
Abstract
Introduction. Guidewire entrapment with an inferior vena cava (IVC) filter during internal jugular vein central line placement is a rare complication. The diagnosis is made by abdominal X-ray or fluoroscopy, and in the majority of cases, the guidewire is removed by interventional radiology, seldom requiring operative removal. Objective. To describe a case of diagnosing central line guidewire entrapment with an IVC by bedside ultrasound. Data source/Case summary. During the placement of a central venous catheter (CVC) in a 63-year-old man—on postoperative day 7 from small bowel resection with presumed peripherally inserted central catheter sepsis—the authors were unable to remove the guidewire. Bedside ultrasound was used to quickly identify the guidewire entrapment down the IVC to the IVC filter. Conclusion. Bedside ultrasound may aid in the diagnosis and expedite the management of guidewire entrapment with IVC filter, which is on the CVC placement complications.
“With the increasing incidence of CVC [central venous catheter] and IVC [inferior vena cava] filter placements, reporting the occurrence of guidewire entrapment has increased.
Guidewire entrapment with inferior vena cava (IVC) filter is one of the rare complications that have been reported in the literature during CVC placement, pulmonary artery catheter placement, or during various intravascular interventional procedures.1-4 In US hospitals, millions of central venous catheters (CVCs) are inserted yearly with reported complications ranging from 5% to 19%. 5 Every year about 30 000 IVC filters are placed in the United States, when anticoagulation is contraindicated or for occurrence or recurrence of a pulmonary embolus (PE) even in presence of anticoagulation.6,7 With the increasing incidence of CVC and IVC filter placements, reporting the occurrence of guidewire entrapment has increased.8,9 We report a case of guidewire entrapment in an IVC filter during CVC placement and describe how bedside ultrasound aided in the diagnosis and prompted timely intervention.
Case Summary
A 63-year-old man—on postoperative day 7 from small bowel resection, gastric feeding tube placement, and incisional hernia repair with a mesh placement—was transferred to the surgical intensive care unit (SICU) for a presumed peripherally inserted central catheter (PICC) line sepsis. Past medical and surgical history included the following: bilateral lower extremity deep vein thrombosis, atrial fibrillation, IVC filter placement for high risk of PE, superior mesenteric artery embolization complicated by small bowel ischemia and bowel resection. Following his arrival in SICU, blood cultures from peripheral and PICC line were obtained and the PICC line was removed. Placement of a CVC was attempted for hemodynamic monitoring, vascular access, and parenteral nutrition. Under ultrasound guidance, a new left internal jugular vein (IJV) central line placement was attempted. The procedure was done by the SICU resident under supervision using a linear array probe 12 MHz and a curvilinear array probe (z.one ultra system, ZONARE Medical Systems, Mountain View, CA) to identify the left IJV before starting the procedure. Under sterile technique, the introducer needle was inserted in left IJV and the guidewire was passed beyond 25 cm marker from the skin level. The patient experienced a short episode of ventricular tachycardia and the operator pulled the guidewire back slightly resulting in return to normal sinus rhythm. The guidewire was slightly advanced a few centimeters with the sterile seldinger technique for vein dilatation followed by placement of the CVC. Near completion of the procedure, attempts to pull back the guidewire were unsuccessful even after rotation and j-wire straightening techniques. Without any further attempts to pull the guidewire, a curvilinear array transducer was placed in subxipoid area to possibly locate the guidewire intra-atrially or intraventricularly. Neither the guidewire nor any pericardial effusion was seen. On positioning the transducer along the right anterior axillary line between the sixth and eighth intercoastal spaces, a guidewire artifact was identified within the IVC. Further scanning of the IVC caudally identified the IVC filter along with the guidewire (Figures 1 and 2).
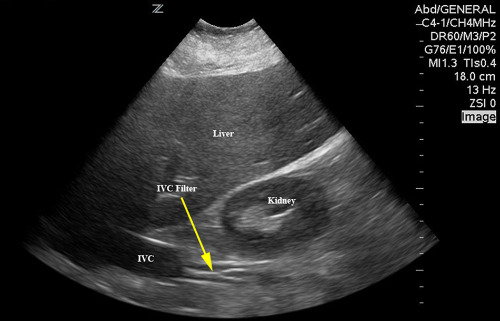
Ultrasound image showing IVC filter in inferior.
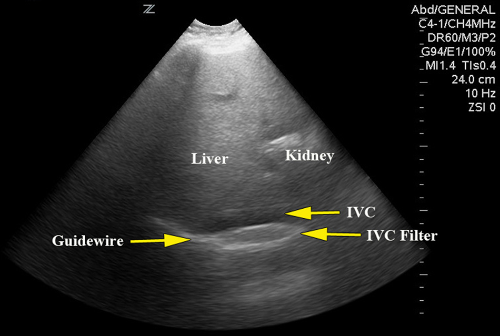
Ultrasound imaging showing guidewire entrapment with IVC filter.
