
Abstract
Importance
Family-centered occupational therapy (FCOT) Coaching Intervention improves child participation and parental skills, yet its use in hospital-based early intervention (EI) in Taiwan is limited.
Objective
To evaluate FCOT Coaching Intervention for enhancing daily participation and play in autistic children.
Design
Quasi-experimental, pretest–posttest design.
Setting
National Taiwan University Children's Hospital.
Participants
Nineteen autistic children (aged 2–6) and their parents. Families self-selected into FCOT Coaching Intervention group (n = 9) or control group (n = 10) based on transportation convenience.
Intervention
FCOT Coaching Intervention group comprised twice-weekly, 30-min sessions over 6 months, focusing on parent coaching and family-centered goals. Controls received traditional therapy in community clinics.
Outcomes and Measures
Child outcomes were assessed via Psychoeducational Profile–Third Edition (PEP-3), Vineland Adaptive Behavior Scale (VABS), and Revised Knox Preschool Play Scale (RKPPS). Parenting stress and family outcomes were measured with Parenting Stress Index–Short Form (PSI-SF) and Family Outcomes Survey–Revised (FOS-R). Goal Attainment Scaling (GAS) assessed individualized goals in FCOT Coaching Intervention group.
Results
Children who received FCOT Coaching Intervention showed significant gains in adaptive behaviors (p = .021), daily living skills (p = .026), and attention during play (p = .035). GAS revealed notable progress in play and daily activity participation. Parenting stress and family outcomes showed no significant group differences.
Conclusions and Relevance
FCOT Coaching Intervention effectively enhanced parts of functional participation and play in young autistic children in a hospital setting. Findings support expanding FCOT Coaching Intervention in EI and underscore the need for long-term follow-up.
Plain-Language Summary
This study evaluated the effectiveness of FCOT Coaching Intervention for young autistic children in Taiwan. Children in the FCOT Coaching Intervention group showed greater improvements than those in the control group in daily living skills and attention during play. Parents reported increased child participation, while parenting stress and family outcomes did not differ between or within groups. These findings support FCOT as an effective approach for hospital-based EI.
Introduction
Participation in play and daily activities is central to childhood. Play promotes exploration, socialization, communication, and motor development (Parham & Fazio, 2008), whereas participation in daily routines—such as feeding, dressing, and toileting—supports independence and self-esteem (Shepherd, 2014). Together, these occupations provide a foundation for lifelong development.
Autism spectrum disorder (ASD) is a neurodevelopmental condition affecting social interaction and communication, and characterized by restricted or repetitive behaviors (American Psychiatric Association, 2013). These features can disrupt children's participation in both play and everyday routines. Autistic children may show repetitive play patterns and experience difficulties engaging in daily activities (DeGrace, 2004; Miller-Kuhaneck, H. A., 2014; Pfeiffer et al., 2017).
ASD prevalence is increasing globally. Approximately 1.85% of children in the United States are affected (Maenner et al., 2020), compared with 0.36% in Asia (Qiu et al., 2020). In Taiwan, the reported prevalence of ASD is higher, at approximately 1.2%, than the broader Asian estimate (Hsu et al., 2012).
Given the participation challenges associated with ASD, emerging evidence supports participation-focused and caregiver-coaching approaches to improve play, activities of daily living (ADL), and family outcomes (Baker et al., 2023, Little et al., 2023, Weaver, 2015).
Family-centered practice (FCP) emphasizes family involvement in decision-making, planning, and service delivery for young children with special needs (Watling et al., 2023). Consistent with contemporary occupational therapy, parent coaching has been used to support children's social communication, play, and ADL participation (Chiu & Tseng, 2020; Foster et al., 2013; Little et al., 2018; Simpson, 2015), with moderate evidence for benefits in family-identified goals, occupational performance, and caregiver satisfaction (Watling et al., 2023). One established model is occupational performance coaching (OPC), a manualized, occupation-centered coaching intervention that uses collaborative performance analysis and parent-initiated solution finding to support participation in daily routines and play (Graham et al., 2009, 2010), with ongoing trials further strengthening the evidence base for coaching-based interventions (Graham et al., 2024). OPC emphasizes caregiver agency and parent-initiated solution finding as the primary mechanisms of change. FCOT Coaching Intervention includes in-session occupation-based demonstration or real-time guided practice within clinical settings.
The family-centered occupational therapy (FCOT) Coaching Intervention is a novel, hospital-based approach that combines caregiver coaching with in-session occupation-based activities (e.g., structured play activities and, when appropriate, small-group play opportunities). In this approach, parents contribute their intimate knowledge of the child's participation in daily activities, while occupational therapists provide professional expertise. Together, they observe the child's performance in the clinic and collaboratively develop strategies that are meaningful, feasible, and readily incorporated into family routines.
In Taiwan, early intervention (EI) services are largely delivered in hospital outpatient settings under the National Health Insurance system. Although home programs are recommended, they are often discontinued due to caregiver burden and implementation barriers (Chiang et al., 2016). Despite a 126% increase in EI funding—from NTD 356 M in 2016 to NTD 805 M in 2024 (Health Promotion Administration, n.d., Table 8.2.5)—evidence regarding the effectiveness of hospital-based family-centered intervention remains limited.
Therefore, this study aimed to develop and evaluate a hospital-based FCOT Coaching Intervention using parent coaching to enhance autistic children's participation in play and daily activities. Findings may inform policy, refine hospital-based EI services, and strengthen the evidence base for FCOT in occupational therapy.
