
Abstract
Patients with acute lung injury or acute respiratory distress syndrome present many challenges in the perioperative setting. Maintaining oxygenation and hemodynamic stability requires a comprehensive plan for both transport and intraoperative management. Many factors are important to consider when choosing a mechanical ventilation strategy, including tidal volume, ventilation mode, and maintenance of positive end-expiratory pressure. The goals of care include maintenance of lung protective strategies during surgery and avoidance of adverse events during transport. Considerations for ventilation unique to the intraoperative setting and situations requiring use of a transport ventilator or an ICU ventilator are discussed. Overall, providing safe and high-quality perioperative care to a critically ill patient requires communication and collaboration among a multidisciplinary team.
Keywords
“The physiologic derangements resulting from critical illness have implications on all aspects of perioperative care, including transport, intraoperative management, and postoperative stabilization.”
Critically ill patients frequently require surgical intervention for a variety of indications. Common examples include trauma, burns, abdominal compartment syndrome, sepsis, acute hemorrhage, and obstetric emergencies. Many of these problems carry an association with acute lung injury (ALI) or acute respiratory distress syndrome (ARDS). The physiologic derangements resulting from critical illness have implications on all aspects of perioperative care, including transport, intraoperative management, and postoperative stabilization. All members of the health care team, including intensivists, anesthesia providers, surgeons, respiratory therapists, and nursing staff must be familiar with the unique challenges associated with the perioperative care of the critically ill patient with ALI/ARDS.
This review will focus on the perioperative care of mechanically ventilated patients with ALI and ARDS. We will discuss specific considerations for management of ventilation in the operating room (OR), summarize the distinct features of both anesthesia and ICU ventilators, and address factors important to the care of mechanically ventilated patients during transport and while under anesthesia.
Considerations for Ventilating Critically Ill Patients in the Operating Room
Critically ill patients on advanced ventilator settings present unique challenges in the intraoperative period. These patients, who may already have ARDS or ALI or may be at risk for developing ALI/ARDS, commonly start with marginal oxygenation, which may worsen during surgery and anesthesia because of the many dynamic changes that occur in the OR. Important factors to consider when determining an intraoperative ventilation strategy are summarized in Table 1.
Considerations for Intraoperative Mechanical Ventilatory Support in Patients With Acute Respiratory Failure

Abbreviations: FRC, functional residual capacity; VT, tidal volume; ARDS, acute respiratory distress syndrome; ALI, acute lung injury; Fio2, fraction of inspired oxygen; PEEP, positive end-expiratory pressure; ECMO, extracorporeal membrane oxygenation; PVR, pulmonary vascular resistance; RV, right ventricular; LV, left ventricular; CO, cardiac output; BP, blood pressure.
Respiratory Effects of General Anesthesia
General anesthesia has predictable effects on the respiratory system. Patients with normal pulmonary function experience decreased oxygenation on induction of anesthesia that returns to normal within 2 hours after minimally invasive surgery but may last up to 2 weeks in patients undergoing upper abdominal or intrathoracic surgery. 1 Induction of anesthesia in a supine patient causes a 15% to 20% reduction in functional residual capacity, 2 which results primarily from loss of diaphragmatic and respiratory muscle tone. Ventilation perfusion (V/Q) mismatch results from the consequent dependent lung atelectasis,3,4 resorption atelectasis with the use of high fraction of inspired oxygen (Fio2), 5 and the effect of inhalational anesthetics, which inhibit hypoxic pulmonary vasoconstriction. 6 It is estimated that shunt fraction (Qs/Qt) increases by 0.1 to 0.15 during anesthesia in healthy patients,7(pp350-378) but more drastic changes may occur in patients with pulmonary disease as perfusion to heterogeneous lung increases. One retrospective study showed that Pao2/Fio2 decreased by an average of 63 mm Hg when patients requiring preoperative mechanical ventilation (MV) for respiratory failure underwent general anesthesia. 1
Lung Protective Ventilation
Data from animal studies suggests that MV with higher tidal volume (VT) causes lung injury and inflammation, 8 but whether it is the MV itself or the tidal volume size that initiates the process is an ongoing debate.9,10 Even in patients with normal lungs, MV has been associated with increases in inflammatory mediators in serum and bronchoalveolar lavage fluid regardless of size of VT, 9 but the use of low tidal volume attenuates the inflammatory response.9,10 However, the increase in inflammatory mediators alone has not correlated with worsened clinical outcomes in patients with normal lungs,9,10 suggesting that insults in addition to MV are required for progression to ALI.
