
Abstract
Background
Pure endoscopic surgery (functional endoscopic sinus surgery) has been increasingly replacing external approaches in the management of sinonasal inverted papillomas.
Objective
To analyze and compare the effectiveness of pure endoscopic procedure with external or combined procedures to paranasal inverted papillomas, including the experience from two institutions in North Greece, over a 20-year period.
Methods
Systematic literature searches of MEDLINE (1952–2016), EMBASE (1974–2016), and the Cochrane Central Register of Controlled Trials. Review of all English-language studies comparing endoscopic and open techniques. Odds ratios (ORs), risk ratio, 95% confidence intervals (CIs), and tests for heterogeneity were reported. Recurrence rates according to initial tumor stage.
Results
In total, 2451 patients had been enrolled in the 23 studies, published between 1992 and 2014. All the included articles are graded as level IV evidence. Among the 1526 patients of the endoscopic group, 212 (13.8%) had recurrence, with the mean time of recurrence to range from 14 to 46.6 months. In the external approach group, 111 (18.7%) of the 592 patients had recurrence, with the time of recurrence to range from 7 to 92 months. The recurrence rate in the combined approach group was 12.9%. The occurrence rate of recurrence attributable to the surgical choice was significantly different between endoscopic and external group (OR: 0.61; 95% CI: 0.40–0.92; P = 0.02; 14.9% vs. 18.8% in endoscopic and external group, respectively).
Conclusions
The present systematic review and meta-analysis indicates that endoscopic approach seems a favorable treatment option of sinonasal inverted papillomas and confirms the global recommendation that is the gold standard in the treatment of such nose lesions, revealing a lower recurrence rate compared to external approaches.
Keywords
Introduction
Inverted papilloma (IP) is relatively rare benign epithelial sinonasal lesion, accounting for 0.5% to 4% of all surgically removed primary nasal tumors.1,2 Its clinical interest is based on tumor’s trend to be locally aggressive, having high recurrence rate and association with malignancy.
Removal of all mucosal disease is considered the key factor to prevent the recurrence of the tumor, with exclusion of synchronous malignancy of the removed lesion’s specimens to be needed. Long-term follow-up of such patients is recommended, as recurrence or metachronous malignancy can occur even after many years after disease’s onset.
Historically, conservative treatment approach of IPs with endonasal nonendoscopic “polypectomies” resulted in unacceptably high recurrence rates up to 78%. 3 This local excision was replaced by radical external approaches, with medial maxillectomy via lateral rhinotomy or midfacial degloving to be considered as “gold standard” technique. Over the past 20 years, the progress in endoscopic sinus surgery has revolutionized the management of such sinus pathology, achieving comparable results and limiting the morbidity of external approaches.
The aim of the present systematic review and meta-analysis is to analyze and compare the effectiveness of pure endoscopic procedure with external or combined procedures to IPs. Our experience from two institutions in North Greece, over a 20-year period, is included.
Material and Methods
Systematic Review and Meta-Analysis
A computer systematic literature search in MEDLINE, Ovid, EMBASE, the Cochrane Database of Systematic Reviews, and CENTRAL electronic databases was performed by one of the reviewers (JG) from 10 February 2015 to 10 March 2015, in order to identify studies that answered the question of interest. For this purpose, the following free-text terms were used: “papilloma inverted/inverting” or “Schneiderian” combined with “nose” or “sinus” or “paranasal” or “sinonasal” or “head” and limited to “human.”
Additionally, extensive hand-searching of the references of all relevant studies was also performed. Only English-language primary studies were applied. Results were further limited to exclude case reports, editorials, letters, and exclusive surgical technique descriptions and reviews.
All criteria for inclusion/exclusion of studies in the present systematic review were specified prior to the literature search. In order for a study to be eligible, the following criteria should be met: (a) the study should report management of sinonasal IPs, comparing pure endoscopic resection with external or combined (external plus endoscopic) surgical techniques, (b) the population size of each study group should be at least 10 patients, and (c) the study should report clearly the performed surgical approach, following up the patients for at least 12 months.
The following exclusion criteria were established: (a) any case report or case series of less than 10 cases in each group, (b) any study reporting nonendoscopic “polypectomies,” and (c) any study reporting cumulative recurrence rates, without reporting them in accordance with the type of operation performed.