Methods
Research Design
This study used a quasi-experimental design and was conducted at National Taiwan University Children's Hospital, a government-certified EI center providing developmental evaluations and interventions. Children were assigned to the FCOT intervention or control group based on parental preference: those receiving therapy at the hospital were in the intervention group, while those who did not were in the control group. This choice was usually influenced by the family's distance from the hospital and travel convenience. The study included a pretest, a 6-month intervention, and a posttest, aiming to evaluate the effects of FCOT with parent coaching on autistic children's participation in daily activities and play. Detailed information is presented in Figure 1.
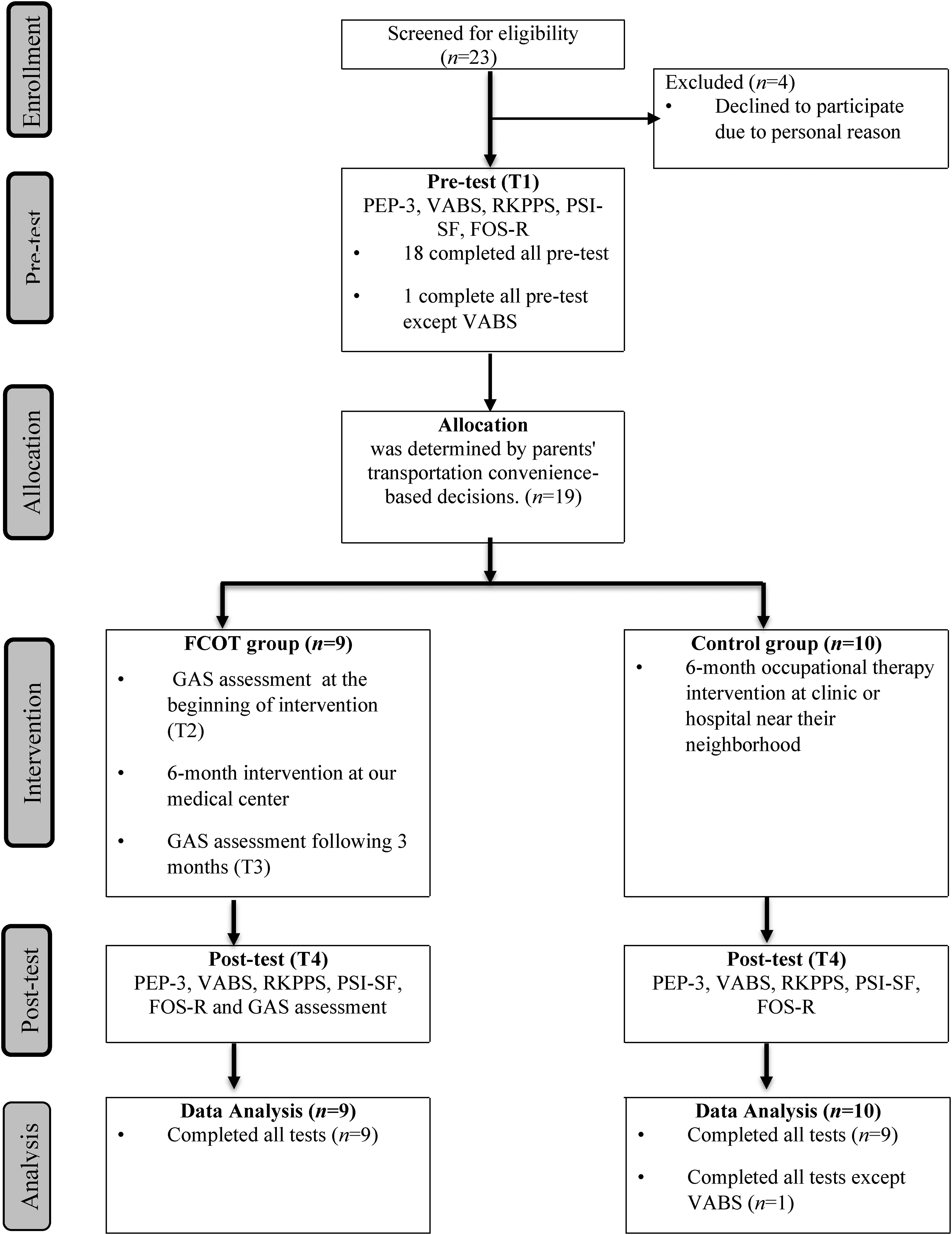
Research design.
Study Setting
Interventions took place in therapy rooms at National Taiwan University Children's Hospital, equipped with age-appropriate toys and materials.
Participants
Nineteen families participated in this study. Children aged 2–6 years were diagnosed with Autism Spectrum Disorder according to DSM-5 criteria by a multidisciplinary team. Children with comorbid neurological conditions were excluded. Participants were the child's primary caregivers who could consistently participate in twice-weekly 30-min sessions for 6 months, understand and communicate in Chinese, and agreed not to enroll their child in occupational therapy services provided at other hospitals or clinics during the study period.
Procedures
All procedures in this study were approved by the Institutional Review Board of National Taiwan University Hospital (NTUH), and the study was registered as a clinical trial with the Unique Protocol ID 201509008RINC.
Pretest assessments were conducted by a licensed occupational therapist with expertise in ASD who was blinded to group allocation, using the standardized tools PEP-3, VABS, RKPPS, PSI-SF, and FOS-R. The same therapist also conducted the posttest assessments 6 months later using the same tools. After the pretest, eligible participants were assigned based on whether parents and their children were willing to attend the hospital-based FCOT Coaching Intervention. Those who preferred to receive intervention at another hospital or clinic due to transportation or scheduling constraints were assigned to the control group. Information on the type and duration of interventions they received was collected.
