
Abstract
Although effective interprofessional collaboration is a key component of patient safety and quality improvement initiatives, little is known about the nature of collaboration in ICU settings. Through ethnographic research, this study will explore interprofessional care in 8 ICUs (6 based in the United States and 2 based in Canada), develop an empirically based readiness/diagnostic tool to assess the quality of team-based care delivery, and develop interventions to strengthen team-based care and patient family involvement. Our study has 3 iterative phases and will involve: a scoping review of the literature on team dynamics in the ICU, an ethnographic study (observation, shadowing, interviews) across 8 sites over 2 years and the collection of clinical outcomes data to inform the development of a “diagnostics” tool for interprofessional collaboration and family member involvement in ICU care, as well as interprofessional intervention development. The importance of ethnographic and other forms of qualitative research for the improvement of health care delivery has already been recognized. This study’s comparative design and the richness of its data have the potential to generate a multidimensional understanding of the processes of interprofessional collaboration and patient family member involvement. The creation of generally applicable, empirically grounded tools also has the potential to enhance these processes.
Keywords
“Intensive care is one area where effective inter-professional collaboration is most critical, given the severity of the cases . . .”
Background
The need for effective interprofessional care to reduce duplication of effort, restrict clinical error, improve safety, and enhance the quality of patient care is now widely acknowledged. 1 Intensive care is one area where effective interprofessional collaboration is most critical, given the severity of the cases and the quick and often unpredictable changes in patients’ conditions. Yet attempts to improve quality of care and patient safety have seen mixed results, possibly because of the absence of theory informed rapid cycling approaches of many quality improvement and patient safety initiatives.2,3 In response, several authors have asked deeper study and greater contextualization of health care delivery 4 through consideration of those cultural factors that affect care provision, encouraging greater use of qualitative research methods.5,6
This study will investigate how culture influences interprofessional collaboration and patient family involvement in the ICU. Using ethnography—a combination of observations, shadowing, formal and informal interviews understood to be one of the most powerful research methods to study culture7,8—we aim to better understand the factors that shape team-based care and patient family involvement on ICUs. To date, the few ethnographic studies that have sought to delve further into team dynamics have been undertaken at single sites, and have focused mostly on intraprofessional dynamics—typically within nursing, thus limiting the generalizable inferences that can be drawn from these studies. 9 Similarly, patients and their families have also been excluded from both research and interventions targeting teamwork. Exceptions are few and far between.10,11
Our study is informed by a framework developed by Reeves et al. 9 The framework invites researchers to pay attention to several determinants of interprofessional care: relational, processual, organizational, contextual (see Table 1).
Factors Influencing Interprofessional Teamwork
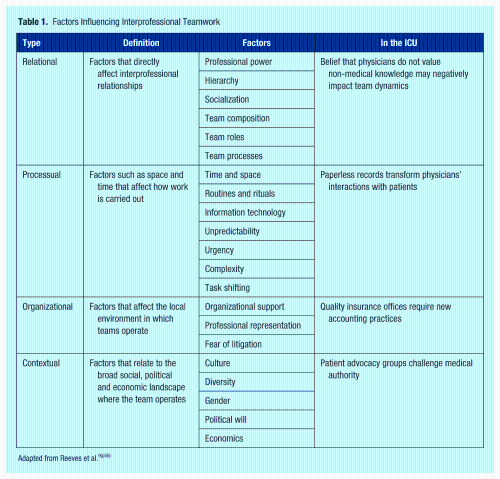
Adapted from Reeves et al.9(p58)
There are several advantages to starting with such a framework. Established theories are used explicitly to design the research questions, select and interpret relevant data, and propose explanations for observed phenomena. 12 Several authors have argued that very few patient safety or quality improvement interventions to date have outlined their theoretical underpinnings, or provided explicit rationales for how they might work.13 -15 In contrast, the present study will send its ethnographers into the field with a framework of sensitizing concepts to provide as clear an idea as possible about the links between culture, teamwork, and improved outcomes. 16 In this way the ethnographers will come to their differing study sites with expertise and concepts from their own discipline, ready to make sense of the realities they observe using this expertise as well as the local expertise of insiders in the field. 17 This conceptual framework builds on decades of research in interprofessional collaboration and will help orient data collection and facilitate comparative analysis across the 8 sites. 9 As such, it will help organize observations systematically, orienting the attention of ethnographers toward elements that previous research has shown to shape the nature and quality of interprofessional care.