Quantitative Data Synthesis
The RevMan software 5.3 (The Cochrane Collaboration, 2014) was used in order to combine the results for meta-analysis. Inconsistency of studies (study-to-study variation) was assessed by using the χ2 statistic (the hypothesis tested was that the studies are all drawn from the same population, i.e. from a population with the same effect size). A fixed effects model was used, where no heterogeneity was present, whereas a random effects model was applied in the presence of significant heterogeneity.
Our Experience
The medical records of the patients with sinonasal IPs, diagnosed and treated in Otorhinolaryngology—Head & Neck Surgery Departments of AHEPA University Hospital and Papanikolaou General Hospital, were reviewed retrospectively. Both the Local Commission of Bioethics of AHEPA University Hospital and the Institutional Review Board (IRB) of Papanikolaou General Hospital approved the protocol of the review of medical records (IRB number is not available). The patients were evaluated for age at diagnosis, gender, site of lesion, surgical approaches and procedures, occurrence of associated malignancy, and recurrence rate. Inclusion in the study also required, apart from a histologically proven case of IP, a minimum 12-month follow-up period. The extent of sinus involvement was assessed from imaging studies and intraoperative findings.
Surgical approach and extent of surgery was dictated by the site of origin and extent of the disease while routinely informing the patient in case of endoscopic approaches for the probability of switching to an external one depending on intraoperative findings. A variety of external (Caldwell-Luc, lateral rhinotomy, midfacial degloving, etc.) approaches were used. Endoscopes were used primarily during the latter half of the 20-year period examined here, mirroring both technological advances and our growing experience on the field.
Results
Systematic Review and Meta-Analysis
The electronic search resulted in the identification of 1009 publications. Subsequently, the exclusion of irrelevant studies according to their title resulted in 384 potentially eligible publications. The abstracts of these studies were examined, and 212 manuscripts were identified that could provide data to answer the research question of interest (Figure 1). The full texts of these studies were examined thoroughly, resulting in the exclusion of 189 publications. In total, 2451 patients had been enrolled in the 22 studies4–25 (Figure 1).
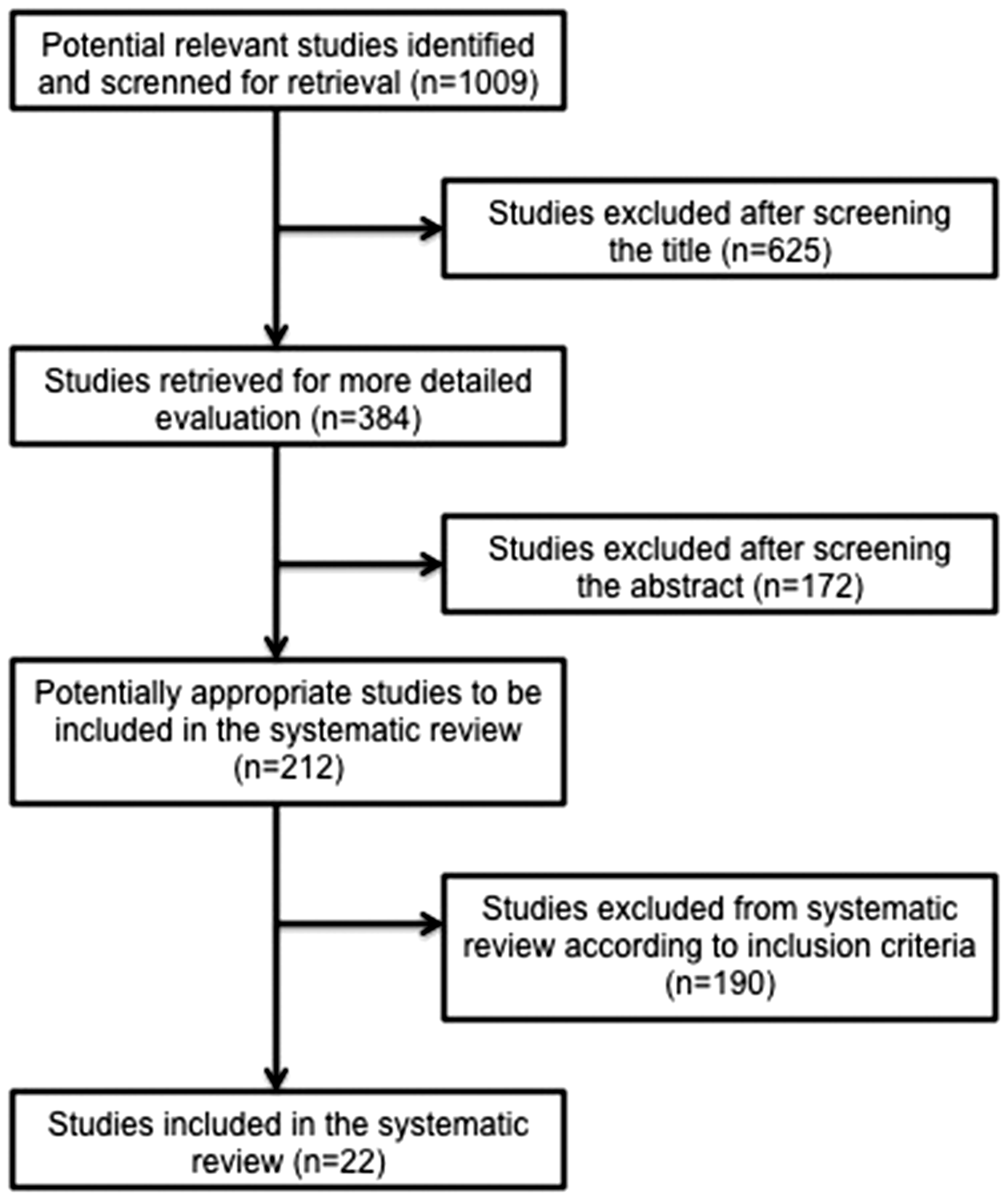
Flow diagram for study selection.
In Table 1, we present in chronological order the 23 studies (including our experience), comparing the endoscopic approach of IPs with either external or combined operation. The eligible studies were published between 1992 and 2014. All the included articles are graded as level IV evidence. The study size in the included studies ranged from 27 to 578 patients. Pooling the patients of each study, endoscopy group includes 1526 patients, external 592, and combined 333 patients. Reviewing the characteristics of the surgical procedures of the included studies, in 12 studies, pure endoscopic approach was compared with the external approach. In