
Abstract
Background:
Autoimmune thyroid diseases (AITDs), including Hashimoto’s thyroiditis and Graves’ disease, are characterized by aberrant immune responses influenced by both genetic predisposition and environmental triggers. Genetic association studies have identified several candidate loci that may contribute to the onset and progression of these conditions. The present study investigates the potential impact of specific genetic polymorphisms in interleukin genes (IL17A, IL1B, IL18) and CTLA-4 on thyroid peroxidase antibody (TPOAb) levels in individuals from northwest Iran.
Results:
A total of 82 individuals with elevated TPOAb levels and 82 antibody-negative controls were genotyped for single nucleotide polymorphisms using the tetra-primer amplification refractory mutation system polymerase chain reaction. The analysis revealed significant associations between specific genetic variants and TPOAb levels. Notably, the AG genotype of IL17A rs4711998 was associated with a protective effect, whereas the AA genotype of IL1B rs16944 was correlated with elevated antibody levels, suggesting a potential role in enhancing autoimmune responses.
Conclusions:
These findings underscore the contribution of genetic variations in interleukin genes to the pathogenesis of AITDs in the northwest Iranian population. Elucidating these associations may enhance our understanding of disease mechanisms and contribute to the development of targeted therapeutic strategies.
Keywords
Introduction
Autoimmune thyroid diseases (AITDs), affecting 2–5% of the population, result from an aberration in immune system tolerance, with thyroid antibodies against antigens like thyroid peroxidase (TPO) and thyroglobulin (Tg) present in over 90% of patients (Xing et al., 2021). Among AITDs, Graves’ disease (GD) and Hashimoto’s thyroiditis (HT) exhibit a 5% prevalence, with overlapping antibodies. AITD is more prevalent in women (5:1 to 10:1 ratio), with factors such as postpartum thyroiditis, maternal regulatory T cells, and X-chromosome inactivation contributing to the gender disparity (Wang et al., 2021).
The rise in AITD prevalence, encompassing conditions like type 1 diabetes, suggests a multifactorial etiology involving gene-environment interaction (Dong and Fu, 2014). Environmental factors, including infection, diet, iodine, and smoking, play a substantial role in AITD (Ferrari et al., 2017). While major histocompatibility complex (MHC) class II genes were initially linked to susceptibility, subsequent research identified non-MHC genes influencing AITD etiology (Vaidya et al., 2002). Genetic studies support hereditary predisposition to AITD, with nearly 80% of GD risk attributed to genetic factors. Key genes, including thyroid-specific genes (Tg, TSHR) and immune regulatory genes, influence AITD susceptibility (Shukla et al., 2018).
Interleukin-17A (IL17A), Interleukin-1B (IL1B), and Interleukin-18 (IL18) are key pro-inflammatory cytokines implicated in autoimmune thyroid disorders. IL17A, mainly produced by Th17 cells, drives inflammation through cytokines, chemokines, and matrix metalloproteinases; its gene polymorphisms may influence anti-thyroid peroxidase (anti-TPO) antibody levels (Banerjee et al., 2023; Huangfu et al., 2023; Lu et al., 2023; Wiersinga, 2016). IL1B, produced by macrophages, monocytes, and dendritic cells, initiates immune responses by stimulating cytokine release and leukocyte infiltration, with elevated thyroid levels linked to autoimmunity and potential associations with anti-TPO antibodies (Khalilzadeh et al., 2010; Liu et al., 2010b; Zhao et al., 2013). IL18, secreted by macrophages and dendritic cells, enhances Th1 responses by inducing interferon-gamma, and its increased presence in thyroid tissue suggests a role in sustaining chronic autoimmune inflammation (Liu et al., 2010c; Myśliwiec et al., 2003; Takiyama et al., 2002).
Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) assumes a pivotal role as a regulator within the immune system, exercising control over T-cell activation and subsequent immune responses (Ting et al., 2016). As a member of the CD28/B7 immunoglobulin superfamily, CTLA-4 is expressed on the surface of T cells and functions as a key negative regulator of T-cell activation. Its primary role involves inhibiting co-stimulatory signals essential for T-cell activation, thereby preventing excessive immune responses and maintaining immune homeostasis. The pivotal role of CTLA-4 in autoimmunity has been extensively investigated, particularly in the context of thyroid inflammation and AITDs (Hossen et al., 2023). Alterations in CTLA-4 function have been associated with autoimmune thyroid disorders, highlighting its potential role in the pathogenesis of these conditions (Chistiakov and Turakulov, 2003). As noted, anti-TPO antibodies serve as key biomarkers of autoimmune thyroid disorders, reflecting immune-mediated thyroid tissue damage. Recent research has focused on the potential association between CTLA-4 gene polymorphisms and anti-TPO antibody levels (Ting et al., 2016).