The prevalence of ARDS and ALI approximates 9% among all ICU patients and 37% among mechanically ventilated patients. 11 Mortality in this population when traditional tidal volumes (10-15 cm3/kg) are used is 40% to 50%. 11 The landmark study from the Acute Respiratory Distress Syndrome Network (ARDSnet) in which patients with ALI were randomized to traditional (12 cm3/kg and plateau pressure <50 cm H2O) or low (6 cm3/kg and plateau pressure <30 cm H2O) VT demonstrated decreased mortality and increased ventilator-free days in patients treated with the low VT strategy, or lung protective ventilation. 8 In addition, serum interleukin-6 levels decreased more in the low VT group, suggesting improvement in lung inflammation. 8 Maintenance of low tidal volume ventilation with reasonable oxygenation (Pao2 55-80, Sao2 > 88% to 95%) 12 is the key strategy of the ARDSnet protocol, because outcome in the ARDSnet study was not dependent on oxygenation. 8 A recent Cochrane review of 6 studies involving 1297 patients showed a relative risk of 0.74 for 28-day mortality in patients with ARDS treated with lung protective ventilation. 11 Because surgical issues such as trauma, burns, pancreatitis, and intra-abdominal sepsis have a strong association with ARDS, patients requiring lung protective ventilation are commonly seen in the OR.
Oxygenation
Increasing Fio2 and applying positive end-expiratory pressure (PEEP) are traditional approaches that improve oxygenation in mechanically ventilated patients. PEEP recruits collapsed lung and prevents atelectasis, which improves V/Q matching 13 and helps to mitigate ventilator induced lung injury by preventing repeated opening and closing of alveoli.9,10 Excessive PEEP, however, may worsen oxygenation by causing regional overdistension, thereby increasing V/Q mismatch by redistributing perfusion to low V/Q units. 13 ARDS progresses through several phases, characterized early on by increased capillary permeability and accumulation of fluid in the alveoli, followed by cellular proliferation and deposition of matrix components, and culminating with either slow resolution or further fibrosis over weeks to months. Because ARDS is a dynamic process, PEEP may have variable effects on lung recruitment, oxygenation, and lung protection at later disease phases. Neuromuscular blockade, pulmonary vasodilators, prone positioning, extracorporeal membrane oxygenation, and advanced ventilator settings [e.g., airway pressure release ventilation (APRV) and high-frequency oscillatory ventilation (HFOV)] are additional treatments used in patients with severely compromised oxygenation.
A recruitment maneuver is a ventilatory strategy used to open collapsed lung. Recruitment maneuvers have been shown to increase oxygenation and lung compliance and to reduce alveolar dead space. 14 Recruitment maneuvers can take the form of intermittent high-pressure breaths (40 cm H2O for 30-40 seconds), “optimal” levels of PEEP (the PEEP required to prevent atelectasis in an individual patient), large VT breaths set at regular intervals (sigh breaths), or a combination of the above.15,16 The most effective recruitment maneuver is a matter of debate, but two recent prospective studies showed that a combination of sigh breaths and high PEEP is most effective at improving and sustaining oxygenation and lung compliance.15,16
Lung and Chest Wall Compliance
Acute lung injury and ARDS are diseases of low lung compliance caused by interstitial edema early in the disease process followed by repair and fibrosis in the later stages. 17 Other etiologies of respiratory failure, including pneumonia, pulmonary edema, and alveolar hemorrhage, are also characterized by low lung compliance. Regional variations in lung compliance caused by heterogeneously affected lung tissue, 17 in addition to dynamic changes in compliance occurring during surgery from patient positioning, fluid resuscitation, neuromuscular blockade, and surgical stimuli, can contribute to difficulty in maintaining adequate intraoperative oxygenation and ventilation.
