consideration of their combined or cumulative effects on functional trajectories (Liang et al., 2023; Liu et al., 2022). Consequently, current evidence provides an incomplete understanding of how sensory impairments interact and accumulate over time to influence everyday functioning in later life.
Therefore, this study examines longitudinal associations between sensory impairment and trajectories of ADLs and IADLs among older adults, conceptualizing sensory-related functional decline as a dynamic process rather than a static outcome. Using national panel data and latent growth curve modeling (LGM), it further aims to identify domain-specific patterns of change in ADLs and IADLs to better capture differences in functional decline and their temporal characteristics. These findings may inform occupational therapists (OTs) on how to support older adults across the life span in order to help promote functional independence in later life.
Methods
Study Data
This study used a longitudinal design based on data from waves 6 to 9 of the Korea Longitudinal Study of Aging (KLoSA). The KLoSA is a nationally representative panel survey of community-dwelling Korean adults aged 45 years and older, conducted biennially by the Korea Employment Information Service (Oh et al., 2024). It collects comprehensive information on demographic characteristics, health status, functional ability, and socioeconomic factors. The survey employs a multistage, stratified probability sampling design based on geographic region and housing type to ensure national representativeness. Data are collected through computer-assisted personal interviews, with repeated follow up of the same individuals over time. As with most longitudinal studies, attrition occurs due to mortality and nonresponse.
Data from waves 6 to 9 were selected because of the consistent measurement of key variables, including ADLs, IADLs, and sensory function (hearing and vision), enabling the examination of recent functional trajectories among older adults. A total of 7,490 participants were included in wave 6. Individuals aged ≥65 years with complete data on all study variables across waves 6 to 9 were eligible for inclusion.
The final analytic sample comprised 2,961 older adults with complete data across all four waves. Missing data were addressed using listwise deletion, which may have introduced potential selection bias. This secondary analysis of de-identified, publicly available data was exempt from the institutional review board review.
Dependent Variables
Two functional outcomes were examined as dependent variables: ADL and IADL. The ADL measure comprised seven self-care activities: dressing, bathing, eating, toileting, transferring, walking, and continence. The IADL measure included ten more complex activities: meal preparation, shopping, money management, medication management, housekeeping, transportation use, and telephone use. Each item was assessed via self-report and coded as 1 (independent, no assistance required) or 0 (dependent, requiring assistance). Total scores ranged from 0 to 7 for ADL and 0 to 10 for IADL, with higher scores indicating better functional performance. ADL and IADL were assessed across waves 6 to 9 and modeled as separate longitudinal outcomes in the latent growth curve analyses.
Time-Varying Independent Variables
Hearing and vision were included as time-varying independent variables. Both sensory functions were assessed at each wave using self-reported five-point Likert scales, with higher scores indicating better function (1 = very poor to 5 = very good). Hearing and vision were specified as time-varying predictors of ADL and IADL at corresponding waves, enabling the examination of contemporaneous associations between sensory function and functional performance over time.
Covariates
Time-invariant covariates measured at wave 6 were included to control for potential confounding effects. These included age (continuous, years), sex (1 = male and 0 = female), residential region (1 = urban, 2 = suburban, and 3 = rural), educational attainment (1 = elementary school, 2 = middle school, 3 = high school, and 4 = college degree), employment status (1 = employed and 0 = retired), hearing aid use (1 = yes and 0 = no), and visual aid use (1 = yes and 0 = no). All covariates were specified as time-invariant predictors of both intercept and slope factors in the LGMs.
