
Abstract
Background
Endoscopic pituitary surgery (EPS) is increasingly being used for the treatment of pituitary lesions. Obesity is a growing epidemic in our nation associated with numerous comorbidities known to impact surgical outcomes. We present a multi-institutional database study evaluating the association between body mass index (BMI) and postsurgical outcomes of EPS.
Methods
Patients who underwent EPS from 2005 to 2013 were identified from the American College of Surgeons National Surgical Quality Improvement Program database. Preoperative variables, comorbidities, and postoperative outcomes, such as 30-day complications, morbidity, and mortality, were analyzed.
Results
A total of 789 patients were analyzed, of which 382 were obese (BMI ≥ 30) (48.4%). No difference in reoperation rate (P = .928) or unplanned readmission rates (P = .837) was found between the obese versus nonobese group. A higher overall complication rate was observed in the obese group compared to the nonobese counterparts (P = .005). However, when separated into surgical complications (3.7% vs 1.5%, P = .068) and medical complications (7.6% vs 3.9%, P = .027), only medical complications, specifically pneumonia, remained significantly different. EPS on obese patients was also associated with prolonged operating time (154.8 min vs 141.0 min, P = .011).
Conclusions
EPS may be a safe treatment option for pituitary lesions in the obese population. Although obese patients undergoing EPS are at increased risk of medical complications and prolonged operating times, this did not influence mortality, reoperation, or readmission rate.
Keywords
Introduction
Obesity has become an increasing public health concern in the United States, where more than 72 million U.S. adults are obese, 1 equating to a prevalence of 36.5%. Body mass index (BMI) has traditionally been used as a measure of obesity and overweight status. The Centers for Disease Control and Prevention (CDC) defines obesity in adults as a BMI greater than or equal to 30 kg/m2. 2 Obesity has also created a financial burden on society, carrying an estimated annual medical cost of $147 billion in 2008 U.S. dollars. 1 Some health conditions such as heart disease, stroke, and type 2 diabetes have been linked to obesity. 1 Historically, obesity has also been viewed as a significant risk factor for negative postoperative outcomes following nonbariatric surgery because it is associated with apnea, obesity hypoventilation syndrome, and pulmonary embolism (PE).3–7 Furthermore, obesity is associated with excess visceral adipose tissue, which contributes to profound metabolic disturbances and a prothrombotic, pro-inflammatory state. 4 Obesity has also been demonstrated to increase postoperative cardiac arrhythmias, wound dehiscence, and infectious complications. 4
Excessive weight gain can be one of the first clinical signs suggesting Cushing’s Disease, a condition characterized by hypercortisolism due to a pituitary adenoma.8,9 Surgical resection of pituitary adenomas such as those in Cushing’s Disease has become the gold standard of treatment. 10 With continued advancement in endoscopic surgery and improvements in both technique and technology, this approach has gained increasing popularity and has become the ideal method in surgical treatment of pituitary adenomas.11,12 To date, there has been one retrospective review that reported obesity to be an independent predictor of postoperative cerebrospinal fluid (CSF) leak after endoscopic transsphenoidal surgery. 13 In regard to neurologic/neurosurgical disorders, obesity has been associated with idiopathic intracranial hypertension and spontaneous CSF rhinorrhea.14,15 Within the realm of otolaryngologic surgery, the relationship between BMI and outcomes of cervical endocrine procedures such as thyroidectomy and parathyroidectomy has been studied.16–18 One study demonstrated that morbid obesity is associated with longer operation times, a more difficult airway and longer stay in the postanesthesia care unit. 18 A large multi-institutional study showed that those with higher BMI undergoing thyroid and parathyroid surgery were at increased risk of wound complication, had longer operation times, and were more likely to require general anesthesia compared to nonobese patients. The impact of obesity on outcomes following endoscopic pituitary surgery (EPS) has been rarely studied. We aim to conduct the first large-scale, multi-institutional analysis using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database to examine the effect of obesity on postoperative medical complications, surgical complications, reoperation rates, unplanned readmission rates, and other variables in EPS patients.
Materials and Methods
The 2005–2013 NSQIP user files were queried in June 2016 in order to isolate patients who had undergone EPS. This was accomplished through the use of Current Procedural Code 62165. The isolated patients were separated into 2 groups based on weight status, with an obese group (BMI ≤ 30) and a nonobese group (BMI < 30). The NSQIP database allowed us to compare these two groups on the basis of demographics, comorbidities, and 30-day postoperative outcomes. Secondary to the de-identified nature of the NSQIP dataset, this analysis was deemed exempt from the Rutgers New Jersey Medical School Institutional Review Board.