Hemodynamic Implications of Ventilation
Ventilation strategy may have a significant impact on cardiovascular function. Hypercapnea and acidosis, which are acceptable consequences of lung protective ventilation, can lead to increased pulmonary vascular resistance and decreased cardiac contractility. 18 High PEEP can decrease venous return, right ventricular ejection fraction, and left ventricular preload leading to decreased cardiac output and blood pressure. Alternatively, PEEP can augment cardiac output in patients with ventricular dysfunction by offloading the left ventricle. 18 Tidal volume, however, does not seem to play as large a role in hemodynamic instability as other ventilator settings. Analysis of a subgroup of patients included in the ARDSnet study found no difference in hemodynamic function, vasopressor use, fluid administration, or diuretic therapy between patients ventilated with 6 or 12 cm3/kg VT. 18 Blood loss, insensible losses, and third spacing during surgery all contribute to the potential for hemodynamic variability, which may influence decisions related to volume resuscitation or the use of vasopressor drugs. These interventions in turn may further affect the respiratory system.
Fluid Management
A restrictive fluid management strategy increases ventilator free days and decreases ICU length of stay in patients with ARDS. 19 However, intraoperative fluid shifts and blood loss necessitate volume resuscitation and occasional blood transfusion, which may negatively affect oxygenation. Intraoperative fluid requirements had an inverse correlation with Pao2/Fio2 in a retrospective study of 145 patients requiring preoperative MV for respiratory failure who subsequently underwent surgery. 1 In a retrospective cohort study of patients who developed postoperative ARDS, the odds ratio for diagnosis of ARDS was 3.8 in those receiving intraoperative resuscitation >20 mL/kg/h and 2.4 in those receiving 10 to 20 mL/kg/h, compared with those receiving less than 10 mL/kg/h. 20 Blood product transfusion was not associated with development of ARDS in this study, 20 but has been linked to respiratory complications such as transfusion-related acute lung injury and transfusion-associated circulatory overload. 21
Patient Positioning
Surgery often requires changes in patient positioning to optimize surgical exposure and operating conditions. Positions such as prone, lateral decubitus, or Trendelenberg produce alterations in regional lung ventilation, perfusion, and compliance. These position changes have the potential to produce negative consequences on oxygenation; however, certain positions may improve respiratory parameters. For example, prone positioning improves lung oxygenation in patients with ARDS 22 as well as in the elective surgery population with minimal effect on respiratory compliance and Paco2. 23 The lateral position may have variable effects on the patient with nonuniformly affected lungs. Oxygenation worsens when the more affected lung is in the dependent position and improves when in the nondependent position. 24
Anesthesia Ventilators
Mechanical ventilation in the OR has changed dramatically over the past several decades as anesthetic and surgical techniques have gained complexity. Consequently, newer technology allows for performance of surgery and anesthesia on a sicker patient population. The first anesthetic delivery mechanisms were open systems limiting patients to spontaneous breathing. Reservoir bags were then developed to allow manual ventilation. A need for MV arose as use of neuromuscular blockade and opioids gained popularity. Anesthesia ventilators have since been increasing in complexity and now incorporate both controlled and assisted spontaneous breathing modes as standard features. 25 Continued improvement in ventilator technology is likely, as the current surgical atmosphere requires anesthesia ventilators with capabilities and ventilation modes similar to ICU ventilators.