Statistical Analysis
LGM is a longitudinal analytic approach within the structural equation modeling framework that estimates initial status (intercept, i) and rate of change (slope, s) in repeatedly measured outcomes. Negative values indicate decline, whereas positive values indicate improvement over time. In this study, LGM was used to estimate trajectories of ADL and IADL across four waves. Model 1 (unconditional model) examined overall patterns of change in ADL and IADL over time. Model 2 (conditional model) incorporated time-varying sensory function as predictors and baseline covariates as time-invariant factors to examine their associations with ADL and IADL trajectories and to explain interindividual differences in intercept and slope factors. Slope factor loadings were fixed at 0, 1, 2, and 3 to reflect equal time intervals and model linear change over time (Bollen & Curran, 2006; Duncan & Duncan, 2009).
Model fit was evaluated using multiple indices, including the chi-squared statistic, root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker–Lewis index (TLI), and standardized root mean square residual (SRMR). RMSEA values < 0.08, CFI and TLI values > 0.90, and SRMR values < 0.08 were considered indicative of acceptable fit (Chen et al., 2008; Hu & Bentler, 1999; Marsh et al., 2004). Parameters were estimated using maximum likelihood estimation. All analyses were conducted in Mplus (version 8.4), with statistical significance set at p < .05.
Results
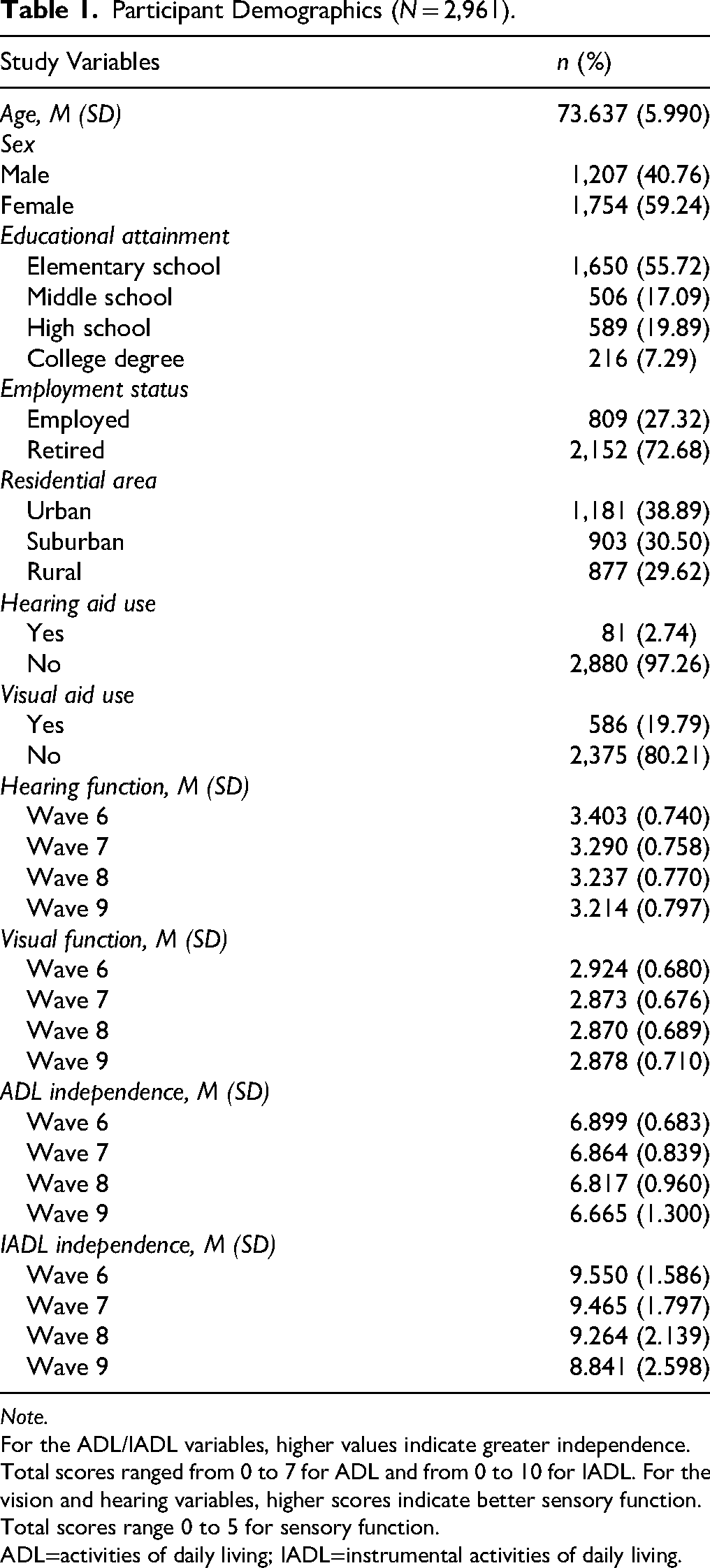
The demographic and clinical characteristics of the participants are presented in Table 1. The analytic sample included 2,961 community-dwelling older adults with a mean age of 73.637 years (SD = 5.990), and a higher proportion were women (59.24%) than men. Most participants had completed elementary education (55.72%) and were retired (72.68%). Participants resided in urban (38.89%), suburban (30.50%), and rural (29.62%) areas. Hearing aid use was rare, with only 2.74% reporting use at baseline. Across study waves, both ADL and IADL scores declined over time, indicating progressive functional limitations during follow up.
Participant Demographics (N = 2,961).
Note.
For the ADL/IADL variables, higher values indicate greater independence. Total scores ranged from 0 to 7 for ADL and from 0 to 10 for IADL. For the vision and hearing variables, higher scores indicate better sensory function. Total scores range 0 to 5 for sensory function.
ADL=activities of daily living; IADL=instrumental activities of daily living.
Model 1: Unconditional LGM
Model 1 Parameter Estimates for Unconditional LGM of ADL and IADL Change Over Time.
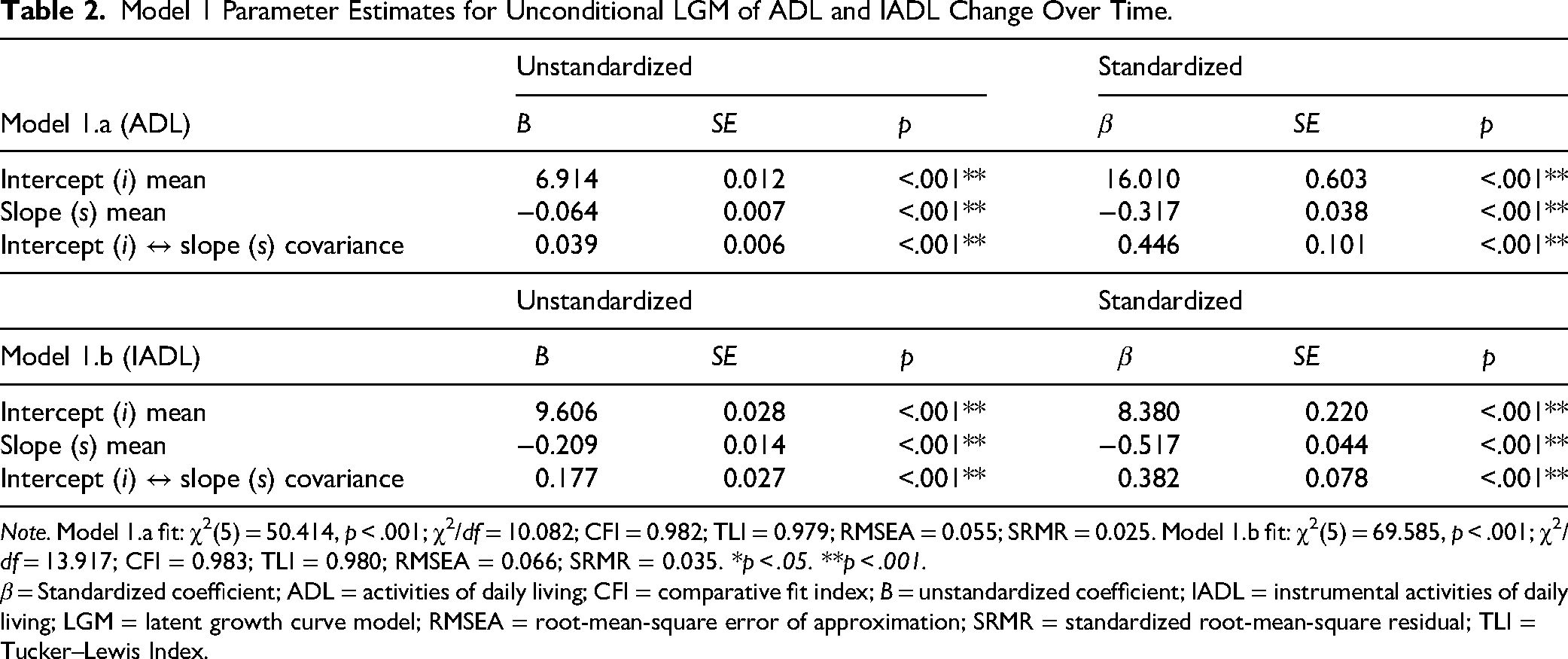