The patient was sent to the interventional radiology suite without delay prior to any radiographic confirmation. Under fluoroscopy, entrapment of guidewire with IVC filter (Figure 3) was confirmed and successfully removed with only a few episodes of ventricular tachycardia without hemodynamic compromise. A new CVC was placed in the left IJV while the patient was in interventional radiology suite, and the IVC filter was left intact in place.
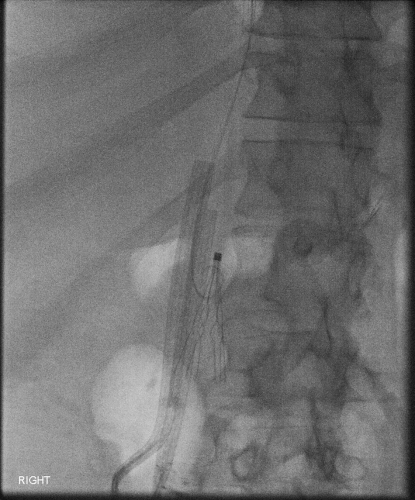
Fluoroscopy image showing guidewire entrapment.
Discussion
Using ultrasound during central line placement is the standard of care in many institutions to ensure patient safety and to reduce the number of attempts and complications.10-13 To date, no published report has described the use of bedside ultrasound in identifying guidewire entrapment to an IVC filter during CVC placement. From various prior case series and reports, the diagnosis of guidewire entrapment is done by obtaining a chest/abdominal X-ray and once confirmed, the patient underwent guidewire removal by interventional radiology or in rare cases, by vascular surgery. 4
In our case report, the ICU resident was unaware of the presence of an IVC filter during CVC placement and the guidewire was inserted beyond 25 cm from the skin level. Likely the guidewire entered the right atrium and then right ventricle temporarily and the patient experienced ventricular tachycardia. To change to sinus rhythm, the guidewire was pulled back by few centimeters, that is, from right ventricle to the superior vena cava (SVC). Inadvertently, the resident again advanced the guidewire by few more centimeters, which might have resulted in the guidewire changing its route from the SVC to the IVC. This led to entrapment within the IVC filter that was located at T12/L1 vertebral junction. During CVC placement, it is recommended that the guidewire not be placed more than 20 cm from the skin level to avoid arrhythmias or other rare complications.
The advantage of bedside ultrasonography is the immediate availability and nonradiating imaging to identify cardiac structures, intrathoracic and intra-abdominal vasculature prior to and during placement of CVC. Killu et al 14 have described the identification of CVC artifact within the SVC as confirmation of proper CVC placement. Vezzani et al, 15 in a prospective diagnostic study, demonstrated that the sensitivity and specificity of ultrasound detection of catheter misplacement could be as high as 96% and 93%, respectively. Postprocedural sonographic lung assessment for detection of occult pneumothorax and prompt placement identification has been described in the field of emergency medicine and critical care medicine.14,15 Routinely, a chest X-ray is performed immediately after the procedure and it is possible to miss small volume pneumothorax or pneumothorax over posterior or medial locations. Ultrasound is found to be superior in diagnosing even small volume pneumothorax when compared with chest X-ray. The other benefits of postprocedural ultrasound are reduction in lead time for diagnosing pneumothorax, 15 radiation exposure, and also cost burden.
The differential diagnosis of a trapped guidewire includes not only IVC filter entrapment but also entrapment in sternocleidomastoid muscle or deep tissue if introducer needle pierces the posterior wall of IJV. Cardiac valve entrapment (tricuspid valve), knotting of the guidewire, and kinking of the guidewire where it cannot be pulled back from the catheter has been reported.5,16
By performing a bedside ultrasound in a systematic way, one can possibly identify the location of the guidewire entrapment. We propose tracing the guidewire with a linear or microconvex probe from point of skin entry, visualizing the wire in the IJV, and confirming the wire coursing toward the SVC. Placing phased probe over the subxiphoid area will help identify guidewire location inside the cardia, that is, either in right atrium, right ventricle, or entanglement with tricuspid valve or in IVC. Finally, placing a phased array or a curvilinear probe over right sixth/seventh or eighth intercostal spaces at the anterior axillary line pointing toward left may help visualize the IVC. Usually, IVC filters are placed above or below the junction of the IVC and the right renal vein.
Conclusion
Literature describes bedside ultrasound for the diagnosis and expedited management of CVC placement complication such as vascular injury or pneumothorax. We described how ultrasound expedited the identification and timely treatment of an entrapped guidewire to an IVC filter.
Footnotes
The author(s) declare no potential conflicts of interest with respect to the authorship and/or publication of this article.