Understanding how specific genetic variations in IL17A, IL1B, IL-18, and CTLA-4 influence the production of anti-TPO antibodies is critical for elucidating the complex genetic basis of AITDs. In the present study, we examine the association of single nucleotide polymorphisms (SNPs) in IL17A (rs8193036 C > T and rs4711998 A > G), IL18 (rs1946518 T > G), IL1B (rs16944 A > G), and CTLA-4 (rs231779 C > T) with anti-TPO levels in a population from northwest Iran.
Material and Methods
Study approval
This case-control study was conducted from September 2021 to September 2022 at the Immunology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran. The study protocol was approved by the Ethics Committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1401.475).
The study was conducted in accordance with ethical guidelines, including the Declaration of Helsinki (1975) and the European Convention on Human Rights and Biomedicine (Oviedo, 4 April 1997), which safeguard human rights and dignity in the application of biology and medicine. All participants provided written informed consent prior to enrollment. Data were recorded and maintained anonymously to ensure participant confidentiality.
Subjects
Participants were stratified according to anti-TPO levels into an anti-TPO–positive group (anti-TPO >30 IU/mL) and an anti-TPO–negative group (anti-TPO <30 IU/mL). Hypothyroidism was diagnosed by an endocrinologist based on clinical criteria, including fatigue, lethargy, constipation, dry skin, and increased sensitivity to cold, among other symptoms. Laboratory assessments included measurement of serum anti-TPO, thyroid-stimulating hormone (TSH), and vitamin D levels. Anti-TPO and vitamin D concentrations were determined using enzyme-linked immunosorbent assay (ELISA) kits (Monobid Co., USA, and Abcam Co., UK, respectively), while TSH levels were measured using an ELISA kit from Padtan Gostar, Iran.
A total of 82 anti-TPO–positive subjects (64 females and 18 males) from the Azari population were recruited for the anti-TPO–positive group. The age of the case group ranged from 21 to 60 years, with a mean of 39.95 ± 9.03 years. The control group consisted of 82 anti-TPO–negative individuals (52 females and 30 males) of the same ethnicity and comparable age, who were randomly selected for inclusion. The age of the control group ranged from 16 to 60 years, with a mean of 40.74 ± 11.31 years. Participant characteristics are summarized in Table 1.
Characteristics of Participants and Their Anti-TPO, THS, and Vitamin D3 Level
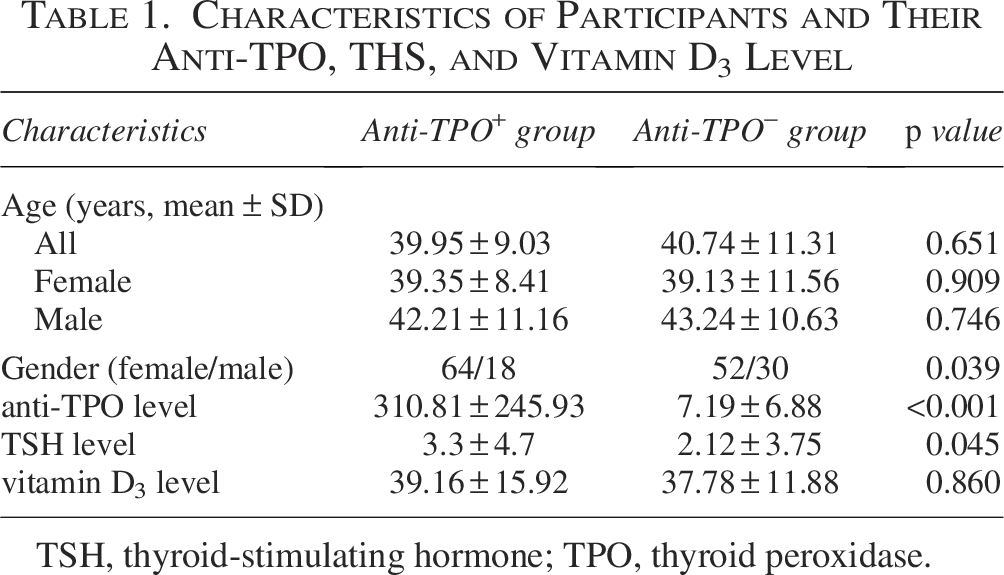
TSH, thyroid-stimulating hormone; TPO, thyroid peroxidase.