Comorbidities analyzed included diabetes, smoking (<1 year prior to surgery), dyspnea, current alcohol use, chronic obstructive pulmonary disease, congestive heart failure, previous percutaneous coronary intervention, previous myocardial infarction (MI), hypertension (requiring medication), previous transient ischemic attack, previous cerebrovascular accident (CVA), systemic sepsis, functional status (independent/dependent), and American Society of Anesthesiologists (ASA) class (Table 1).
Overall Patient Demographics and Characteristics in Endoscopic Pituitary Surgery.
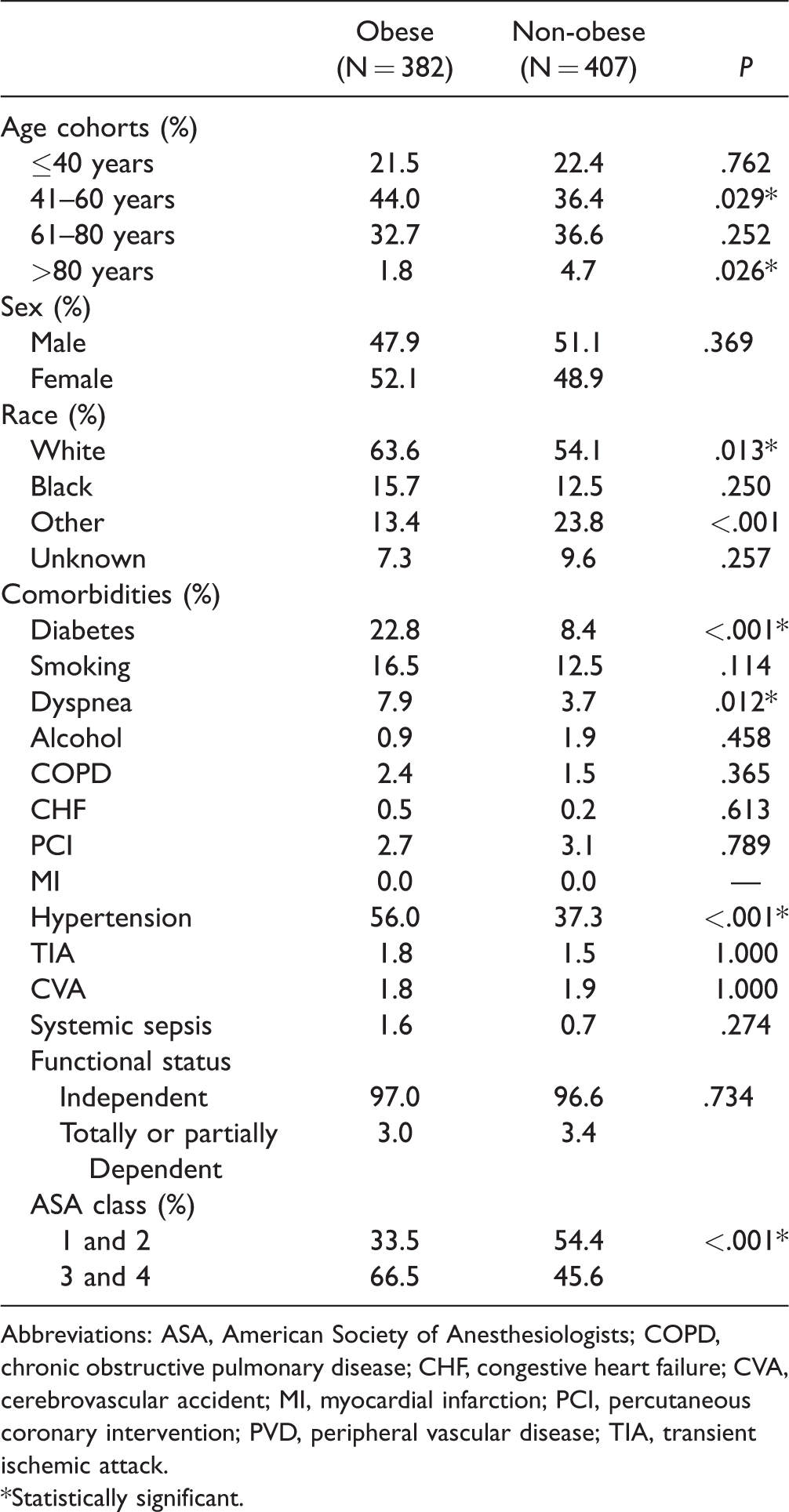
Abbreviations: ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; CVA, cerebrovascular accident; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; TIA, transient ischemic attack.