Participants in the FCOT Coaching Intervention group participated in twice-weekly sessions for 6 months, focusing on parent coaching and collaborative goal-setting, while the control group received traditional therapist-directed therapy at community clinics. Parent-selected goals in the FCOT group were evaluated using the GAS. After 3 months of intervention, the therapist reviewed the child's goal attainment with parents; if the goals had been achieved, new goals were established. Goal attainment was reviewed again at 6 months using the GAS.
Child-Related Outcome Measures
Psychoeducational Profile, Third Edition (PEP-3)
PEP-3 is a standardized tool assessing communication, motor skills, and maladaptive behavior in autistic children aged 2–7.5 years (Schopler et al., 2005). The Chinese version of PEP-3 has been validated to have high internal consistency (.92–.98) and interrater reliability (.57–.94) (Fu et al., 2010).
Vineland Adaptive Behavior Scale (VABS)
The VABS assesses adaptive behavior across four domains—communication, daily living skills, socialization, and motor skills—combined into a total adaptive behavior score. The Chinese version of VABS used in our study demonstrates strong reliability: test–retest (.90), interrater (.74–.89), and split-half (.91–.99) (Wu et al., 2004).
Revised Knox Preschool Play Scale (RKPPS)
The RKPPS (Knox, 1997) assesses play development across four dimensions—space management, material management, pretense/symbolic play, and participation—encompassing 12 play behavior categories. It demonstrates strong interrater reliability (r > .80) and constructs validity (Bledsoe & Shepherd, 1982; Jankovich et al., 2008).
Goal Attainment Scale (GAS)
GAS is a criterion-referenced tool measuring individualized goals on a five-point scale: 0 indicates expected attainment, +1/+2 exceed expectations, and −1/–2 fall below expectations (Kiresuk & Sherman, 1968). GAS demonstrates strong reliability and validity across clinical and research contexts, including pediatric rehabilitation (Hurn et al., 2006; Palisano et al., 1992; Ruble et al., 2012).
In this study, GAS assessed three parent-selected goals related to their child's daily activity and play participation within the FCOT group. This individualized approach captured clinically meaningful progress aligned with family priorities.
Baseline: Child requires 1.5–2 h per meal, frequently distracted, needing prompts. Performance Levels: –2: >1 h with frequent distractions. –1: ≤1 h but remains distracted. 0: ≤1 h, no distractions. +1: ≤45 min, no distractions. +2: ≤30 min, no distractions.
Family-Related Outcome Measures
Parenting Stress Index-Short Form (PSI-SF)
The PSI-SF includes 36 items across three domains—parenting distress, difficult child, and parent–child dysfunctional interaction—rated on a 5-point scale, with higher scores indicating greater stress (Abidin, 1990). This study used the Chinese version, with total scores (sum of three domains) analyzed. Internal consistency ranged from .856 to .947, indicating high reliability (Wen, 2011).
Family Outcomes Survey-Revised (FOS-R)
The FOS-R evaluates EI effectiveness using a 5-point scale. It comprises: (1) family outcomes across five domains—understanding the child's strengths, needs, and abilities; knowing and advocating for one's rights; supporting the child's development and learning; having support systems; and accessing the community; and (2) helpfulness of EI indicators—knowing your rights, communicating your child's needs, and helping your child develop and learn. Internal consistency ranges from .73 to .91. This study used the Traditional Chinese version (Early Childhood Technical Assistance Center, n.d.); the original English version was developed by Bailey Jr. et al. (2011).
Intervention
The FCOT intervention was developed by a team of five occupational therapists with extensive EI experience. The intervention was delivered in a hospital outpatient setting and was grounded in child development frameworks, sensory integration principles (Bundy et al., 2002), and behavioral strategies addressing common challenges in play and daily routines. A licensed occupational therapist with early-intervention experience and training in parent coaching delivered FCOT using an evidence-informed coaching approach (Rush & Shelden, 2011). Core coaching processes included joint planning, guided observation, real-time action/practice, reflective questioning, and performance-based feedback. Through these processes, therapists supported caregivers to (a) analyze child behavior within everyday occupations, (b) identify naturally occurring learning opportunities, and (c) implement and adapt strategies within family routines.
To enhance transparency and replicability, FCOT was specified using the Rehabilitation Treatment Specification System (RTSS), including treatment targets, active ingredients, proposed mechanisms of action, and expected outcomes (Schwartz et al., 2022). A detailed RTSS specification and examples of therapist–caregiver coaching procedures are provided in the Supplementary Material.
A distinguishing feature of FCOT (relative to coaching-only protocols) was the integration of caregiver coaching with in-session, occupation-based demonstration. This integration supported real-time modeling, guided caregiver practice, and feedback in the clinic context. Intervention activities were individualized to caregiver-prioritized goals and used to demonstrate strategies while scaffolding caregiver skill acquisition. Each 30-min individual session followed a consistent structure: brief joint planning to review priorities and between-session action plans, followed by therapist demonstration and guided caregiver practice during occupation-based activities, and concluding with reflective discussion, feedback, and an agreed-upon plan for carryover to home routines. Session documentation captured the goals addressed, strategies practiced, and caregiver action plans for between-session implementation. For example, when a caregiver's goal involved turn-taking or sharing, the therapist structured a clinic-based play activity with the caregiver–child dyad or, when clinically appropriate, arranged a small-group play opportunity (3–4 children) to create natural social demands. If group play sessions were conducted, parent coaching was provided in the subsequent individual session. Caregivers were supported to observe the child's responses and the therapist's facilitation strategies and then practice the strategies with their child while receiving immediate coaching and feedback. Follow-up coaching discussions focused on generalizing these strategies to home routines and community contexts and tailoring them to family preferences and constraints.