seven studies, endoscopic treatment of IPs was compared to combined approach, and in four papers, results of three different study groups (endoscopic, external, and combined) were presented. The follow-up period ranged from 12 to 74 months. The overall malignancy rate was 4.9%, with 122 cases presenting either synchronous or metachronous neoplasia.
General Characteristics of the Included Studies.
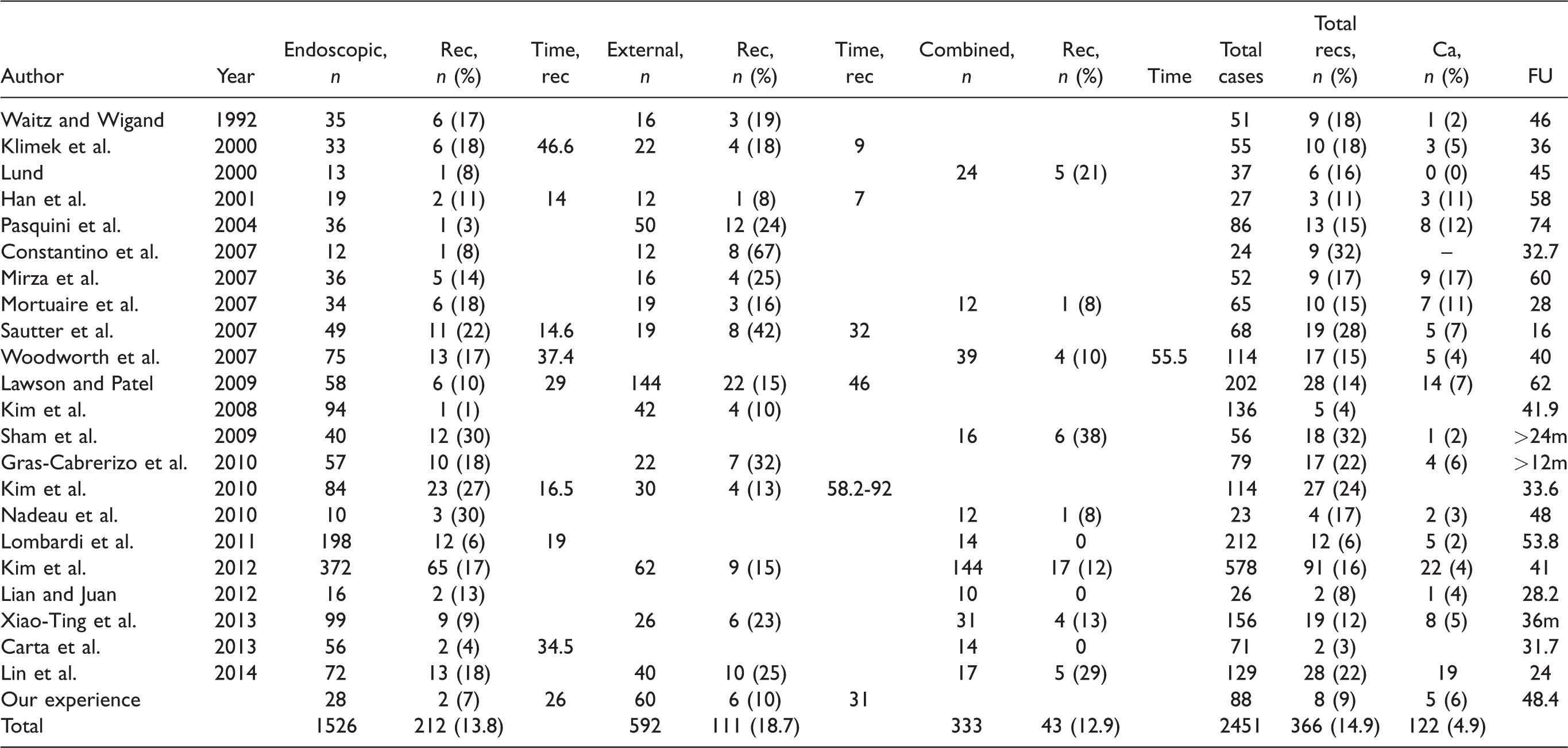
Rec: recurrence; FU: follow-up.
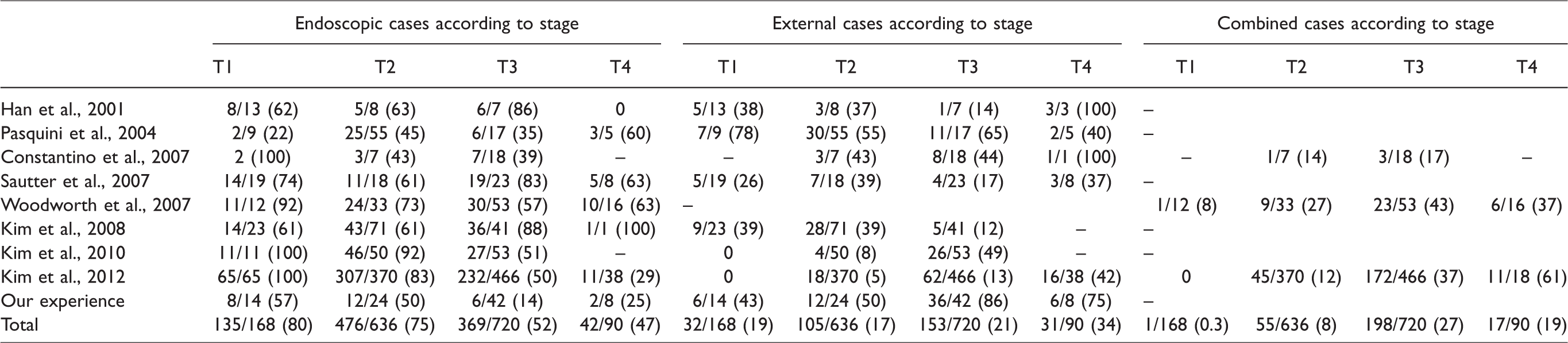
According to Krouse staging system, the majority of patients (80%) with T1 stage received endoscopic approach. 26 Regarding the T2 tumors, endoscopic approach seems to be the first treatment choice (75%). As tumor’s size increased, the rate of external or combined increased (Table 2).
Surgical Approach According to Staging System.
Among the 1526 patient of the endoscopic group, 212 (13.8%) had recurrence, with the mean time of recurrence to range from 14 to 46.6 months. In the external approach group, 111 (18.7%) had recurrence, with the time of recurrence to range from 7 to 92 months. The recurrence rate in the combined approach group was 12.9%. The occurrence rate of recurrence attributable to the surgical choice was significant different between endoscopic and external group (odds ratio (OR): 0.61; 95% confidence interval (CI): 0.40–0.92; P = 0.02; 14.9% vs. 18.8% in endoscopic and external group, respectively) (Figure 2). However, the occurrence rate of recurrence did not differ significantly between endoscopic and combined group (OR: 1.26; 95% CI: 0.86–0.1.84; P = 0.23) (Figure 3).