Note. Model 1.a fit: χ2(5) = 50.414, p < .001; χ2/df = 10.082; CFI = 0.982; TLI = 0.979; RMSEA = 0.055; SRMR = 0.025. Model 1.b fit: χ2(5) = 69.585, p < .001; χ2/df = 13.917; CFI = 0.983; TLI = 0.980; RMSEA = 0.066; SRMR = 0.035. *p < .05. **p < .001.
β = Standardized coefficient; ADL = activities of daily living; CFI = comparative fit index; B = unstandardized coefficient; IADL = instrumental activities of daily living; LGM = latent growth curve model; RMSEA = root-mean-square error of approximation; SRMR = standardized root-mean-square residual; TLI = Tucker–Lewis Index.
Similarly, for IADL (model 1.b), the intercept was 9.606 (SE = 0.028, p < .001), and the slope was −0.209 (SE = 0.014, p < .001), indicating a significant decline in IADL functioning over time. The intercept–slope covariance was also significant (B = 0.177, SE = 0.027, p < .001), implying a systematic association between baseline IADL levels and subsequent change trajectories.
Model 2.a: LGM of ADL With Time-Varying Sensory Function
Table 3 presents the results of the conditional LGM examining ADL trajectories, incorporating time-varying hearing and vision function and time-invariant covariates. The conceptual path diagram for model 2.a is shown in Supplemental Figure S1. Model 2.a demonstrated adequate model fit (χ2[43] = 116.429, p < .001; χ2/df = 2.707; CFI = 0.975; TLI = 0.962; RMSEA = 0.024; SRMR = 0.031).
Model 2.a Parameter Estimates for LGM of ADL Over Time With Time-Varying (Hearing and Vision Function) and Time-Invariant Covariates.