Although anesthesia ventilators have become more sophisticated over time, many important differences exist when compared with ICU ventilators. Many anesthesia delivery systems cannot provide the high minute ventilation, increased airway pressures, flow characteristics, and PEEP needed to maintain oxygenation in patients with severe lung disease.13,26 Anesthesia ventilators are capable of delivering accurate VT in healthy lungs of average size, but the accuracy of VT delivery decreases at low VT or with low lung compliance. Anesthesia ventilators are double-circuit systems, where a conditioned gas within the bellows is compressed by a pressure regulated wall supply of gas. 26 During volume controlled ventilation, fresh gas flow increases VT, whereas the compliance of the bellows and circuit decrease VT.26-28 In addition, the limited flow capabilities of anesthesia ventilators cause delivery of reduced VT and minute ventilation at high respiratory rates and/or low lung compliance during volume- and pressure-controlled ventilation27,29,30 (Figure 1). Finally, the necessity for anesthesia ventilators to deliver inhaled anesthetics, scavenge exhaled gas, and allow for both ventilator-delivered and manually assisted breaths provides a challenge to design of improved systems.25,31
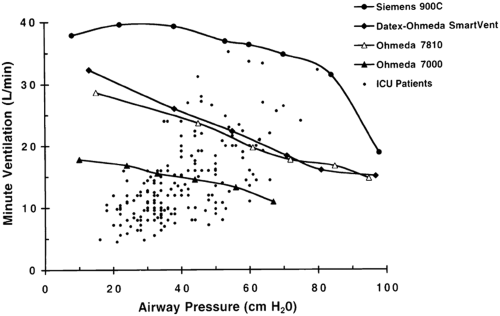
Calculated minute ventilation (VE) as a function of airway pressure at an inspiratory duty cycle (TI/TTOT) = 0.33. Superimposed are the preoperative VE and peak airway pressure values of 200 patients with acute respiratory failure requiring preoperative mechanical ventilation. Minute ventilation = mean inspiratory flow × inspiratory duty cycle.
More recently, anesthesia delivery systems that possess capabilities approaching ICU ventilators have been developed. 33 Compensation for both system compliance and fresh gas flow leads to more accurate VT delivery.27,28,31 Improved pressure and flow capabilities allow for delivery of increased minute ventilation and peak pressures, even in patients with low lung compliance. 32 The introduction of advanced breathing modes, such as pressure control with automatically adjusted flow rates to regulate volume, 29 and efficient spontaneous breathing modes 33 has greatly increased the versatility of anesthesia ventilators. A renewed interest in piston ventilators has arisen because of their ability to deliver accurate VT and improved inspiratory flow characteristics that facilitate advanced ventilation modes. 25
ICU Ventilators
In contrast to anesthesia ventilators, ICU ventilators are single-circuit systems, where gas from the wall supply is delivered directly to the patient at constantly regulated pressures. Minimal compressible volumes, precise servo-regulated valves, pressure-independent flow generators, and other characteristics that allow the delivery of high and variable inspiratory flow, peak pressures, minute ventilation, and PEEP also contribute to accuracy of VT delivery. 32
Advanced ventilation modes, including APRV and HFOV are occasionally used in patients with respiratory failure that have failed traditional MV. These modes take advantage of high mean airway pressure to prevent atelectasis and to maintain an open lung state, thereby improving oxygenation and preventing trauma from repeated alveolar opening and closing. 34 In APRV, patients are allowed to breathe spontaneously during a high continuous positive airway pressure (inspiratory) phase that alternates with a pressure release (low pressure or expiratory) phase. APRV has the advantage of allowing spontaneous ventilation through an active expiratory valve, which improves V/Q matching by preferentially directing gas flow to dependent lung regions34,35 and may decrease sedation requirements.13,36 Hemodynamic function is also improved as negative diaphragmatic pressure augments venous return and cardiac output.34,35 Small observational studies have shown decreased multiorgan failure and mortality, decreased peak airway pressures, improved cardiac index, decreased pulmonary vascular resistance, and decreased vasopressor and inotrope use with APRV in ARDS,37-39 although data from large randomized controlled trials supporting these benefits are not available. 34 HFOV is best studied in the neonatal population, but its use as a rescue modality is being revisited in adults. 34 HFOV is characterized by rapid oscillations of a piston-driven diaphragm, creating pressure differentials that result in small high frequency VT. Advantages include lack of alveolar overdistension and atelectasis; however, barotrauma and hemodynamic instability are concerns.34,36,40 Prospective randomized controlled trials comparing these ventilation modes to the current standard of care in lung protective ventilation have not been conducted, so their use is currently limited to situations where traditional MV has failed.