*Statistically significant.
Postoperative outcomes included overall complications, surgical complications, and medical complications. Surgical complications included superficial, deep, and organ/space surgical site infections, wound disruption, and severe bleeding (requiring blood transfusion within 72 hours of the postsurgical period). Surgical complications more specific to EPS such as CSF leak, diabetes insipidus (DI), and syndrome of inappropriate anti-diuretic hormone (SIADH) are not explicitly tracked in the database and thus could not be analyzed. Medical complications consisted of pneumonia, PE, ventilator use for >48 hours, unplanned reintubation, urinary tract infection (UTI), renal insufficiency (increase in creatinine >2mg/dL above preoperative value), acute renal failure, CVA with neurological deficit, nerve injury, cardiac arrest requiring cardiopulmonary resuscitation, MI, and sepsis. Other outcomes analyzed included rates of mortality, reoperation, readmission, and unplanned readmission as well as operating time and length of stay (Table 2).
Postoperative Complications in Endoscopic Pituitary Surgery.
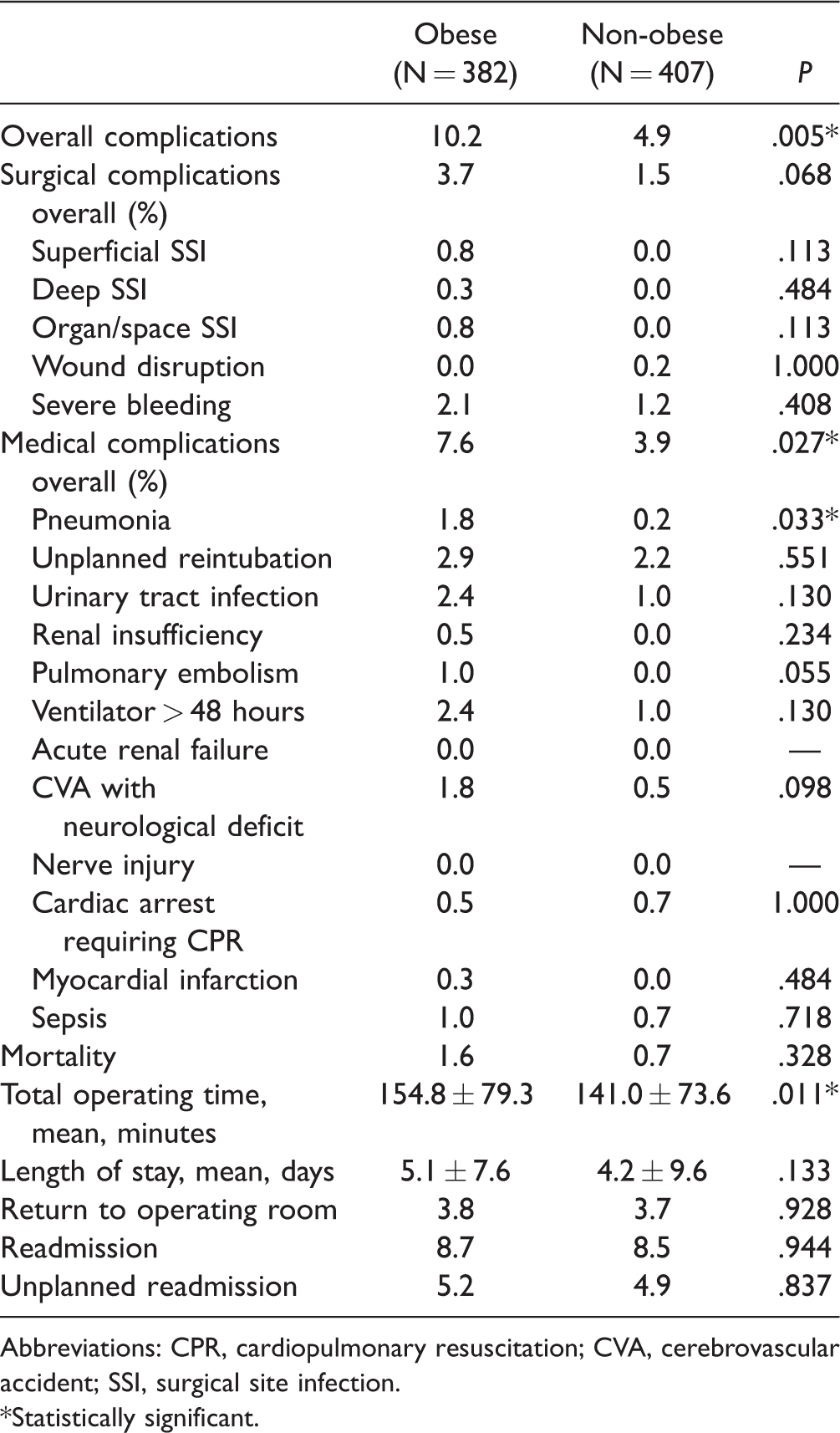
Abbreviations: CPR, cardiopulmonary resuscitation; CVA, cerebrovascular accident; SSI, surgical site infection.