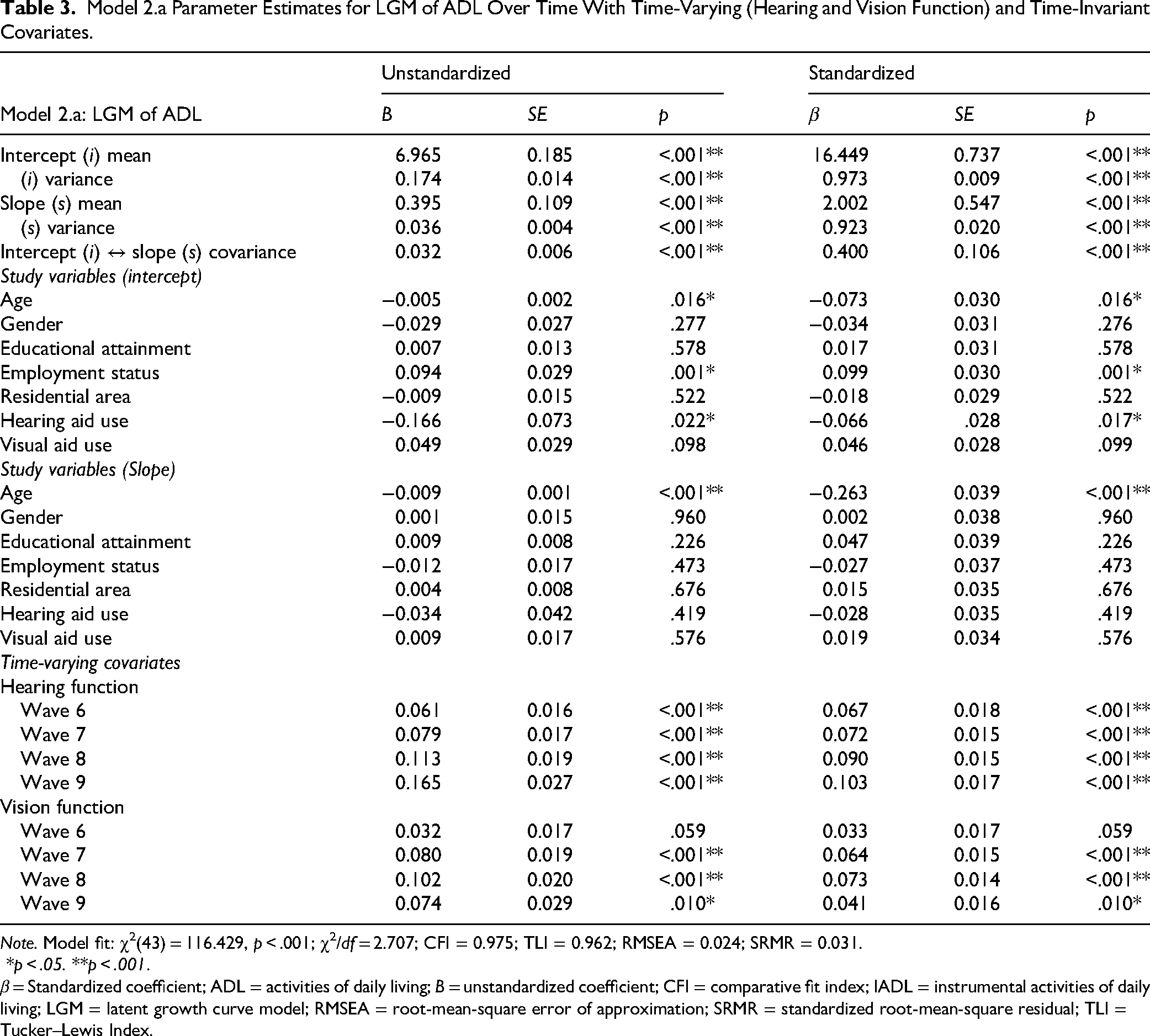
Note. Model fit: χ2(43) = 116.429, p < .001; χ2/df = 2.707; CFI = 0.975; TLI = 0.962; RMSEA = 0.024; SRMR = 0.031.
*p < .05. **p < .001.
β = Standardized coefficient; ADL = activities of daily living; B = unstandardized coefficient; CFI = comparative fit index; IADL = instrumental activities of daily living; LGM = latent growth curve model; RMSEA = root-mean-square error of approximation; SRMR = standardized root-mean-square residual; TLI = Tucker–Lewis Index.
The estimated intercept for ADL was 6.965 (SE = 0.185, p < .001), and the slope was 0.395 (SE = 0.109, p < .001), indicating significant longitudinal change after accounting for time-varying predictors and covariates. Accordingly, this adjusted slope may differ from the unconditional trend observed in model 1. The covariance between intercept and slope remained significant (B = 0.032, SE = 0.006, p < .001), indicating a meaningful association between baseline ADL status and its rate of change over time.