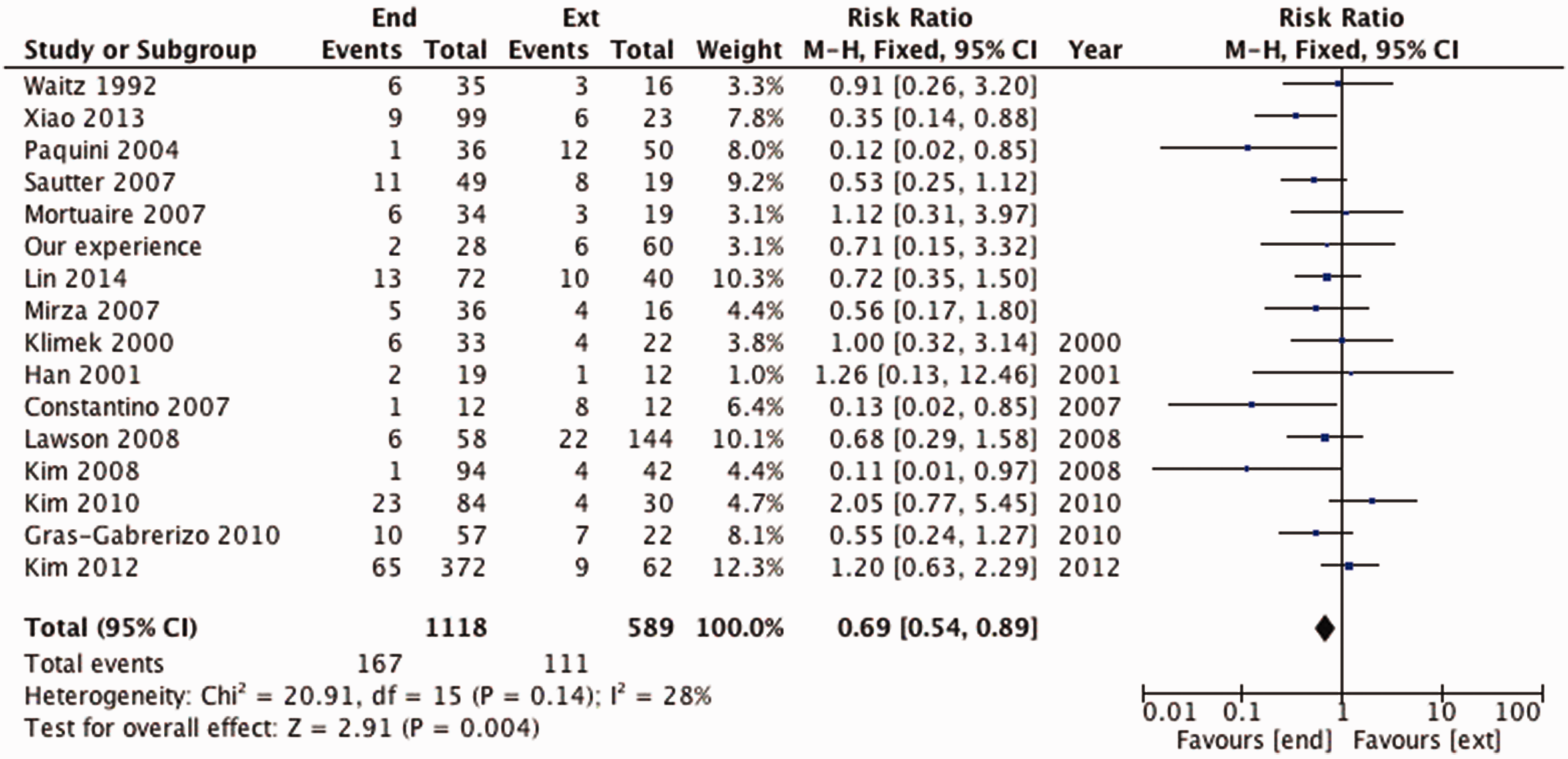
Risk ratio (RR) of recurrence attributable to the surgical choice, evaluating the difference between endoscopic and external group in favor of endoscopy, with the difference being statistically significant (P < 0.05). The measure of effect of each study and of the meta-analysis is represented with a square and a diamond, retrospectively. The vertical line representing no effect is also plotted.