For some patients, only ICU ventilators possess the capabilities to maintain oxygenation and ventilation during a surgical procedure. Patients who have failed traditional MV in the ICU and require unique modes of ventilation such as APRV and HFOV should have these ventilation mode capabilities continued during transport and in the OR. Barriers to the use of ICU ventilators in the OR include inability to deliver volatile anesthetics, lack of ready availability, and lack of familiarity among some anesthesia providers.
Perioperative Management of the Critically Ill Patient
Taking a critically ill patient to the OR requires an interdisciplinary approach involving the patient’s intensive care team, anesthesia team, surgical team, respiratory therapists, and nursing staff. The potential for clinical decline exists throughout several stages, so care must be taken to formulate a plan with the goal of anticipating, preventing, and preparing for complications during each phase.
Transport
Prior to transport, the patient’s condition should be optimized in the ICU. Both the indication for transport and the feasibility of performing the procedure at bedside should be assessed.41,42 If the decision is made to transport the patient, an organized and systematic approach is necessary because critically ill patients are susceptible to a variety of adverse events (AEs) during transport (Table 2). Transport-related AEs most commonly fall into 4 broad categories: factors related to the patient, equipment, transport organization, or transport team. 41 Specific common AEs include hypotension, hypoxia, arrhythmia, cardiac arrest, extubation, difficulty with MV, undersedation, oxygen supply failure, electrical failure, and other equipment failure. 41 In addition, transport has been associated with increased risk of ventilator-associated pneumonia.13,41 Serious AEs, which threaten the life of the patient, have been reported to occur during 4% to 9% of transports. 41 The incidence of all AEs, including serious or otherwise, is up to 68%. 41 Transport-related AEs require intervention up to 80% of the time, 41 so the transport team must be adequately prepared with appropriate personnel, rescue drugs, airway equipment, and backup supplies in the case of equipment failure.
Recommendations for Transporting Critically Ill Patients