Among time-invariant covariates, employment status was positively associated with the intercept, whereas hearing aid use was negatively associated with the intercept. Age was negatively associated with both the intercept and slope. Regarding time-varying predictors, hearing function showed significant positive associations with ADL across all four waves (β range = 0.067–0.103, p < .001). Vision function was also positively associated with ADL, with statistically significant effects observed from wave 7 onward. Overall, better sensory function was consistently associated with higher ADL performance. The magnitude of hearing effects increased across waves, whereas vision showed no consistent temporal pattern.
Model 2.b: LGM of IADL With Time-Varying Sensory Function
The results of the conditional LGM for IADL are presented in Table 4. The conceptual path diagram of model 2.b is shown in Supplemental Figure S2. Model 2.b demonstrated acceptable model fit, although the chi-squared statistic was significant (χ2[43] = 238.848, p < .001; χ2/df = 5.554; CFI = 0.960; TLI = 0.938; RMSEA = 0.039; SRMR = 0.051), which is common in large samples.
Model 2.b Parameter Estimates for LGM of IADL Over Time With Time-Varying (Hearing and Vision Function) and Time-Invariant Covariates.
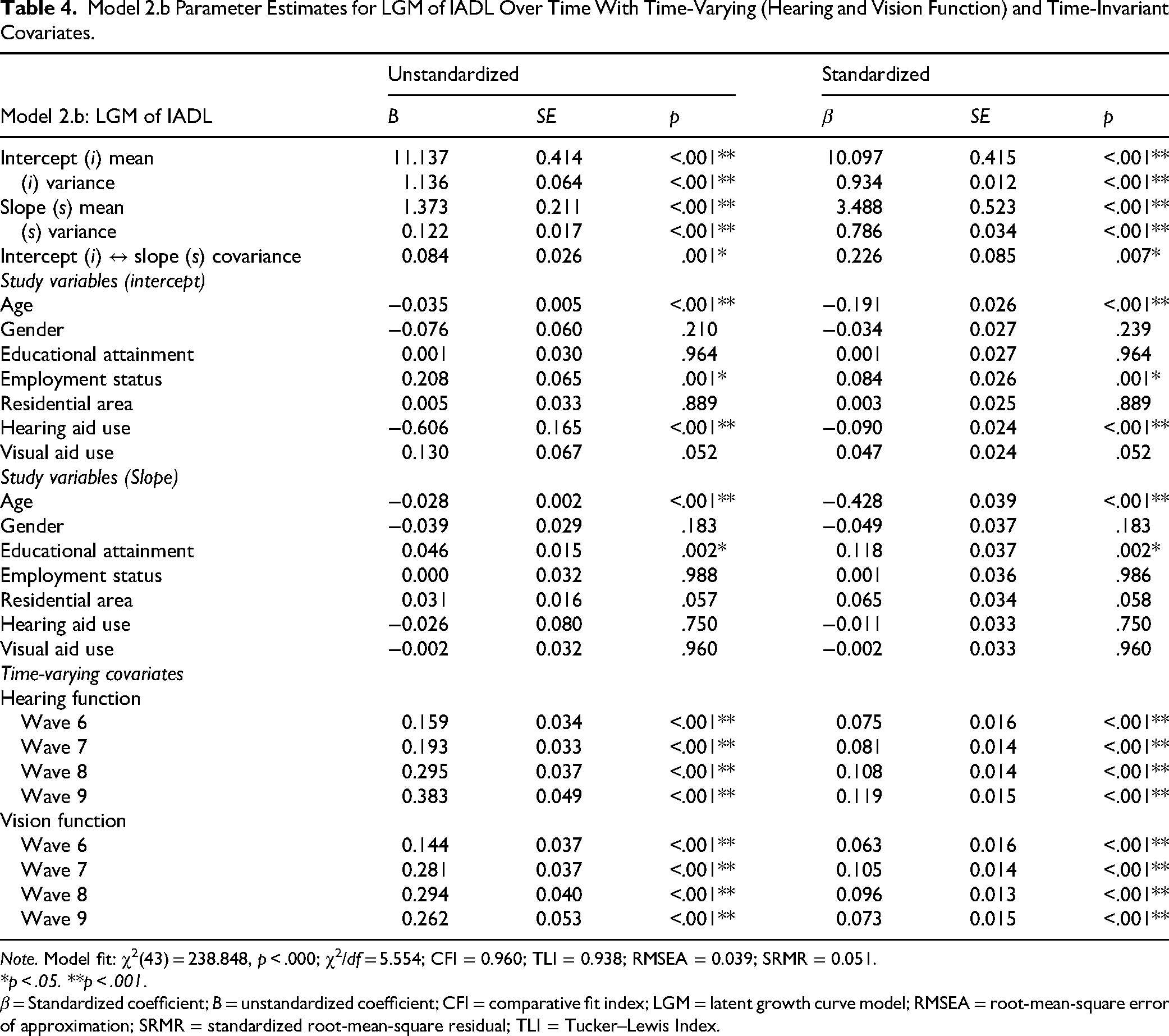
Note. Model fit: χ2(43) = 238.848, p < .000; χ2/df = 5.554; CFI = 0.960; TLI = 0.938; RMSEA = 0.039; SRMR = 0.051.
*p < .05. **p < .001.
β = Standardized coefficient; B = unstandardized coefficient; CFI = comparative fit index; LGM = latent growth curve model; RMSEA = root-mean-square error of approximation; SRMR = standardized root-mean-square residual; TLI = Tucker–Lewis Index.
The estimated intercept for IADL was 11.137 (SE = 0.414, p < .001), and the slope was 1.373 (SE = 0.211, p < .001). The intercept–slope covariance was statistically significant (B = 0.084, SE = 0.026, p = .001), indicating heterogeneity in IADL change depending on baseline functional status.