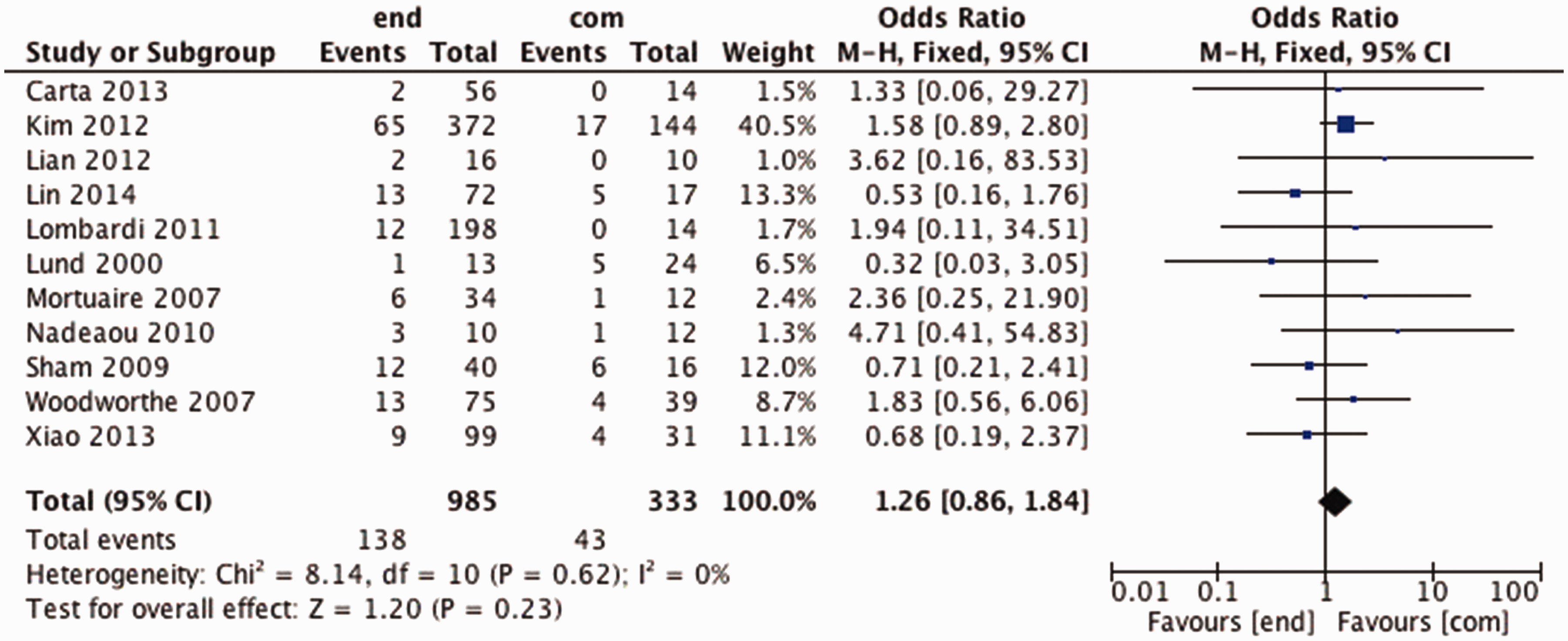
Odds ratio (OR) of recurrence attributable to the surgical choice, evaluating the difference between endoscopic and combined group in favor of endoscopy, without this difference being statistically significant (P > 0.05). The measure of effect of each study and of the meta-analysis is represented with a square and a diamond, retrospectively. The vertical line representing no effect is also plotted.