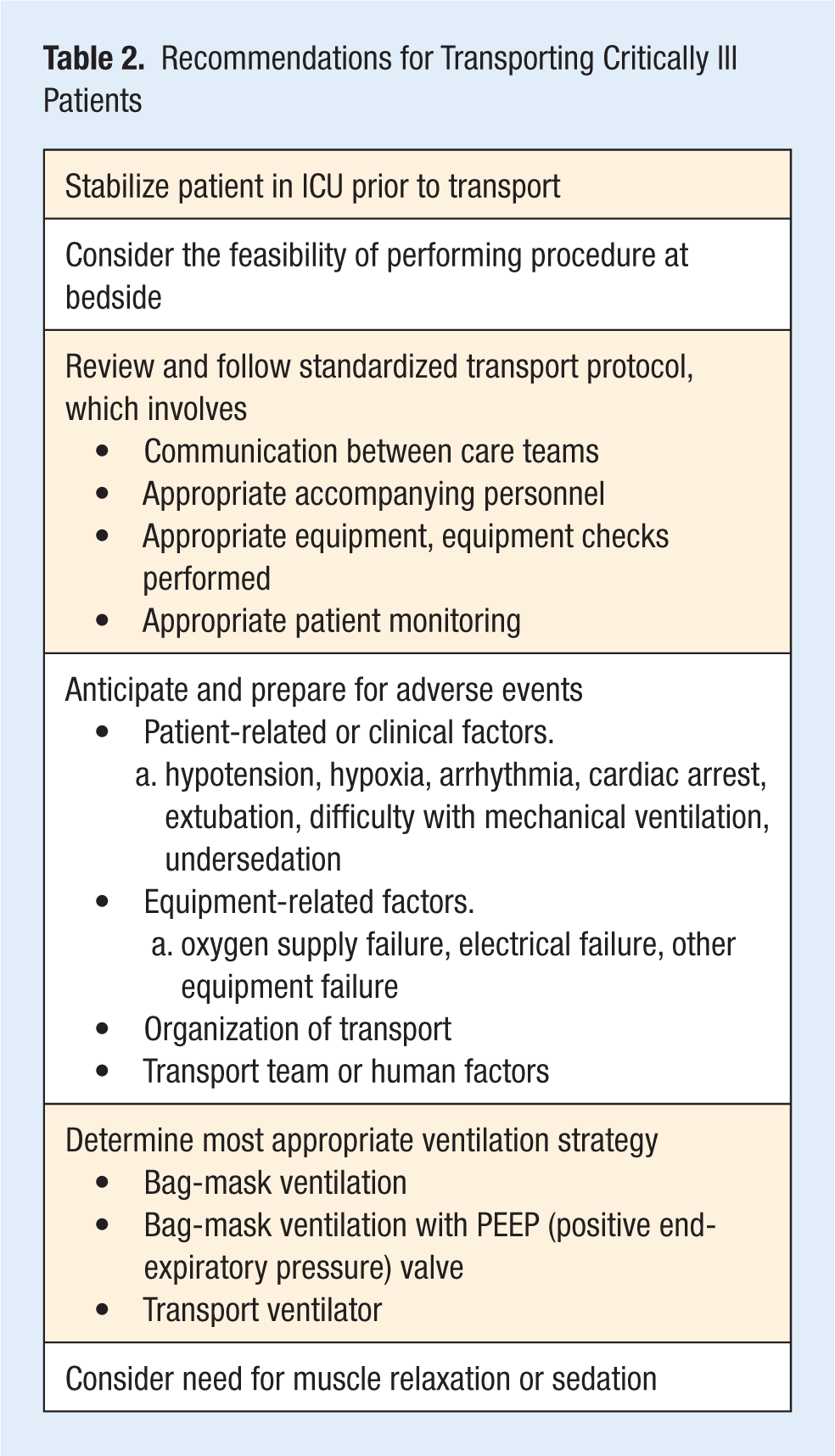
Guidelines from the American College of Critical Care Medicine and Society of Critical Care Medicine for the intrahospital transport of critically ill patients endorse the development of a standardized written institution-wide transfer plan. The plan, which may include checklists, should be strictly reviewed prior to transporting any patient. 42 The issues that must be addressed include coordination and communication between care teams, appropriate accompanying personnel, availability of appropriate equipment and check of functionality, and monitoring during transport. 42
In addition to the factors above, the plan for ventilation during transport warrants specific attention. Options include bag-mask ventilation (with or without a PEEP valve) or MV. One useful technique that may help inform providers about the need for a transport ventilator involves evaluation of the patient’s respiratory function, including oxygen saturation and end tidal CO2, and hemodynamic stability during a 5-minute trial of manual ventilation. Maintenance of respiratory and hemodynamic parameters during the trial period indicates that it is likely safe to proceed without a transport ventilator.
Although many transport ventilators do not work as efficiently as their ICU counterparts, 43 the use of transport ventilators has been shown to provide superior oxygenation, more consistent minute ventilation, 44 and improved regularity in the respiratory cycle when compared with manual ventilation. 45 In a study conducted on unprotected airways in the OR setting, bag-mask ventilation was associated with higher peak airway pressure, higher delta airway pressure, and lower oxygenation than occurred with resuscitation ventilators. 46 Occasional situations may arise when even a transport ventilator would not provide adequate respiratory support during transport, for example, when transporting a patient on an advanced ventilation mode. The transport team must consider several factors, including ventilator mode, FiO2, PEEP, minute ventilation, and inspiratory flow when deciding whether to use a transport ventilator or an ICU ventilator during transport. In addition, the need for sedatives and neuromuscular blockade should be considered in the ventilation plan.