Among time-invariant covariates, age and hearing aid use were negatively associated with the intercept, whereas employment status was positively associated with the intercept. Age was negatively associated with the slope, while educational attainment showed a positive association with the slope. Regarding time-varying predictors, both hearing and vision were positively associated with IADL at all waves (β range = 0.063–0.119, all p < .001), indicating that better sensory function is consistently linked to higher levels of IADL performance over time. Consistent with the ADL findings, hearing effects increased across waves, whereas vision did not show a consistent temporal pattern.
Discussion
This study examined longitudinal trajectories of ADLs and IADLs and their associations with sensory function among community-dwelling older adults. The findings indicate that sensory function was significantly associated with both ADL and IADL performance over time. Standardized coefficients were consistently positive across all waves, suggesting that sensory function and functional performance changed in the same direction. The positive slopes observed in the conditional models reflect adjusted change after accounting for both time-varying and time-invariant covariates, rather than a simple increase over time. Given that both sensory function and functional performance declined across waves, the results suggest that reductions in sensory function are accompanied by concurrent declines in ADL and IADL performance. These findings are consistent with previous research demonstrating that sensory impairments are closely linked to functional limitations and reduced independence (Cimarolli & Jopp, 2014; Davidson & Guthrie, 2019).
Furthermore, the association between sensory function and functional performance was stronger for IADLs than for ADLs. This finding suggests that IADL tasks, which require higher levels of cognitive processing, environmental interaction, and sensory integration, may be more sensitive to changes in sensory function. Prior research similarly indicates that IADLs are a more sensitive indicator of early functional decline and show stronger associations with sensory impairment than basic ADLs (Bouscaren et al., 2019; Mueller-Schotte et al., 2019).