DNA extraction
For sample collection, 2 mL of peripheral blood was obtained from each participant using sterile ethylenediaminetetraacetic acid vacutainers. Genomic DNA was extracted using a column-based DNA extraction kit (GeneAll, Seoul, South Korea) following the manufacturer’s protocol. Briefly, 300 µL of blood was transferred into a 1.5–2 mL microcentrifuge tube, followed by the addition of 20 µL proteinase K and 200 µL cell lysis buffer. The mixture was vortexed for 15 s and incubated at 60°C for 15–20 min. Subsequently, 200 µL binding buffer was added and vortexed for 15 s, after which the solution was transferred to a spin column and centrifuged at 6,000×g for 1 min. The column filter was sequentially washed: 500 µL Wash I (centrifuged at 12,000×g for 1 min), 500 µL Wash II (centrifuged at 12,000×g for 1 min), and 500 µL Wash III (centrifuged at 12,000×g for 2 min), with the filter transferred to a new collection tube after each wash. To remove residual wash buffer, the column was centrifuged at 18,000×g for 3 min. DNA was eluted by transferring the filter to a new 1.5–2 mL microcentrifuge tube, adding 100 µL elution buffer, and incubating at room temperature for 5–10 min, followed by centrifugation at 12,000×g for 1.5–2 min. DNA concentration and purity were assessed using a Nanodrop spectrophotometer, and the extracted DNA samples were stored at –20°C until further use.
Genotyping
Genotyping of IL17A (rs8193036 and rs4711998), IL18 (rs1946518), IL1B (rs16944), and CTLA4 (rs231779) SNPs was performed using tetra-primer amplification refractory mutation system polymerase chain reaction (tetra-ARMS-PCR). Primers were designed using Oligo Analyzer v1.0.3 software based on sequences retrieved from the NCBI