Intraoperative Management
An important distinction exists between patients with preexisting ALI/ARDS and those at risk for developing ALI/ARDS. Both populations are commonly seen in the OR. Management principles are essentially the same for both patient groups, except that the focus of management in the former population includes both treatment and prevention of further injury, whereas in the latter involves primarily preventative strategies. Risk factors for development of ALI/ARDS include diseases such as sepsis, trauma, burns, pneumonia, and pancreatitis; toxin exposure; intraoperative volume resuscitation >20 mL/kg/hr20; and prior MV with high VT (>700 cm3), peak inspiratory pressure (PIP; >30 cm H2O), and PEEP (>5 cm H2O). 21 It is important to identify patients at risk for development of ALI/ARDS in order to employ preventative management, including use of lung protective ventilation and restrictive fluid strategies.
The OR anesthesia team must take many patient factors into account when caring for a critically ill patient with respiratory failure, including intraoperative ventilation, oxygenation, hemodynamic management, and anesthetic plan. 13 Maintaining oxygenation while avoiding additional lung injury should be the primary focus of the intraoperative ventilation strategy. 13 In a retrospective study of 145 patients requiring preoperative MV for respiratory failure and subsequently undergoing surgery, patients ventilated with an ICU ventilator intraoperatively had a nonsignificant but smaller increase in Qs/Qt (0.06 vs 0.08), a more rapid return to preoperative Pao2/Fio2, and required less PEEP postoperatively. 1 Although there are no specific guidelines directing the intraoperative use of an ICU ventilator, the need for additional support should be determined on a case-by-case basis after review of preoperative ventilatory requirements, including airway pressure, minute ventilation, and PEEP. Suggestions for intaoperative use of an ICU ventilator can be found in Table 3. Modern anesthesia ventilators with improved pressure and flow capabilities should be able to meet the ventilatory requirements of mechanically ventilated patients with PIPs approaching 60 cm H2O and minute ventilation up to 18 L/min. 32
Recommendations for Intraoperative Use of an ICU Ventilator
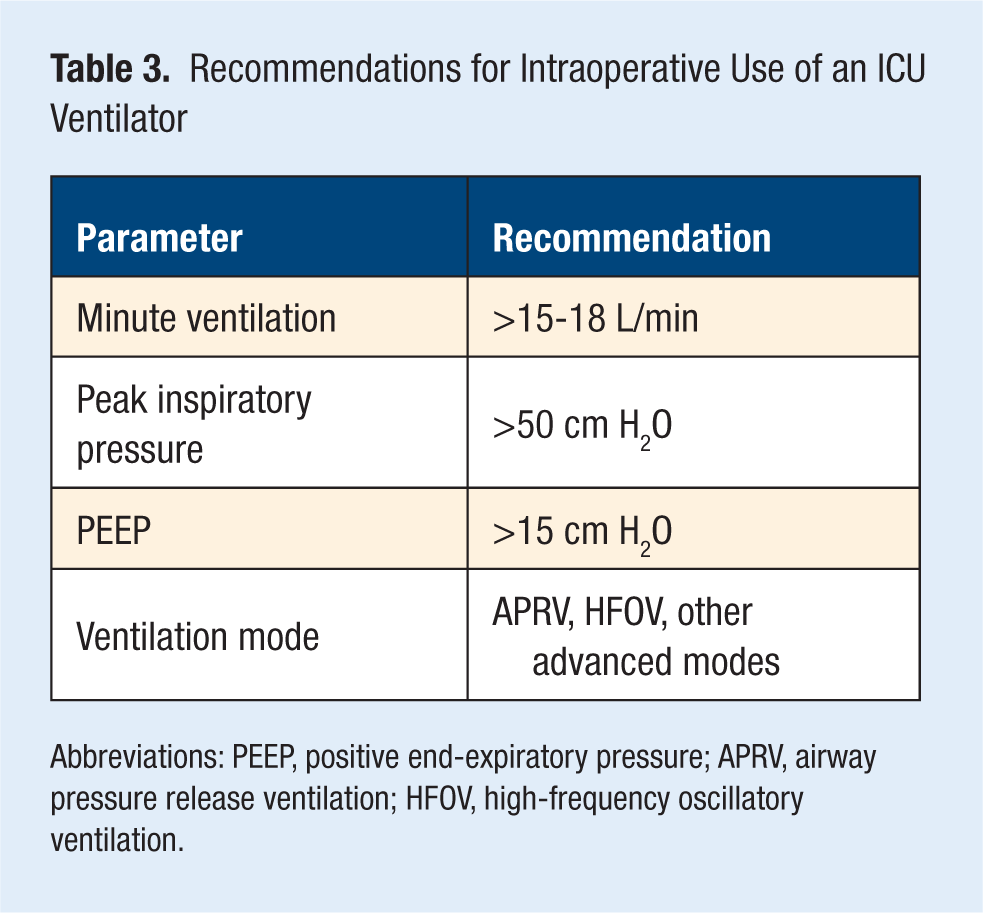
Abbreviations: PEEP, positive end-expiratory pressure; APRV, airway pressure release ventilation; HFOV, high-frequency oscillatory ventilation.