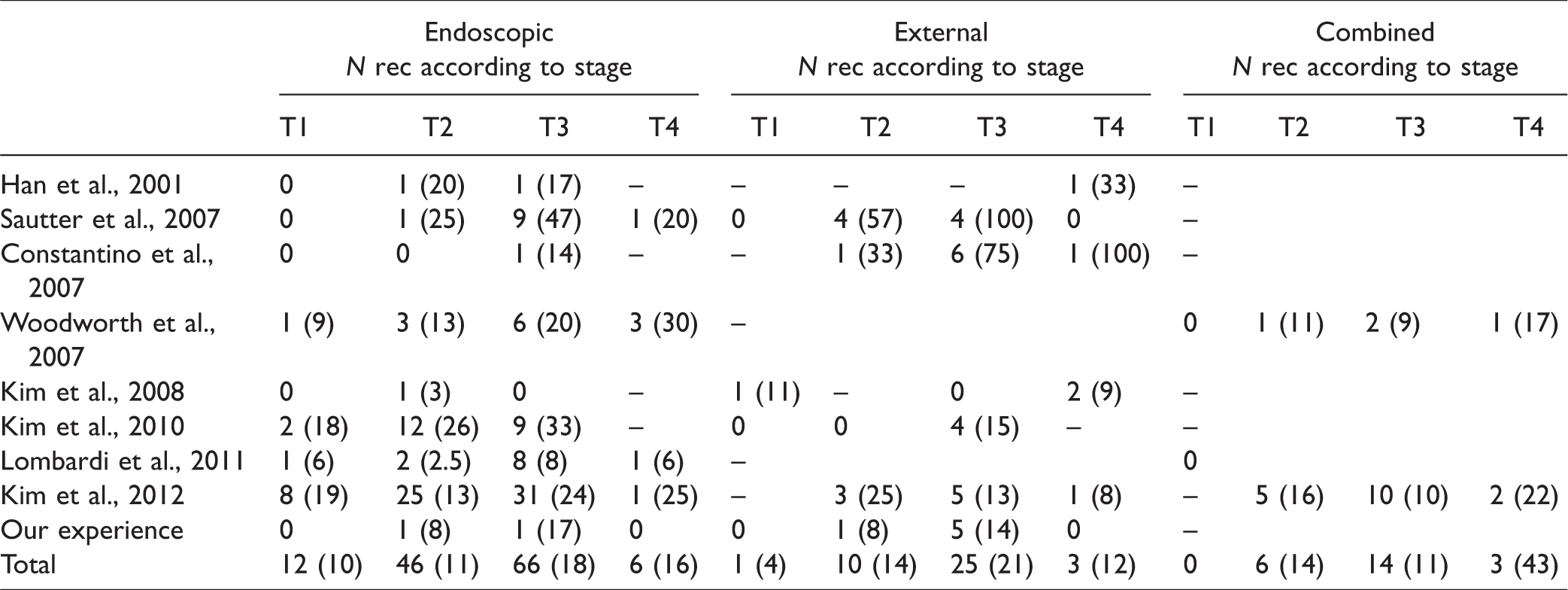
In Table 3, nine studies providing the recurrence rates according to surgical approach in each stage are presented. The comparison of recurrence rates in each of the stages did not reveal statistically significant difference between endoscopic and external or combined approach (P > 0.05).
Recurrence Rates According to Surgical Approach in Each Stage.
Our Experience
Between 1991 and 2011, 88 patients with IP were identified being treated in the two departments. Among the patients, were 70 men and 18 women, with mean age of 56.1 years and age range of 19 to 87 years.
According to Krouse’s staging system, 57% of T1 cases received endoscopic approach. As the stage increased, the rate of open approach increased, with the 86% of T3 and 75% of T4 treated with an external approach. Follow-up period ranged from 12 months to 5 years, with a mean of 48.4 months. During follow-up period, a total of eight patients subsequently developed recurrences, raising recurrence rate to 9%. All the recurrences were observed at the same site as the previous primary tumor origin. The mean interval between surgical treatment and diagnosis of recurrence was 30 months (range 12–48). Among the 88 patients, 28 underwent resection via endoscopic approach and 60 via external approach. The recurrence rate according to surgical approach was 7% and 10%, respectively. The recurrence rate according to surgical approach in each stage is presented in Table 1.
In the pathological review, malignancy was detected in 5 out of the 88 original cases (6%); all cases were diagnosed with squamous cell carcinoma. All cases of synchronous malignancy had undergone a lateral rhinotomy approach. Interestingly, three out of five patients (60%) presenting malignancy were female. In all cases, postoperative radiation therapy (60–65 Gy) on the primary site was planned. No recurrence was noted during follow-up.