database. After validation, primers were synthesized by Sinacolon Co. For each PCR reaction, 7.5 µL of 2X PCR Mastermix (Amplicon, Denmark), 0.5 µL of each primer, and 1 µL of genomic DNA were combined. Distilled water was added to reach a final reaction volume of 15 µL. PCR amplification conditions were as follows:
PCR products were subjected to electrophoretic separation on a 2% agarose gel prepared with 0.5X Tris-Boric acid-EDTA (TBE) buffer and stained with a DNA-safe dye. Following electrophoresis, samples were interpreted as follows: the presence of a single wild-type fragment was designated as wild-type homozygote, the presence of a single mutant fragment was designated as mutant homozygote, and the presence of both wild-type and mutant fragments was designated as heterozygote. The size and characteristics of each PCR fragment are summarized in Table 2. Representative results of the gel electrophoresis are presented in Figure 1.
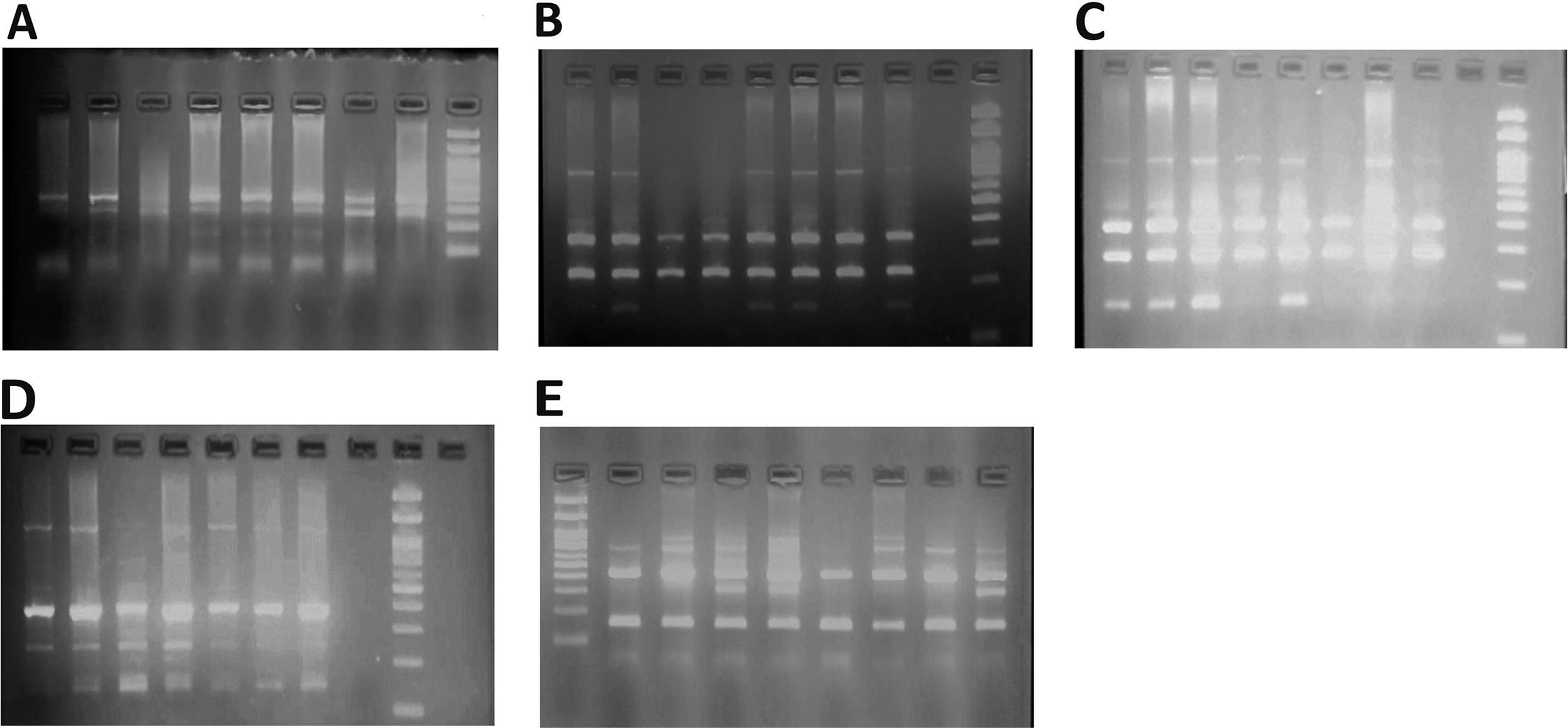
Electrophoretic results.
Characteristics of Interested Genes’ Primers and Fragment Length of PCR Product for Each Allele
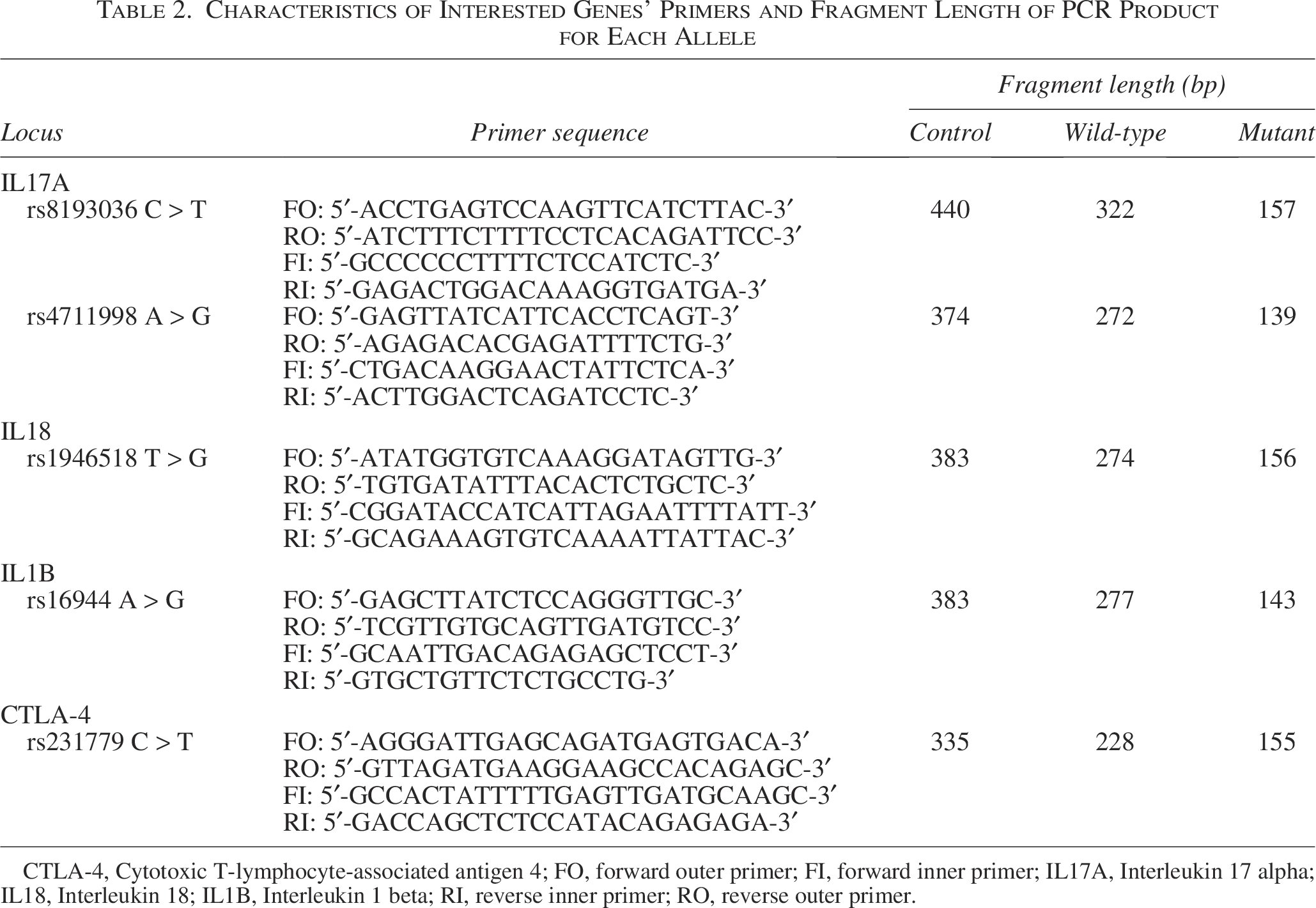
CTLA-4, Cytotoxic T-lymphocyte-associated antigen 4; FO, forward outer primer; FI, forward inner primer; IL17A, Interleukin 17 alpha; IL18, Interleukin 18; IL1B, Interleukin 1 beta; RI, reverse inner primer; RO, reverse outer primer.
Statistical analysis
To assess the normality of the data, the Shapiro-Wilk and Kolmogorov-Smirnov tests were performed. Comparisons between groups were conducted using the Mann-Whitney U test for anti-TPO, vitamin D3, and TSH levels, while an independent-samples t-test was used to compare age between case and control groups. To evaluate the association between gene polymorphisms and anti-TPO levels, odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for each genotype and allele using logistic regression analysis. Associations were further assessed using Pearson’s chi-square test.