The control group received usual occupational therapy and other therapies (e.g., ABA, play therapy) in the hospital outpatient setting. Only the total weekly therapy hours were recorded, and details of the treatment content were largely unavailable. According to caregivers’ reports, most interventions were therapist-directed, with children receiving direct therapy while caregivers remained outside the treatment room. No structured caregiver coaching provided.
Statistical Analysis
Baseline group characteristics were examined using nonparametric tests (χ2 or Fisher's exact tests, as appropriate). Given the small sample and non-normal distributions, within-group pre–post changes were analyzed using Wilcoxon signed-rank tests, and between-group differences in change (posttest–pretest) scores were evaluated using Mann–Whitney U tests.
For Goal Attainment Scaling (GAS), raw goal scores in the FCOT group were converted to standardized T scores (M = 50, SD = 10), with a T score of 50 indicating expected goal attainment. Wilcoxon signed-rank tests were used to evaluate the change in GAS T scores at 3 months and from 3 to 6 months within the FCOT group.
Statistical significance was set at p < .05 (two-tailed). Effect sizes were calculated as r (z/√N) for nonparametric comparisons and interpreted using conventional benchmarks (small ≈ .10, medium ≈ .30, large ≈ .50).
Results
Participant Characteristics
Nineteen children participated: nine in the FCOT group and ten in the control group. All completed pretest, intervention, and posttest phases. Participants in the FCOT group and control group were comparable in age (FCOT: 3.7 ± 1.1 years; control: 4.0 ± 1.1 years; p = .574) and gender distribution (FCOT: 6 boys, 3 girls; control: 9 boys, 1 girl; p = .303). Both groups received a similar amount of occupational therapy during the research period (FCOT: 1.02 ± 0.29 h/week; control: 0.95 ± 0.80 h/week; p = .348). However, the control group received significantly more hours of other treatments—including ABA, play therapy, psychotherapy, music therapy, speech therapy, and physical therapy—than the FCOT group (FCOT: 0.39 ± 0.49 h/week; control: 3.30 ± 3.61 h/week; p = .032). Baseline assessments revealed no significant differences in PEP-3, VABS, or RKPPS scores, confirming group comparability at study onset.
PEP-3 Results
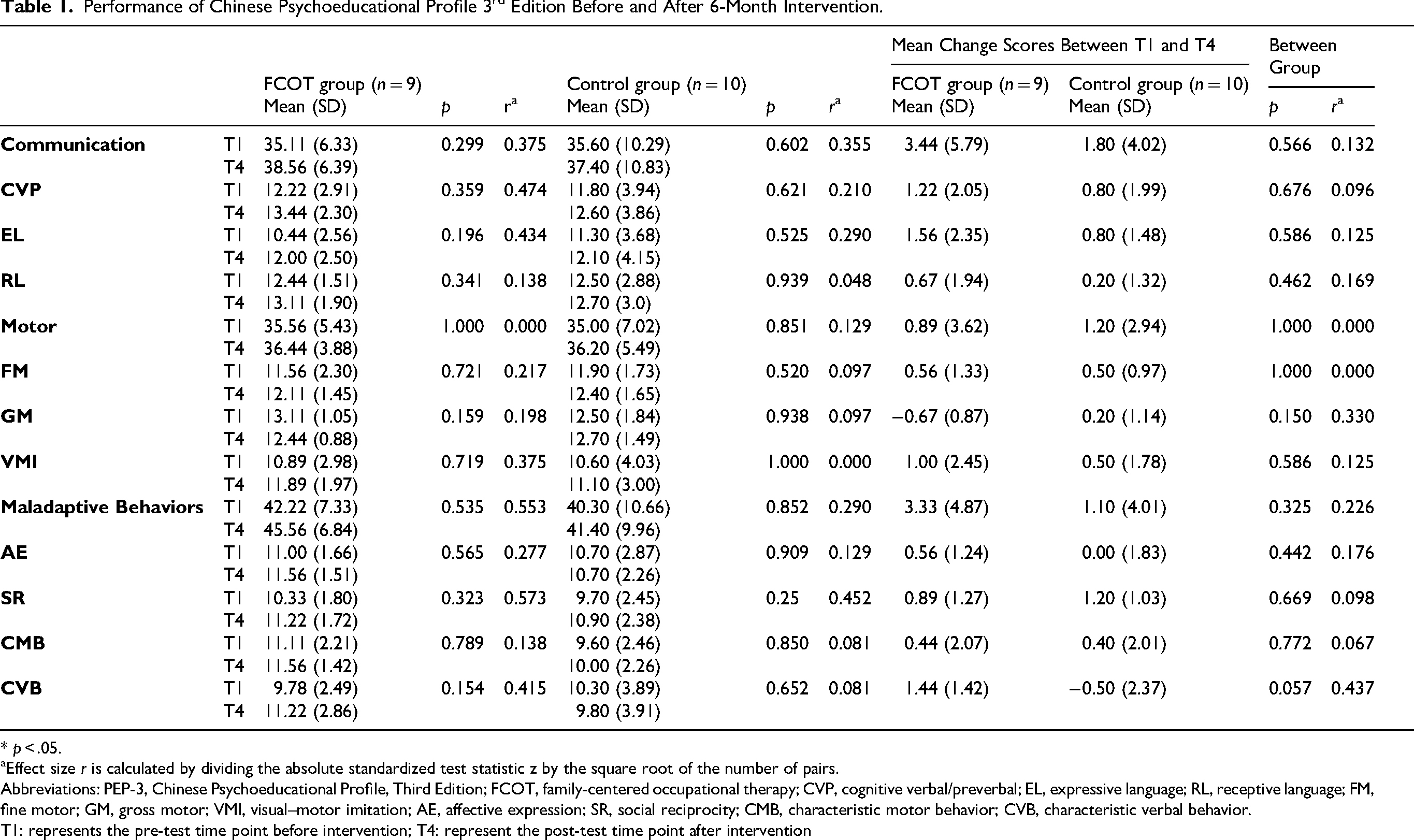
No significant within-group improvements were observed across composites or subtests in either group (ps > .05). However, the FCOT group demonstrated moderate-to-large effect sizes in Communication, Maladaptive behaviors, and five subtests: cognitive verbal/preverbal, expressive language, visual-motor imitation, social reciprocity, and characteristic verbal behaviors, suggesting substantial within-group improvements. In contrast, the control group showed moderate within-group effects only in communication and social reciprocity (Table 1). Between-group differences were generally non-significant.