Methods/Design
This project aims to overcome the current shortcomings in our knowledge of team interactions in the intensive care unit. It is focused on the following research aims:
To comprehensively explore, through the use of ethnographic methods, the team-based cultures of 8 ICUs: 6 in the United States and 2 in Canada;
Based on this rich descriptive work, identify an empirically based readiness/diagnostic tool that can provide an indication of whether optimal collaborative team-based care is being delivered;
Develop iteratively a set of scalable ICU interventional activities that focus on strengthening team-based care and patient family involvement in health care.
This study is divided into 3 main phases: (1) review of the literature; (2) data collection, including site identification, qualitative fieldwork, collection of clinical outcomes data, analysis and synthesis; and (3) instrument development. It is iterative in nature: Findings from earlier stages in the study will inform future steps, as is now considered best practice in qualitative research.8,18,19
Phase 1: Scoping Review
Phase 1 will consist of a scoping review of the literature on team dynamics in ICUs. Scoping reviews are intended to map the state of knowledge in a field through 5 stages: identifying the research question; identifying relevant studies; selecting studies; charting the data; and collating, summarizing, and reporting the data.20,21 To answer our research question (what do we know about team-based care in the ICU from ethnographic research?), we will focus on recently published qualitative studies that included periods of observation among their data collection methods. In this scoping review, we will query the PubMed/Medline database as well as the CINAHL and Scopus databases for ICU-based ethnographic studies that focus on teams or interprofessional care. Teams are defined broadly to include family members.
Phase 2: Data Collection, Analysis, and Synthesis
This phase of the study will be fieldwork intensive, and will last 18 months. In the first year, 4 sites in 2 cities will be studied in depth; in the second year, 4 more sites will be added: 2 in the United States and 2 in Canada.
Ethnography is the systematic and careful observation, documentation, and analysis of the behaviors and attitudes of a group or culture. It often focuses on the meanings and functions of human actions, and thus is based on a constructivist view of reality that aims to develop a holistic, contextualized account of the group or culture studied.7,8,22,23 Through observation, ethnography provides insights about what actually happens in a setting instead of focusing on what people say happens in a setting. 24 Consequently, one key advantage of ethnography is that it provides accounts that minimize social desirability bias, selective perception, and poor recall among participants. 24 Several authors have recently invited greater use of ethnographic research methods in confronting health care challenges generally,8,25 -27 and critical care quality and safety projects more specifically.5,6 Ethnographic accounts have the potential to offer thick descriptions of the realities of intensive care and to provide rich insights into the perspectives of all in the ICU.
Sampling
Intensive care units vary significantly along several dimensions: the age of the population they serve (pediatric vs adult ICUs); the geographic, political, social, and economic territory from which they draw this population (eg, rural, suburban, or urban, percentage insured, etc); the mission of the hospital they are in (research/teaching, community, or for-profit hospitals); their specialty (eg, surgical, medical, neurological, etc); their staff composition (eg, with or without intensivists; with or without nurse practitioners); whether they are “open” (admitting physicians continue to act as primary provider in the ICU) or “closed” (admission requires transfer of responsibility from admitting physician to intensivist). For the first year, we will employ theoretical sampling to choose 4 adult medical ICUs (MICUs) associated with academic centers in 2 urban areas: San Francisco (West Coast) and Baltimore (East Coast) and will use a maximum variation sampling strategy to identify MICUs that varied along the dimensions described above.
Selection of sites in the second year will expand to include 2 further US sites to explore how findings from the year 1 site resonant (or not) with other ICUs. In addition, 2 Canadian ICU sites will be recruited to examine the extent to which the findings are US-specific, or have a wider North American resonance. Selection of these sites will also be guided by findings from the first year of fieldwork, consistent with our iterative design. In addition, to ensure the study elicits perspectives from other ICU contexts, the team may consider the selection of suburban ICUs, surgical or neurological ICUs, or for-profit US hospitals.