The consistency of genotype frequency distributions in the control group with the Hardy–Weinberg equilibrium was evaluated using the chi-square goodness-of-fit test. Statistical significance was defined as a p value less than 0.05. All analyses were performed using STATA version 16 software.
Result
This study investigated the association between IL17A (rs8193036 and rs4711998), IL18 (rs1946518), IL1B (rs16944), and CTLA4 (rs231779) gene polymorphisms and anti-TPO levels in a population from northwest Iran. A total of 82 anti-TPO-positive subjects (64 females and 18 males; mean age 39.95 ± 9.03 years) and 82 anti-TPO-negative controls (52 females and 30 males; mean age 40.74 ± 11.31 years) were recruited. Serum levels of anti-TPO, TSH, and vitamin D3 were measured for all participants. The mean ± SD of anti-TPO levels was 310.81 ± 245.93 IU/mL in the anti-TPO positive group and 7.19 ± 6.88 IU/mL in the control group. The mean ± SD TSH levels were 3.3 ± 4.7 mIU/L in the case group and 2.12 ± 3.75 mIU/L in controls. Mean ± SD vitamin D3 levels were 39.16 ± 15.92 ng/mL in the anti-TPO positive group and 37.78 ± 11.88 ng/mL in controls.
Comparative analyses revealed a statistically significant difference between the anti-TPO positive and negative groups in anti-TPO levels (P < 0.001) and TSH levels (P = 0.045), whereas no significant differences were observed in vitamin D3 levels (P > 0.05) or age (P > 0.05). The detailed characteristics of participants are summarized in Table 1.