Performance of Chinese Psychoeducational Profile 3rd Edition Before and After 6-Month Intervention.
* p < .05.
Effect size r is calculated by dividing the absolute standardized test statistic z by the square root of the number of pairs.
Abbreviations: PEP-3, Chinese Psychoeducational Profile, Third Edition; FCOT, family-centered occupational therapy; CVP, cognitive verbal/preverbal; EL, expressive language; RL, receptive language; FM, fine motor; GM, gross motor; VMI, visual–motor imitation; AE, affective expression; SR, social reciprocity; CMB, characteristic motor behavior; CVB, characteristic verbal behavior.
T1: represents the pre-test time point before intervention; T4: represent the post-test time point after intervention
VABS Results
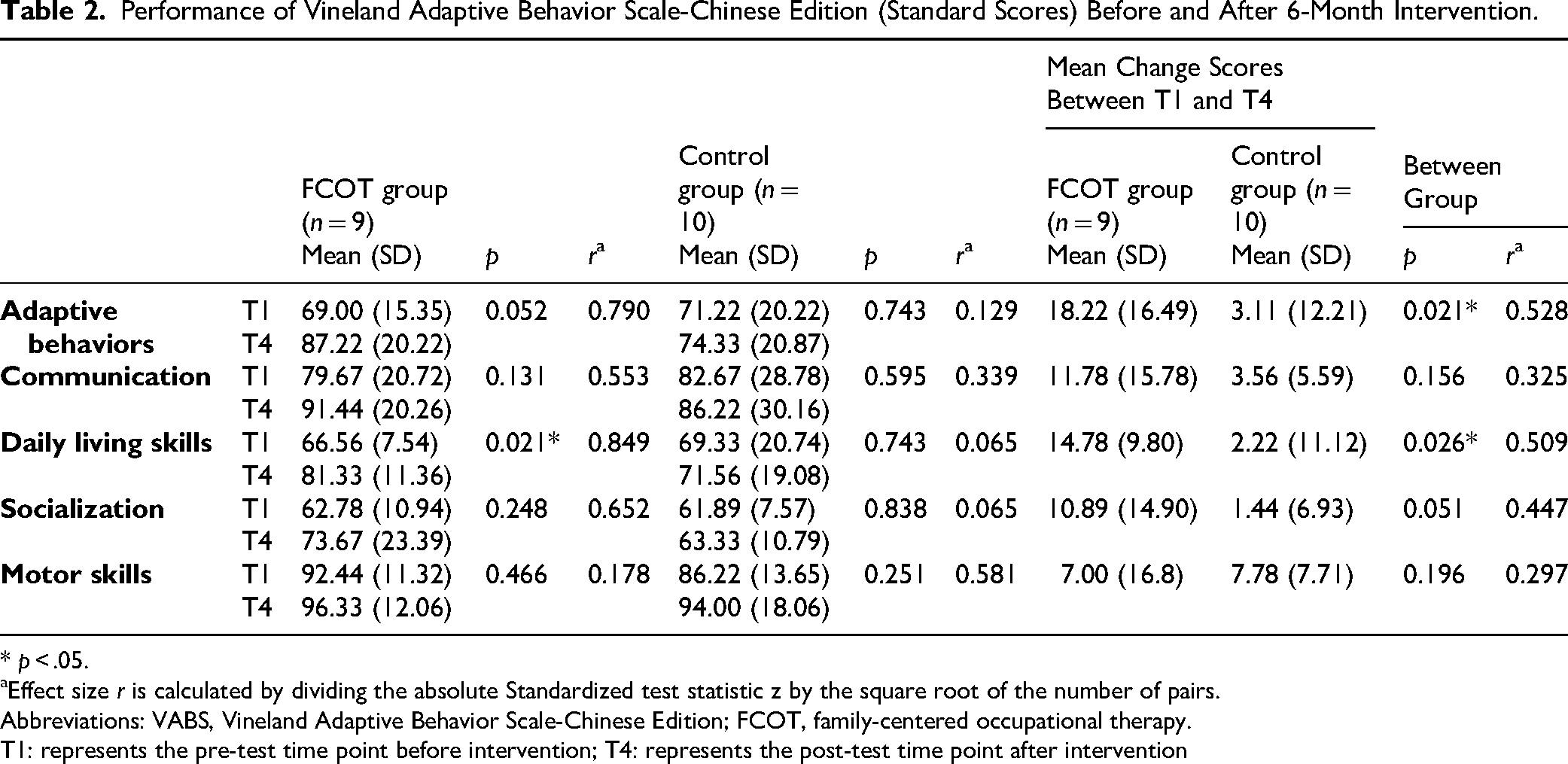
Children in the FCOT group showed significant within-group gains in daily living skills (p = .021) and marginal improvement in total Adaptive Behavior (p = .052). The control group showed no significant within-group changes across all areas (Table 2).