In addition, distinct patterns emerged for hearing and vision. Hearing function showed a gradually increasing association with functional performance across waves, whereas vision function did not demonstrate a consistent temporal pattern. This suggests that the effects of hearing decline on functional performance may accumulate over time, exerting a progressively greater influence on functional outcomes in later life. This interpretation is consistent with longitudinal evidence showing that changes in sensory function are linked to changes in functional decline over time (Jang et al., 2023; Mueller-Schotte et al., 2019) and is further supported by findings that hearing-related interventions, such as hearing aid use, are associated with improved functional outcomes (Assi et al., 2024).
The analysis of time-invariant covariates showed that age, employment status, and hearing aid use were significantly associated with baseline levels of both ADLs and IADLs, indicating that these factors contribute to differences in initial functional status. In contrast, age was the only significant predictor of change in ADL over time, whereas both age and educational attainment influenced changes in IADLs. These findings suggest that decline in basic functioning is primarily driven by biological aging, whereas changes in more complex functioning are additionally shaped by socioeconomic factors such as education (Liu et al., 2022).
OTs are well-positioned to translate these domain-specific patterns into targeted, client-centered interventions. The findings indicate that sensory function is closely associated with functional performance, with a stronger influence observed for IADL. Accordingly, OTs may consider assessing sensory function during IADLs, such as medication management and meal preparation. Furthermore, given that functional trajectories vary by age, education, and employment status, OT intervention strategies may need to be tailored according to individual risk profiles. Prior research has similarly highlighted that sensory impairments are closely linked to functional limitations and reduced independence in daily activities (Duran-Badillo et al., 2020; Perlmutter et al., 2010), while integrated sensory interventions have been shown to enhance functional participation and quality of life (Leroi et al., 2020). Although subgroup-specific intervention effects were not directly examined in this study, future research should further explore tailored, client-centered, OT approaches that account for individual characteristics.
Several limitations should be considered when interpreting the findings. First, selection bias may arise from including only participants with complete data across all waves. Second, sensory function was assessed using self-reported measures, which may not fully reflect clinical severity. Third, although sensory functions were modeled as separate time-varying predictors, their combined effects were only considered conceptually rather than empirically tested. Fourth, the reliability and validity of the ADL and IADL measures were not formally evaluated. Finally, although the longitudinal design enabled examination of functional trajectories, causal inferences cannot be established. Despite these limitations, the use of a large, nationally representative longitudinal dataset and LGM strengthens the robustness of the findings.
Implications for Occupational Therapy Practice
This study examined longitudinal associations between sensory function and trajectories of functional decline (ADLs and IADLs) among community-dwelling older adults, yielding the following implications for occupational therapy practice:
-Age-related sensory decline should be recognized as an important risk factor for functional deterioration in later life. -Given the stronger association between sensory function and IADLs than ADLs, OTs should prioritize assessment of sensory-related limitations in complex daily activities required for independent community living. These include medication management, financial management, shopping, transportation, and meal preparation. -The increasing association between hearing function and functional performance over time underscores the importance of ongoing and repeated assessment of sensory changes across the aging process.
Conclusion
Using data from a national database, we found that sensory function was related to longitudinal trajectories of both ADLs and IADLs among older adults. By conceptualizing sensory-related functional decline as a dynamic process rather than a static outcome, these findings underscore the importance of incorporating sensory status into functional assessment. Overall, the results have important implications for occupational therapy practice and aging research by highlighting sensory health as a key component of maintaining functional independence in later life.
Supplemental Material
sj-docx-1-aot-10.1177_19437676261464087 - Supplemental material for Longitudinal Associations Between Hearing and Visual Function and ADL and IADL Independence in Older Adults
Supplemental material, sj-docx-1-aot-10.1177_19437676261464087 for Longitudinal Associations Between Hearing and Visual Function and ADL and IADL Independence in Older Adults by Hanul Kim, Kimberly Hreha and Ickpyo Hong in American Journal of Occupational Therapy
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.