The distribution of genotypes and allele frequencies for each polymorphism in both anti-TPO-positive and negative groups is summarized in detail. For IL17A (rs8193036 C > T), 37 CT and 45 TT subjects (22.6% C and 77.4% T) were observed in the anti-TPO positive group, compared with 36 CT and 46 TT subjects (22% C and 78% T) in the control group. For IL17A (rs4711998 A > G), the anti-TPO positive group included 11 AA, 41 AG, and 30 GG subjects (38.4% A and 61.6% G), while the control group comprised 2 AA, 59 AG, and 21 GG subjects (38.4% A and 61.6% G). For IL18 (rs1946518 T > G), 14 TT and 68 TG subjects (58.5% T and 41.5% G) were present in the anti-TPO positive group, compared with 12 TT and 70 TG subjects (57.3% T and 42.7% G) in controls. For IL1B (rs16944 A > G), 52 AA and 30 AG subjects (81.7% A and 18.3% G) were observed in the anti-TPO positive group, whereas the control group had 37 AA, 43 AG, and 2 GG subjects (71.3% A and 28.7% G). For CTLA4 (rs231779 C > T), 34 CC and 48 CT subjects (29.3% C and 70.7% T) were present in both anti-TPO positive and negative groups. All polymorphisms showed significant differences in genotype distribution according to the Hardy–Weinberg equilibrium (P < 0.05).
The evaluation of associations between IL17A (rs8193036 C > T and rs4711998 A > G), IL18 (rs1946518 T > G), IL1B (rs16944 A > G), and CTLA-4 (rs231779 C > T) polymorphisms and anti-TPO levels revealed the following significant findings; For IL17A rs4711998, the AG genotype was significantly associated with lower anti-TPO levels (OR = 0.48, 95% CI = 0.24–0.96, p = 0.039). Regarding IL1B rs16944, the AA genotype was significantly associated with higher anti-TPO levels (OR = 2.01, 95% CI = 1.07–3.77, p = 0.029), while the G allele was linked to a lower risk or better condition (OR = 0.55, 95% CI = 0.33–0.93, p = 0.027). No significant associations were observed between anti-TPO levels and IL17A rs8193036, IL18 rs1946518, or CTLA-4 rs231779 polymorphisms. Table 3 provides a detailed summary of genotype frequencies and the results of the association analyses.
The Characteristics of Interested Gene Polymorphisms in Anti-TPO+ and Anti-TPO− Subjects and OR and 95% CI and p value of Hardy–Weinberg Equilibrium for Each One
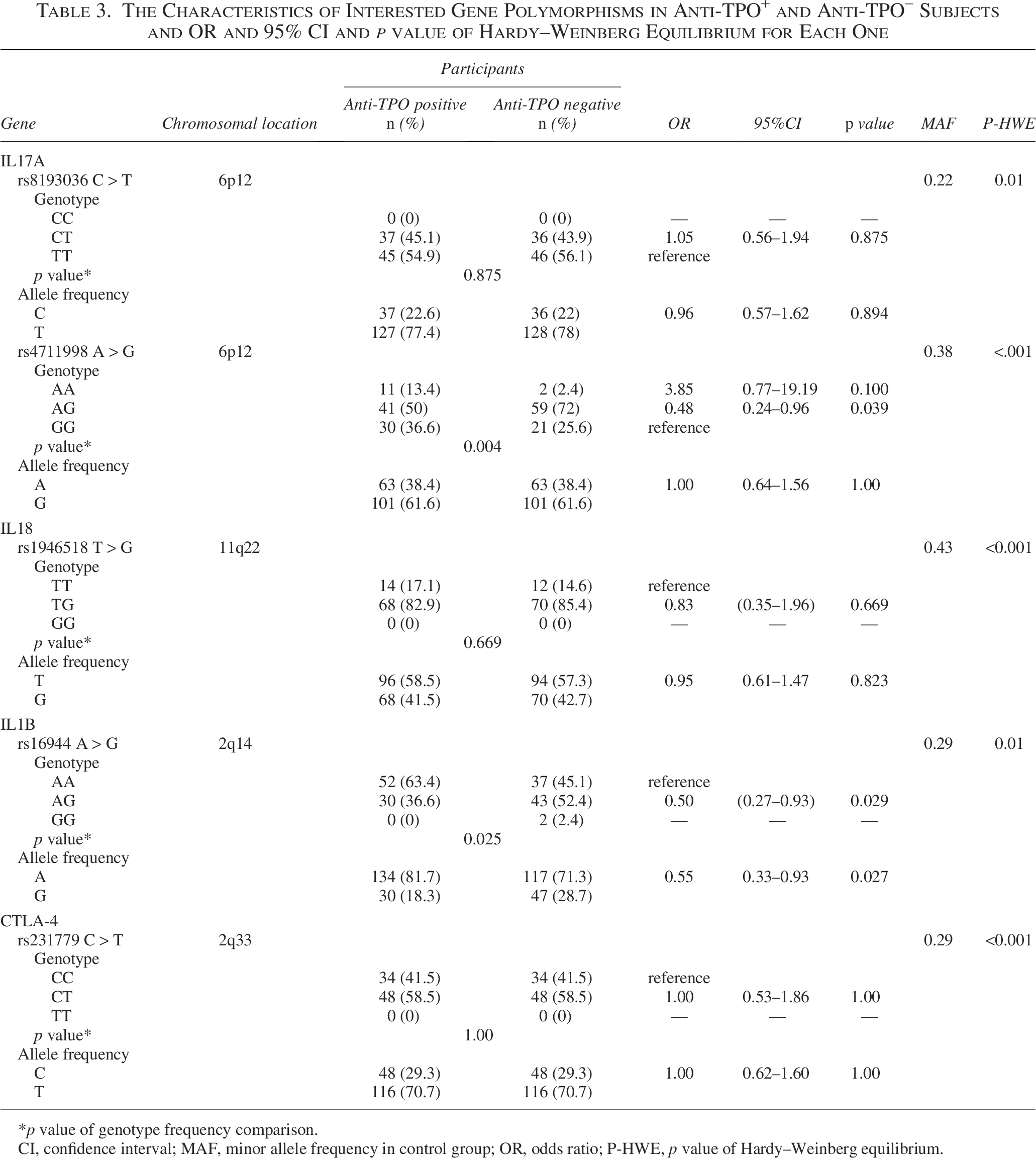
*p value of genotype frequency comparison.
CI, confidence interval; MAF, minor allele frequency in control group; OR, odds ratio; P-HWE, p value of Hardy–Weinberg equilibrium.
To explore the influence of combined genotypes on anti-TPO levels, we compared subsets of case participants carrying different combinations of polymorphisms. Significant differences in anti-TPO levels were observed between the following genotype groups:
rs16944 AA, rs8193036 CT, rs4711998 AG, rs1946518 TG, rs231779 CT (n = 7) vs rs16944 AA, rs8193036 CT, rs4711998 GG, rs1946518 TG, rs231779 CC (n = 4), P = 0.038. rs16944 AA, rs8193036 CT, rs4711998 AG, rs1946518 TG, rs231779 CT (n = 7) vs rs16944 AA, rs8193036 TT, rs4711998 AG, rs1946518 TG, rs231779 CC (n = 7), P = 0.013. rs16944 AA, rs8193036 GG, rs4711998 TG, rs1946518 TG, rs231779 CC (n = 4) vs rs16944 AA, rs8193036 TT, rs4711998 AG, rs1946518 TG, rs231779 CC (n = 7), P = 0.008. rs16944 AA, rs8193036 TT, rs4711998 AG, rs1946518 TG, rs231779 CC (n = 7) vs rs16944 AG, rs8193036 TT, rs4711998 AG, rs1946518 TT, rs231779 CT (n = 3), P = 0.017.
These results suggest that specific combinations of IL17A, IL18, IL1B, and CTLA-4 genotypes may interact to influence anti-TPO levels among affected individuals.
Discussion
In this case-control study, we evaluated the association of IL17A (rs8193036 C > T and rs4711998 A > G), IL18 (rs1946518 T > G), IL1B (rs16944 A > G), and CTLA-4 (rs231779 C > T) SNPs with anti-TPO positivity. Our results showed that genotype frequencies differed significantly between the case and control groups for IL17A rs4711998 A > G (p = 0.039) and IL1B rs16944 A > G (p = 0.029).
The Hardy–Weinberg equilibrium analysis revealed a significant deviation in genotype frequency distribution for IL17A rs4711998 (p < 0.001). Notably, the AG genotype was associated with lower anti-TPO levels, suggesting that heterozygosity at IL17A rs4711998 may confer a protective effect against anti-TPO production. These findings indicate that the IL17A rs4711998 polymorphism could serve as a potential genetic marker influencing anti-TPO levels in patients with AITD.
In the study by Qi et al., the association between IL17A rs4711998 polymorphism and GD was evaluated, and their results demonstrated that the G allele of IL17A rs4711998 was significantly associated with an increased risk of GD (OR = 1.22, 95% CI = 1.03–1.45, p = 0.023) (Qi et al., 2016). Other studies we reviewed focused on the association of different IL17A polymorphisms with various AITDs; however, no study has investigated the potential relationship between IL17A rs4711998 polymorphism and anti-TPO levels (Yan et al., 2012). Moreover, in the study by Qi et al., IL17A rs8193036 showed no association with AITD, which aligns with our findings. To the best of our knowledge, our study is the first to investigate the association between IL17A rs4711998 polymorphism and serum anti-TPO levels.