Performance of Vineland Adaptive Behavior Scale-Chinese Edition (Standard Scores) Before and After 6-Month Intervention.
* p < .05.
Effect size r is calculated by dividing the absolute Standardized test statistic z by the square root of the number of pairs.
Abbreviations: VABS, Vineland Adaptive Behavior Scale-Chinese Edition; FCOT, family-centered occupational therapy.
T1: represents the pre-test time point before intervention; T4: represents the post-test time point after intervention
Between-group comparisons indicated that FCOT significantly outperformed the control group in adaptive behavior (p = .021) and daily living skills (p = .026), with socialization approaching significance (p = .051) (Table 2).
RKPPS Results
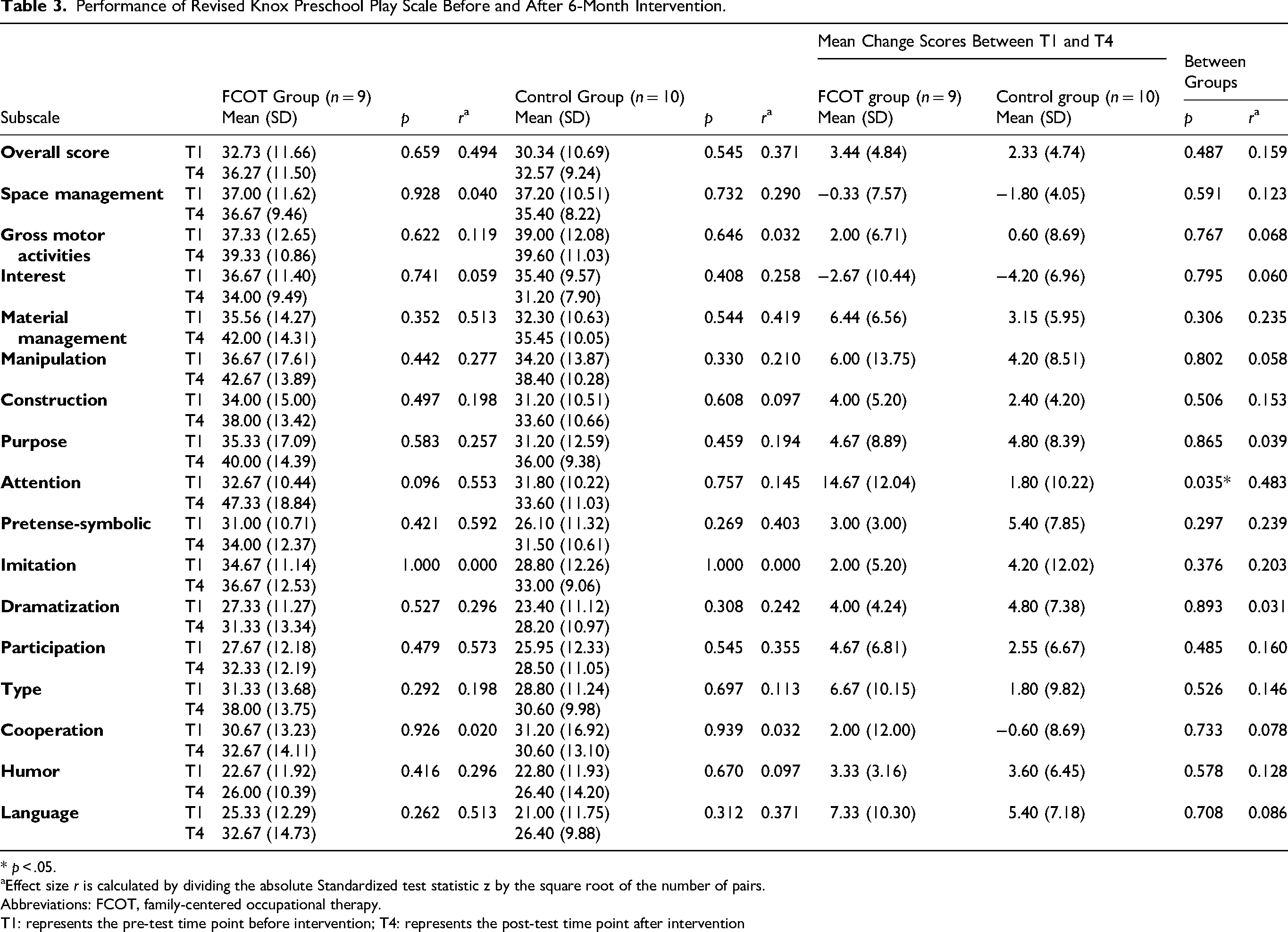
No significant within-group changes were found across four dimensions or 12 play behaviors. However, the FCOT group demonstrated moderate-to-large within-group effect sizes in overall score, the dimensions of material management, pretense-symbolic, participation, and play behaviors of attention and language. The control group showed similar within-group effects except for attention, which was small (Table 3). Between-group differences were non-significant, except for attention, which significantly favored FCOT (p = .035) (Table 3).
Performance of Revised Knox Preschool Play Scale Before and After 6-Month Intervention.
* p < .05.
Effect size r is calculated by dividing the absolute Standardized test statistic z by the square root of the number of pairs.
Abbreviations: FCOT, family-centered occupational therapy.