*Statistically significant.
All statistical calculation for this analysis was accomplished via the use of SPSS version 22 (IBM, Armonk, NY). Both groups were compared to one another through the use of Pearson's χ2, Fisher’s Exact, and independent 2-tailed t-tests. Variable differences between the groups were deemed to be statistically significant if the P value was less than .05. Statistically significant postoperative complications were analyzed through the use of a multivariable logistic regression (which accounts for age, gender, race, and statistically significant demographical differences) to determine the independent impact of obesity on postoperative outcomes (Table 3).
Multivariate Logistic Regression for Postoperative Complications Following Endoscopic Pituitary Surgery.
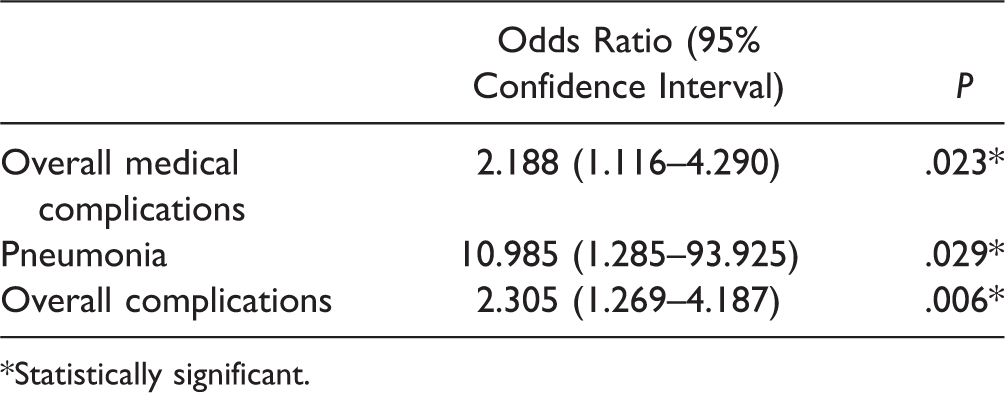
*Statistically significant.
Results
A total of 810 patients who underwent EPS were identified from NSQIP between 2005 and 2013. Patients without BMI data were excluded and a total of 789 patients were included in the final analysis. Of these, 382 (48.4%) were classified as obese (BMI ≥ 30) and 407 were classified as nonobese.
Demographics and Comorbidities
Statistical analysis of the demographics (Table 1) demonstrated that the obese patient population was more likely to be within the 41- to 60-year age-group (44.0% vs 36.4%, P = .029), while the nonobese group was more likely to be greater than 80 years of age (4.7% vs 1.8%, P = .026). A higher percentage of obese patients were white when compared to the nonobese group (63.6% vs 54.1%, P = .013). There were no significant differences in other races or in gender between the two cohorts.
When looking at comorbidities (Table 1), the obese population was significantly more likely to have diabetes (22.8% vs 8.4%, P < .001), dyspnea (7.9% vs 3.7%, P = .012), and hypertension requiring medication (56.0% vs 37.3%, P < .001). Similarly, the obese cohort had a significantly higher percentage of patients within the ASA class 3 and class 4 classifications (66.5% vs 45.6%, P < .001).
Postoperative Outcomes
Upon analysis of postoperative outcomes (Table 2), we determined that the obese patients were more likely to suffer overall complications (10.2% vs 4.9%, P = .005). Upon more specific inquiry, we can see that obese patients had higher rates of surgical (3.7% vs 1.5%, P = .068) and medical (7.6% vs 3.9%, P = .027) complications, although the elevation in surgical complications is not statistically significant. When analyzing specific medical complications, it was shown that obese patients had significantly increased rates of pneumonia (1.8% vs 0.2%, P = .033). There were no significant differences among the other medical complications or between any of the specific surgical complications.