Regarding IL1B rs16944 polymorphism, the Hardy–Weinberg equilibrium test in our study showed a significant deviation in genotype frequency distribution (p = 0.01). Moreover, the AA genotype was significantly associated with elevated anti-TPO levels (OR = 2.01, 95% CI = 1.07–3.77, p = 0.029), suggesting that it may serve as a potential risk marker for aggravation.
Polymorphisms within the IL1 gene have been implicated in multiple autoimmune conditions, including inflammatory bowel disease (Bioque et al., 1995), rheumatoid arthritis (Marinou et al., 2009), systemic lupus erythematosus (Tsai et al., 2009), and AITD (Mikoś et al., 2014). The cytokine IL1B has pleiotropic effects, playing a key role in modulating cytokine production, cell signaling, and immune cell migration (O’Sullivan et al., 2006). Despite numerous investigations, the potential involvement of the IL1B-511 C/T (rs16944) polymorphism in AITD remains inconclusive. While the TT genotype has been identified as a protective factor against GD in some studies, other reports have failed to demonstrate a consistent association with autoimmune thyroid disorders, highlighting the complex and context-dependent role of IL1B in thyroid autoimmunity (Chen et al., 2005; Liu et al., 2010a, 2010b; Zaaber et al., 2016). In some studies, conflicting findings have been reported, with others detecting no significant association between this polymorphism and either GD or HT (Chen et al., 2006; Durães et al., 2014; Khalilzadeh et al., 2009, 2010). Notably, a meta-analysis highlighted an ethnic disparity, indicating a significant association between the IL1B-511 (rs16944) SNP and GD in Asian populations, whereas no such association was observed in Caucasian populations (Jager et al., 2010).
Comparison of the polymorphism profiles of case individuals and their anti-TPO levels suggests that co-inheritance of certain gene polymorphisms may be associated with significantly higher anti-TPO levels. However, due to the small number of subjects in each genotype combination, these findings remain inconclusive and require further investigation.
Despite our efforts, this study had several limitations that may have influenced the reported negative results. These included a limited sample size, which reduced the statistical power, reliance solely on tetra-ARMS-PCR without confirmation by other methods such as sequencing, and restriction to the Azari population in northwest Iran. Larger studies using more precise genotyping techniques would be beneficial to achieve more conclusive results.
Conclusion
In conclusion, this study evaluated the association between specific genetic variations in IL17A, IL1B, IL18, and CTLA-4 and serum anti-TPO antibody levels in a population from northwest Iran. We focused on selected SNPs in these genes to explore their potential links to autoimmune thyroid diseases, particularly Hashimoto’s thyroiditis and GD. The study included 82 anti-TPO-positive individuals and 82 anti-TPO-negative controls.
The results revealed significant associations between specific genetic variations and anti-TPO levels. Notably, the IL17A rs4711998 AG genotype was associated with lower anti-TPO levels, suggesting a potential protective role, whereas the IL1B rs16944 AA genotype was linked to increased anti-TPO levels, indicating a possible aggravating effect. These findings highlight the influence of individual genetic profiles on autoimmune thyroid disease susceptibility and antibody production.
These findings enhance our understanding of the genetic basis of autoimmune thyroid disorders, highlighting the role of specific variations in the IL17A and IL1B genes in influencing anti-TPO antibody levels. Nonetheless, the study has limitations, including a relatively small sample size, which underscores the need for further research to validate and expand upon these results. Overall, this work provides valuable insights into the complex genetic factors contributing to autoimmune thyroid diseases in the northwest Iranian population.
Authors’ Contributions
Conceptualization, A.A.H. and S.S.F.; methodology, A.A.H. and S.S.F.; formal analysis, P.S.; writing—original draft preparation, A.H.; writing—review and editing, A.H. and S.S.F.; visualization, A.H.; supervision, S.S.F. All authors have read and agreed to the published version of the article.
Footnotes
Funding Information
This work is financially supported by Tabriz University of Medical Sciences, Tabriz, Iran, to study any possible correlation between SNPs and anti-TPO level.
Ethics Approval and Consent for Publication
The present study has been approved by the ethics commission of Tabriz University of Medical Sciences (IR.TBZMED.REC.1401.475). Written informed consent for the publication of this case report was obtained from the participants.
Data Availability Statement
Data will be made available on request.
Author Disclosures Statement
No potential conflict of interest relevant to this article was reported.