T1: represents the pre-test time point before intervention; T4: represents the post-test time point after intervention
Goal Attainment Scaling Outcomes
Goal attainment scaling outcomes were assessed only in the FCOT group. Within-group improvements were observed for both daily activity and play goals. Daily activity goals improved significantly at 3 months (median = 50.00; CI: 44.56–55.44; p = .008) and from 3 to 6 months (median = 60.00; CI: 52.31–67.69; p = .008). Play goals also showed significant gains at 3 months (median = 55.00; CI: 47.26–62.74; p = .004) and from 3 to 6 months (median = 50.00; CI: 46.09–61.41; p = .004). After 6 months of intervention, two children had one goal each that was not achieved, whereas the remaining seven children met all three goals. For the unmet goals, the therapist discussed potential contributing factors with the parents. Since the 6-month intervention period had ended, no further intervention was provided.
Results of PSI-SF and FOS-R
No significant within-group post-intervention changes were observed in parental stress for either group. Similarly, within-group family outcomes did not differ significantly although moderate-to-large effect sizes were noted, particularly for “Know rights” and “Help child develop and learn,” favoring the FCOT group. Between-group differences were non-significant.
Discussion
EI services in Taiwan are predominantly delivered in hospital outpatient settings under the National Health Insurance system. Despite substantial public investment, empirical evidence regarding the effectiveness of hospital-based family-centered interventions remains limited. This study evaluated a hospital-based FCOT Coaching Intervention for autistic children. The findings suggest that the intervention is feasible within hospital-based EI settings and may support improvements in children's participation and parent-identified goals in daily activities and play.
Intervention Rationale and Distinct Contribution
The FCOT Coaching Intervention was informed by Rush and Shelden's (2011) coaching framework and adapted for delivery within hospital-based EI settings. Consistent with OPC, the FCOT Coaching Intervention emphasizes enhancing children's participation in daily activities through caregiver coaching, which may explain the observed improvements in participation outcomes (Graham et al., 2009, 2010, 2024).
A key distinguishing feature of FCOT Coaching Intervention, compared with OPC, is the integration of coaching with in-session, occupation-based demonstration. This design aligns with parent-mediated interventions such as Project ImPACT and the Early Start Denver Model, which combine therapist modeling with guided caregiver practice to support skill acquisition and generalization to everyday routines (Ingersoll & Dvortcsak, 2019; Rogers & Dawson, 2010). However, these interventions typically require higher intensity and longer session durations, which may be less feasible within Taiwan's National Health Insurance–funded EI services.
In addition, whereas OPC, Project ImPACT, and ESDM primarily focus on one-to-one parent–child interactions, the FCOT Coaching Intervention incorporates small-group play opportunities alongside individualized parent coaching. This feature may be particularly relevant for children with autism, whose participation challenges often emerge in peer contexts. By observing therapist-facilitated social interactions and practicing strategies through coaching, caregivers may be better supported to apply these strategies in naturalistic settings.
Taken together, these findings suggest that integrating occupation-based therapist demonstration with caregiver coaching may represent a feasible and contextually appropriate adaptation of coaching-informed interventions for hospital-based EI settings. Future research should further examine the mechanisms and effectiveness of this combined approach.
Child Outcomes: Adaptive Behavior, Daily Living Skills, and Play Participation
Children receiving the FCOT Coaching Intervention showed significant improvements in Daily Living Skills and Adaptive Behavior, outperformed the control group, and demonstrated a trend toward improved Socialization. Consistent with previous participation-focused coaching interventions (Chiu & Tseng, 2020; Graham et al., 2010; Little et al., 2018), these findings support the role of caregiver coaching in enhancing children's functional participation in daily routines. Importantly, our findings extend prior literature by demonstrating that such participation gains can be achieved within hospital-based EI settings, where service intensity is often constrained.
In play outcomes, most RKPPS dimensions and behaviors did not show statistically significant within-group change; however, the FCOT group demonstrated moderate-to-large effect sizes across several domains, with a significant between-group advantage in attention during play. Sustained attention to object during play has received limited empirical attention in ASD. Previous studies indicate that children with ASD often remain unengaged and require adult facilitation to sustain interaction with objects or people (Wong & Kasari, 2012). The FCOT Coaching Intervention emphasizes in-session structured play demonstration and guided caregiver practice, which may enhance children's attentional engagement by supporting caregivers in providing timely cues and scaffolding during play. This interpretation is consistent with evidence showing that parent attentional cues can influence sustained attention in young children with ASD (Brigham et al., 2009).
Compared with prior coaching interventions that primarily target one-to-one parent–child interactions, the inclusion of therapist-modeled play and opportunities for observing peer interaction in FCOT may offer an additional mechanism for supporting engagement in socially complex contexts. This feature may be particularly relevant because participation challenges in autism often emerge in peer-based situations rather than isolated dyadic interactions.
These findings have important clinical implications. First, they suggest that integrating coaching with therapist demonstration may enhance participation outcomes by bridging the gap between strategy learning and real-time application. Second, the results highlight attention during play as a potentially sensitive and meaningful outcome for evaluating participation-focused interventions in ASD. Third, the feasibility of implementing FCOT within hospital-based services suggests that coaching-informed, participation-focused interventions can be adapted to settings with limited intensity.
Future research should further examine the mechanisms through which caregiver coaching and therapist demonstration jointly influence children's engagement and participation outcomes.