Discussion
Incomplete resection of the tumor is considered the main causative factor for recurrence. Surgeon’s choice for the treatment of IPs is guided by the purpose to remove completely the lesion, reducing surgical morbidity. The external approach had long been considered the gold standard of IPs and the method against which others judged.27,28 The introduction of endoscopic techniques and improvement of surgical instrumentation, together with intraoperative navigation equipment, have revolutionized the management of such sinonasal lesions. In the past 20 years, many studies have confirmed the validity and efficacy of endoscopic approaches in the treatment of complex sinonasal pathology, obviating the morbidity of external approaches. 29
Purpose of present systematic review was to evaluate in an evidence-based way the available literature, comparing the recurrence rates of endoscopy-treated IPs with those managed with external or combined approaches. Certain inclusion criteria were set in order to minimize the inherent drawbacks of observational studies. Main conclusion of our systematic review is the significant lower recurrence rate of the IPs of the endoscopic approach than of the open approach. A previously published systematic review of the literature also supported the endoscopic resection as a favorable treatment option for most cases of sinonasal IPs.30,31
Subgroup analysis based on the stage of the disease was also included in our systematic review, using the Krouse system as one of the widely accepted standardized systems. Interestingly, the comparison of recurrence in each stage did not confirm the superiority of endoscopic approach over the external or combined one. However, the fact that only 9 out of 22 included studies provided data regarding the recurrence rate of each stage could be a possible explanation of such lack of difference.
Nowadays, in the hands of an experienced rhinologist with the full series of equipment, the endoscopic techniques are considered the gold standard in each stage of the disease. The systematic review confirmed that endoscopic approach is the first choice of surgeons, regardless of the stage of the tumor. However, it should be noted that the area where the endoscopic approach seems to have significant limitation to remove completely the disease is the frontal sinus and the periorbita when there is intraorbital extension, without use of adjunctive approaches. As pure endoscopic approach in frontal sinus IPs can be a challenge, the surgeon should always consider Draf II or III technique for the adequate exposure of the lesion. In rare cases, osteoplastic flap is still indicated and can be the only solution. 32 The lack of facial incision, the less facial swelling, the shorter operative and inpatient time, and the decreased postoperative pain are considered significant supportive factors of endoscopic approach. It should also be noted that the “concept” of surgical removal of the sinonasal IPs has changed over time. In the past, complete resection of the papilloma, along with the entire sinus mucosa and wide bony removal from all sinus walls, was surgeon’s main goal. Now it seems that we are moving in a more functional surgery, considering “pedicle”-oriented surgery and unifocal localization of the IPs. 33
IP’s association with malignancy attaches clinical importance to their treatment strategy. Hence, papilloma and carcinoma may coexist (synchronous tumors), small focal areas of carcinoma in situ may be found inside a papilloma or more rarely a carcinoma may arise at the original site of a papilloma (metachronous malignant transformation). The association of IP with malignancy varies widely in the literature with a range of 0% to 53% with synchronous malignancy rising to 7.1% and metachronous tumors accounting for 3.6% of the cases.10,34–36 The overall malignancy rate of present systematic review was 4.9%. The vast majority was squamous cell carcinomas, but also transitional cell carcinoma, adenocarcinoma, mucoepidermoid carcinoma, and verrucous carcinoma have been reported. In a synchronous malignant IP without bony erosion, pure endoscopic approach can be a realistic option. However, aggressive growth and capability for regional and distant metastasis raise the need for long-term follow-up with radical surgery followed by postoperative radiotherapy to be the treatment of choice in such cases. 30 Generally, IP-associated malignancy carry a better prognosis than usual paranasal malignancy. 10
The results of the present systematic review are liable to certain limitations, which are in direct dependence on the inherent characteristics of the included studies. First, the current systematic review comprises mainly from retrospective studies that because of their small sample size and short follow-up period are underpowered to detect clinically important differences. It should be noted that in all studies included in the present systematic review, allocation of patients to each treatment group seems to have been based on subjective criteria and not on a specific protocol. For these reasons, potential selection or performance bias cannot be excluded, and thus, the results of this systematic review should be interpreted with caution. However, the analysis of our systematic review of the selected surgical approach in each stage does not advocate the selection bias toward more advanced tumors in the nonendoscopic group (Table 2).
Conclusion
In conclusion, a systematic review and meta-analysis of the literature indicates that endoscopic approach seems a favorable treatment option of sinonasal IPs and confirms the global recommendation that is the gold standard in the treatment of such lesions, revealing a lower recurrence rate compared to external approaches. Considering the risk of recurrence and associated malignancy in the treatment plan of IPs, a minimum follow-up of 5 years is recommended, with possible extension in cases that revision surgery is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.