Upon analysis of other postoperative outcomes (Table 2), we can see that pituitary surgery on obese patients is associated with prolonged operating time (154.8 min vs 141.0 min, P = .011) and nonsignificant elevations in length of stay (5.1 days vs 4.2 days, P = .133). Obese patients similarly had elevated rates in mortality (1.6% vs 0.7%, P = .328), reoperation (3.8% vs 3.7%, P = .928), and unplanned readmission (5.2% vs 4.9%, P = .837); however, none of the differences were statistically significant.
Logistic Regression
Binary logistic regression (Table 3) controlling for age, gender, race, and the four statistically significant comorbidities (diabetes, dyspnea, hypertension, and ASA class) shows that obesity is an independent predictor of the previously mentioned significant outcomes: overall medical complications (odds ratio [OR] 2.188, P = .023), pneumonia (OR 10.985, P = .029), and overall complications (OR 2.305, P = .006).
Discussion
Pituitary tumors constitute 10% to 15% of all intracranial tumors and are diagnosed over 10,000 times each year in the United States. 19 Currently, EPS is considered to be a relatively safe treatment option for pituitary tumors with an overall mortality rate of 0.24% and low risk of complications. 20 Although many studies have focused on the efficacy of EPS, few have assessed the impact of patient characteristics on surgical outcomes.
BMI is a universally accepted measure used to define and quantify obesity.21–23 When the classification was first defined, it was used to differentiate death rates above a certain normal cutoff point and has been closely associated with risk of mortality.
Obesity has a significant impact on mortality and has been linked to numerous comorbidities known to impact surgical outcomes.24–26 These comorbidities can lead to higher rates of serious hospital-acquired complications (HACs) related to wound healing, deep vein thrombosis/PE, and UTI. 27 Postoperative complications have been found to be the strongest indicator of increasing healthcare cost and a major economic burden on the healthcare system.28,29 Furthermore, policies set by the Center for Medicare and Medicaid Services allow hospital providers to be financially penalized when patients experience certain HACs. 30 Thus, identifying risk factors associated with, as well as finding treatment options that may reduce postoperative complications, is imperative.
Our study uses the ACS-NSQIP database to examine the effect of obesity on the postoperative outcomes of EPS as a treatment for pituitary lesions. To our knowledge, this study is the first to explore the relationship between BMI and postoperative complications in EPS on a large, multi-institutional scale.
Obese patients were found to have higher overall rates of complications after EPS. However, when stratified into medical and surgical complication type, the increase in medical complications remained significant (7.6 vs 3.9%, P = .27), whereas the increase in surgical complications was not significant (3.7 vs 1.5%, P = .068). Previous studies have also demonstrated increased medical complication risk in the obese patient population. Safaee et al. confirmed reports that obesity is an important risk factor for thromboembolic events after meningioma resection. 31 Studies have also shown significant risk of MI, UTI, and hemorrhage in obese patients compared with nonobese patients undergoing noncardiac surgery. 32 However, in this study, these trends in complications were not implicated in EPS.
Although the obese cohort experienced a greater percentage of overall medical complications as compared to the nonobese cohort, a more detailed analysis of the various possible medical complications showed that only the incidence of pneumonia was statistically increased. This increased incidence of pneumonia in the obese cohort remained significant even after accounting for significant comorbidities including diabetes, dyspnea, and hypertension (OR 11, 95% confidence interval 1.29–93.9). These results are consistent with those in previous studies. A study by Baik et al. examining the association of age and lifestyle factors with pneumonia also showed that obese patients have a higher risk of developing pneumonia, a leading cause of mortality in hospitalized patients and worldwide.33,34 Obesity has been often accompanied by conditions such as gastroesophageal reflux disease, obstructive sleep apnea, diabetes, and asthma, all of which are associated with increased incidence of aspiration and community-acquired pneumonia.35–38 In addition, excess adiposity around the thorax, under the diaphragm, and within the abdomen contributes to decreased chest wall compliance, which favors postoperative pneumonia and atelectasis. 39 Interestingly, obesity has also been associated with increased survival advantage in hospital-acquired pneumonia40–42—a phenomenon known as the “obesity paradox” coined to describe the inverse relationship between obesity and mortality.43–45 Nie et al. point to more aggressive treatments for obese patients, adipose tissue release of soluble tumor necrosis factor-α receptors, and decreased levels of C-reactive protein as possible explanations for this paradox. 46 In our study, no significant differences were found between the obese and nonobese study groups for postoperative mortality (1.6 vs 0.7%), which may be related to the paradoxical survival advantage of obesity during pneumonia infection.