Data Collection
The study will gather qualitative (ethnographic) data as well as quantitative (clinical outcomes) data to examine the processes of interprofessional collaboration and patient/family member involvement that occur at each of the selected ICUs, as well as the clinical outcomes that each unit generates. The collection of both these data sets will ensure the study produces a holistic insight into the ICU setting.
Qualitative data
Trained ethnographers at each of the sites will collect data using 3 main techniques: observation, shadowing, and formal and informal interviews. Documents such as patient and family brochures, care protocols, and so on will be collected when pertinent, along with unit-level outcomes data to analyze the intended and unintended effects of these documents on the organization of interprofessional collaboration. 28 Data collection will be undertaken by the use of the nine observational dimensions found in the literature 8 : space (physical layout of the ICU), actors (range of people involved), activity (different care activities), act (single actions undertaken), objects (the role of physical things such as technology), event (moment that invites particular activities), time (the sequencing of events), goals (what actors are trying to accomplish), and feelings (emotions felt and expressed). Observed phenomena will be contrasted with their interpretations and perceptions among staff during both formal and informal interviews.
For observations, the study will employ a marginal ethnographer approach and a selective intermittent time mode. This is a flexible data collection modality that enables fieldworkers to develop relationships with their subjects, and to focus on key aspects of the culture they are observing. 19 Each ethnographer will be assigned specific sites that they will visit intermittently to sample the different rhythms of intensive care through days, nights, weekdays, weekends, and 4 seasons of variation. They will collect data using the dimensions outlined above. The ethnographers will record the daily routines, team interactions and patient and family involvement that are specific to the unit. Others on the ethnographic team will undertake site visits to confirm findings or suggest alternative readings of the site.
Data collection activities will also include ethnographic shadowing of a number of staff members (around 6-8 per site), who will be followed as they go about their duties in the ICU by the site ethnographer. Ethnographers will take notes about what they see, use talk alouds,29,30 and will ask questions about care and practice at mutually agreed-on times.
To generate a comprehensive understanding of the ICU cultures data will be collected for an extended period at the year 1 sites (up to 12 months). This will ensure the study can generate a unique in-depth account of the complexities of ICU interactions and behaviors through a cycle of 1 year. Data collection in year 2 sites will be gathered for a shorter period (up to 6 months), as the purpose of this fieldwork is to explore the wider resonances produced from the year 1 through the collection of comparative ethnographic data.
To generate additional perspectives on the participating ICUs, 8 to 10 staff members at each site will be formally interviewed and asked questions about their career path, their first impressions of ICU care, their understanding of teams and of teamwork in the ICU, and their experiences with patients and families. In addition, 8 to 10 family members will be interviewed and asked about their experience with intensive care, with the care they received, whether and how they participated in the care of their relative in the ICU, as well as their exposure to interprofessional collaboration.
Quantitative data
A variety of ICU clinical outcomes data will also be gathered at each of the participating ICU sites. It is anticipated that the following data will be gathered: patient length of stays, unplanned readmissions, complication rates, infection rates, and error rates (medical errors, adverse drug reactions, near misses, risk-adjusted mortality). Data from each ICU will be anonymized and aggregated before analysis.
Analysis and Synthesis
In line with best practices in qualitative research, data analysis will be conducted alongside fieldwork, and the fieldwork will be adapted accordingly. The research team will meet weekly to discuss observations and refine data collection techniques, thus using researcher triangulation for rigor.31 -35 The coding scheme will be developed in light of the data and from conversations during weekly meetings. Coding and writing of the marginal ethnographer data will aim to flesh out the context of the ICUs by providing thick descriptions of (1) the settings and (2) broad patterns of team interactions along the nine dimensions discussed above. Coding of the shadowing data will focus on the specifics of different roles in the ICU and on situated experience of team dynamics. Coding of interview data will strive to describe the lived experiences of personnel and families in the ICU as they perceive them. Factors influencing delivery of care will be analyzed in light of the framework discussed above: relational, processual, organizational, and contextual.