It has been demonstrated that typical management of intraoperative hypoxia involves increased Fio2 and PIP regardless of etiology. 47 A recent single-center retrospective study analyzing the intraoperative management of 1286 patients with a preoperative Pao2/Fio2 < 300 mm Hg showed that anesthesia providers tend to use increased Fio2, tolerate higher PIP, and employ lower PEEP than recommended by the ARDSnet guidelines. 48 In all patients studied, intraoperative FiO2, PIP, total VT, and VT in cm3/kg body weight were increased from preoperative settings during surgery, whereas PEEP was decreased from preoperative settings by small but statistically significant amounts. The same was true in the subset of patients with known ALI receiving VT < 7 cm3/kg preoperatively, although the change in VT and VT per kg body weight did not reach statistical significance. This suggests that typical intraoperative management may not involve strict application of ARDSnet recommendations in patients with known ALI. 90-day mortality was independently associated with intraoperative PEEP and PIP in a univariate analysis, although a cause and effect relationship was not clearly demonstrated.
Additional decisions facing the anesthesia team include the use of volatile anesthetic agents because of their effects on oxygenation, or neuromuscular blockade, which inhibits the patient’s ability to ventilate spontaneously. 13 The team must be adequately prepared for management of changes in hemodynamics and oxygenation and may consider placement of invasive monitors to assist in diagnosis of major intraoperative changes.
Conclusions
The care of the critically ill patient with respiratory failure presents a challenge in the perioperative period. A significant decline in the ability to oxygenate may occur intraoperatively because of multiple factors, including the expected respiratory effects of anesthesia, the need for lung protective ventilation, changes to lung and chest wall compliance, and intraoperative fluid resuscitation. Although anesthesia ventilators have improved significantly over the past several decades, they may not have the ability to provide adequate respiratory support to patients on advanced ventilator settings. Intraoperative use of an ICU ventilator may be necessary, but the inability to provide volatile anesthetic agents, lack of availability, and unfamiliarity among anesthesia providers represent drawbacks from the perspective of the anesthesia team. The possibility of adverse events occurring during transport of a critically ill patient may be minimized by following an organized plan that includes interdisciplinary communication, frequent equipment checks, close patient monitoring by appropriate personnel, and anticipation of the many problems which may occur. Intraoperative management requires the discretion of the anesthesia team and ends with postoperative stabilization and handoff in the ICU. The entire process involves a series of events that can only be accomplished safely through adequate preparation, communication, and teamwork.
Footnotes
Acknowledgements
The authors gratefully acknowledge the editorial assistance of Jeffrey A. Katz, MD.
Conflict of Interest: The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.