A significant difference was found in total operating time between the obese and nonobese groups (154.8 ± 79.3 vs 141.0 ± 73.6, P =.011). Traditionally, increased BMI has been associated with increased total operating time.47–52 Stevens et al. suggest that impaired monitoring, hemodynamic lability, and positioning difficulties may contribute to increased operation time in neurotological and otological procedures, and that large shoulders and relatively short neck in the obese habitus could increase the technical difficulty of any procedure. 53 This could also explain the lengthened operating time of EPS in obese patients. In addition, EPS patients are usually fitted with image guidance hardware, and adjustment of the gear may be hindered by the aforementioned factors.
The increased risk of surgical complications with increased BMI has been implicated across many surgical specialties. Increased incidence of wound infections in obese patients undergoing cardiac surgery,54,55 open and minimally invasive surgical treatment of endometrial cancer, 56 as well as cervical endocrine surgery has been demonstrated. 16 The association of obesity with microvascular impairment and poor wound healing may contribute to these higher rates of surgical wound complications.57,58 However, our study demonstrated that those with increased BMI undergoing EPS did not experience an increased incidence of surgical complications. This could be explained by the minimally invasive nature of the procedures, which require smaller incisions and less damage to the soft tissue.17,59
The perioperative outcome of those with increased BMI undergoing EPS is much better, with fewer complications than those with increased BMI undergoing other surgical procedures such as coronary artery bypass graft, endometrial cancer resection, and thyroid and parathyroid surgery. Although our study demonstrated that obese EPS patients are at increased risk of postoperative pneumonia and experience longer operation times, we found that these factors had no significant effect on the overall mortality rate. Therefore, EPS remains a safe surgical approach for the treatment of pituitary lesions in those with increased BMI.
This study is not without limitations. Although the WHO classifies obesity using BMI, it may not reflect true obesity, which could be better marked by waist-to-height ratio or waist circumference.60–64 Call for alternative measurements of general and abdominal obesity in ACS-NSQIP has been noted in previous studies. 65 There are biases inherent to ACS-NSQIP and any retrospective data analysis, mainly selection bias and the inability to adjust for confounding variables. This analysis only includes patients treated at hospitals voluntarily participating in ACS-NSQIP and may not be representative of other hospitals not participating in data collection. Because of the limited number of participating hospitals, a relatively low number of patients undergoing EPS were identified, which may not reflect the commonality of this procedure and may reduce the power of the study. Furthermore, ACS-NSQIP is primarily a general surgery database, and this could also contribute to the lower than expected number of EPS. Due to the nature of the database, rates of complications typical after pituitary surgery, such as CSF leak, DI, and SIADH, are not available, which causes potential for limited validity. There is also no follow-up beyond 30 postoperative days of initial operation, which limits our ability to assess any long-term effects of EPS beyond this period. Intraoperative events are not available on the database, and thus we were unable to assess the role of such events in the outcome of EPS. In addition, variables such as size and type of tumor (secreting vs nonsecreting) are unavailable in NSQIP and could have significantly impacted the outcome of the analyses, especially considering the increased risk of pneumonia identified in our study.
Despite these limitations, the ACS-NSQIP is a large, multi-institutional database which provides standardized definitions for patient characteristics and clinical outcomes and allows for the analysis of robust clinical data that have been audited for inter-rated reliability. 66 The results of this study demonstrate that patients with BMI greater than 30 kg/m2 are more likely to suffer medical complications following EPS, specifically pneumonia, but that they did not have a statistically significant increase in risk of surgical complications. EPS in the obese cohort was also associated with increased total operating time but did not impact morbidity or mortality, length of hospital stay, reoperation rate, or readmission rate. Therefore, EPS remains a safe surgical approach for the treatment of pituitary lesions in those with increased BMI. Preoperative modification of patient risk factors and careful planning of perioperative management is essential in reducing operating times and improving outcomes in obese patients.
Conclusion
EPS is a safe surgical approach in patients with BMI greater than 30 kg/m2. The increase in medical complications and total operating time seen in the obese cohort did not significantly influence mortality or contribute to length of hospital stay, reoperation, or readmission rates. Patient education remains important for the obese patient, with discussion regarding these additional complication risks. The role of obesity should be considered in the perioperative management of the patient.
Footnotes
Authors’ Note
This article was presented as an oral presentation at the 2017 Triological Society Combined Sections Meeting, New Orleans, LA, on January 19–21, 2017.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.