Aggregated outcomes data from each ICU will be analyzed using SPSS to generate monthly frequencies related to patient length of stays, unplanned readmissions, complication rates, and so forth. These data will also be compared with other sites, and also triangulated with qualitative data to explore any possible associations which may link the observed interprofessional processes and behaviors with the clinical outcomes produced by each participating unit. For example, if it is observed that the communication patterns of members within an ICU are poor and information is shared in a fragmented manner, whereas at another site communication is observed to be timely and well coordinated, the outcomes produced by both units will be compared to establish whether these interprofessional processes have any effect on the ICUs’ respective outcomes.
Ethical Issues
Ethics approval for year 1 sites was obtained from the human subject review boards at University of California, San Francisco (Laurel Heights Panel of the Committee on Human Research, approval date: November 8, 2012) and was obtained from Johns Hopkins (approval date: January 17, 2013). The ethnographers will obtain consent from all staff and family members; pseudonyms will be used throughout. No identifiable information will be collected from either patients or staff. A certificate of confidentiality will be obtained to protect the privacy of practitioners and minimize potential harm to both staff and patients.
Quality Issues
Our design includes several quality checks: iteration, member checks, accounting for negative instances/search for outliers, use of numbers, reflexivity, peer auditing, and triangulation. These mechanisms are part of the best practices suggested in the quality in qualitative research literature.8,18,19,32,36 To maximize the likelihood that our study will be iterative, flexible, responsive, and reflexive, our interprofessional team will meet monthly to discuss data collection, analysis, and results. In addition, an international advisory committee, consisting of a range of clinical and research colleagues will be established to provide expert advice, guidance, and support for the study.
Phase 3: Instrument and Intervention Development
Based on the empirical data gathered from participating ICUs in the previous phase, the study team, with support from the advisory committee, will work together to develop a diagnostic tool that will be used to assess the level of interprofessional collaboration, and patient/family member involvement in any ICU. It is anticipated that this tool will consist of a range of elements (eg, observation checklists, structured interviews) that will need to be triangulated to help generate a rapid, but accurate account of the current state of interprofessional collaboration, and patient/family member involvement on a given ICU.
In addition, based on the empirical data gathered from each of the ICUs, the study will develop a range of interventions aimed at enhancing interprofessional collaboration, and patient/family member involvement. Previous work demonstrated the need to design multiple interventions that span education, practice and organizational activities will be employed in the construction of intervention tools during this phase. 9 Tools developed by the study will be combined whenever possible with previous evidence-based interventions and strategies for enhancing teamwork and communication37 -42 to create multicomponent interventions that can be used in tandem with the diagnostics tools.
Apart from drawing on the expertise of the advisory group during the development of these tools, the study will undertake a validation process whereby 5 international clinical and academic experts will be invited to provide feedback on the accuracy, usability, and reliability of these tools.
Discussion
The importance of interprofessional collaboration in the ICU has been recognized as a linchpin in the delivery of high-quality care, 1 with significant impact on its efficiency and effectiveness. Yet the nature of interprofessional collaboration and how it can be enhanced remains poorly understood. Several scholars have argued that focusing on the context and culture of ICUs is the necessary next step in efforts to improve patient safety and outcomes.4,6,26 According to some, a “well-designed ethnographic study that builds on existing research and utilizes theory-based sampling strategies has the potential to illuminate our understanding of relational phenomena that affect the quality of health care.” 22 This study responds to this call to improve the quality of health care delivery through theory-driven ethnographic research.
It is anticipated that the project will generate a number of outcomes. The initial impact of the study will include sharing of rich descriptive work on the relational, processual, organizational, and contextual aspects of interprofessional collaboration in the intensive care setting. This will be shared via national and international presentations and in peer-reviewed journals. A key outcome of this study is an empirically developed diagnostic tool that will have the capacity to assess the level of effective interprofessional collaboration, and patient/family member involvement, as well as a range of interventions aimed at improving identified shortfalls. It is anticipated that the diagnostic tool and intervention package will be shared and disseminated for wider use.
This study is comparative, iterative, and explicitly grounded in theory, resulting in a high potential for the development of diagnostic tools to assess—and then improve—the quality of teamwork in the ICU.
Footnotes
Acknowledgements
This research is funded by the Gordon and Betty Moore Foundation.
Conflict of Interest:
The author(s) declare no potential conflicts of interest with respect to the authorship and/or publication of this article