In contrast, PEP-3 outcomes did not show statistically significant within- or between-group differences. Nevertheless, the FCOT group demonstrated moderate-to-large within-group effect sizes for Communication, Maladaptive Behaviors, and several subtests (e.g., Cognitive Verbal/Preverbal, Expressive Language, Visual–Motor Imitation, Social Reciprocity, and Characteristic Verbal Behaviors). Taken together, these results may indicate promising developmental change signals that were not detectable as statistically significant in a small sample, suggesting the need for adequately powered studies and longer follow-up to clarify developmental effects.
Goal Attainment: Clinically Meaningful Change in Family-Prioritized Participation
Goal Attainment Scaling (GAS) outcomes within the FCOT group showed robust improvements for both daily activity and play goals at 3 months and continued gains from 3 to 6 months. By 6 months, most children met all goals, with only two children having one unmet goal each. This pattern is consistent with prior research using goal attainment scaling as an outcome measure to capture meaningful, family-prioritized changes in participation among young children with autism spectrum disorder (Little et al., 2018). The findings strengthen the clinical interpretability of the standardized outcomes by demonstrating change in family-prioritized participation targets. They also align with the intervention's RTSS-specified emphasis on caregiver-mediated strategy use within daily routines and play.
Family Outcomes: Stress and Broader Family Functioning
Parental stress (PSI-SF) did not change significantly in either group. Similarly, FOS-R scores did not show statistically significant within- or between-group differences, although moderate-to-large effect sizes were observed in domains such as “Know rights” and “Help child develop and learn,” favoring FCOT. Persistent caregiver stress despite child participation gains is consistent with prior literature (Kuhaneck et al., 2015; Oono et al., 2013) and may reflect ongoing caregiving demands and contextual stressors. These findings suggest that FCOT alone may be insufficient to shift broader family well-being outcomes in the short term and support integrating additional psychosocial or care-coordination components (e.g., social work, mental health support, service navigation) to amplify family-level impact.
Considerations for Interpretation
Interpretation should consider differences in service exposure: both groups received similar amounts of occupational therapy; however, the control group received significantly more other therapies (e.g., applied behavior analysis, play therapy) during the study. Although baseline child measures were comparable, unequal concurrent intervention intensity may have diluted between-group contrasts on some outcomes. Future trials should consider controlling for, matching, or statistically adjusting for co-interventions and total therapy dose, and should recruit larger samples to improve power for detecting differences across developmental and family outcomes.
Study Limitations
This study has several limitations. First, the small sample size (n = 19; 9 in the FCOT group and 10 in the control group) limits statistical power and generalizability. Second, group assignment was non-randomized and based on parental convenience, which introduced potential selection bias. Third, the control group received usual therapies, but only total weekly hours were recorded, and details on treatment content and caregiver involvement were largely unavailable, limiting between-group comparability. Future research should employ randomized designs, larger samples, and tighter control of external interventions.
Long-term follow-up is also needed to determine whether FCOT outcomes are sustained. Although child outcomes improved, parenting stress and family outcomes showed no significant changes, consistent with prior evidence suggesting that caregiver stress reduction requires broader supports such as financial aid, respite care, and mental health services (Kuhaneck et al., 2015; Rogers & Vismara, 2008).
Implications for Occupational Therapy Practice
This study suggests that FCOT with parent coaching may be a feasible approach for supporting participation in daily activities and play among young autistic children in hospital-based EI.
FCOT with parent coaching may support children's participation in daily activities and play. Integrating caregiver coaching with occupation-based therapist demonstration may help caregivers apply strategies in everyday routines. Participation-focused goals in daily activities and play may be appropriate targets for occupational therapy intervention.
Conclusion
FCOT with parent coaching led to significant improvements in adaptive behaviors, daily living skills, and attention during play among autistic children in a hospital-based setting. Although no significant changes were observed in family outcomes, positive trends suggest potential broader benefits with sustained or expanded support. These findings underscore the value of implementing FCOT more widely and highlight the need for further research on its long-term effectiveness and scalability.
Supplemental Material
sj-pdf-1-aot-10.1177_19437676261464088 - Supplemental material for Enhancing Play and Daily Activities in Autistic Children: Family-Centered Occupational Therapy in a Hospital Setting
Supplemental material, sj-pdf-1-aot-10.1177_19437676261464088 for Enhancing Play and Daily Activities in Autistic Children: Family-Centered Occupational Therapy in a Hospital Setting by Ya-Lin Hsieh, Mei-Hui Tseng, Fu-Mei Chiang, Wei-Tian Huang, Wen-Hsin Lai and I-Ming Hsiao in American Journal of Occupational Therapy
Supplemental Material
sj-pdf-2-aot-10.1177_19437676261464088 - Supplemental material for Enhancing Play and Daily Activities in Autistic Children: Family-Centered Occupational Therapy in a Hospital Setting
Supplemental material, sj-pdf-2-aot-10.1177_19437676261464088 for Enhancing Play and Daily Activities in Autistic Children: Family-Centered Occupational Therapy in a Hospital Setting by Ya-Lin Hsieh, Mei-Hui Tseng, Fu-Mei Chiang, Wei-Tian Huang, Wen-Hsin Lai and I-Ming Hsiao in American Journal of Occupational Therapy
Footnotes
Acknowledgments
We sincerely thank the participating parents and children. This work was supported by the National Taiwan University Hospital. We also appreciate the expert assistance of the NTUH Statistical Consulting Unit.
ChatGPT (OpenAI, 2025) was used solely for grammar editing; all content was reviewed and approved by the authors.
Ethical Approval
The ethical approval was granted by the ethical committee of the National Taiwan University Hospital.
Funding
This study was partly funded by National Taiwan University Hospital.
National Taiwan University Hospital, (grant number 105-003293).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.