
Abstract
Background
The partial cutting and suture technique is a modification of the cutting and suture technique that overcomes the limitations and simplifies the procedure of the cutting and suture technique.
Objective
We describe the partial cutting and suture technique and evaluate its effectiveness of correcting caudal septal deviation.
Methods
We retrospectively reviewed the medical records of patients who underwent anterior septoplasty using the partial cutting and suture technique. The patients were evaluated with the Nasal Obstructive Symptoms Evaluation (NOSE) scale scores and the acoustic rhinometry preoperatively and 3 months postoperatively.
Results
Thirty-one patients underwent caudal septoplasty by our novel technique. The NOSE scale score changed from 43.5 to 11.0 (P = .000). The minimal cross-sectional area (MCA) on the convex side changed from 0.49 cm2 to 0.65 cm2 (P = .006).
Conclusion
The partial cutting and suture technique is relatively easy and is very effective in correcting caudal septal deviation without any complications.
Introduction
Septoplasty is a common surgery in otolaryngology—head and neck surgery. Usually, it can be easily performed by any otolaryngologist; however, some cases might be very difficult, even for an expert. In some cases, septoplasty involves simple excision of the focal septal deviation; however, if there are severe deviations in the caudal and/or dorsal septum, which constitute the L-strut, extracorporeal septal reconstruction may also be required.
Several procedures to correct caudal septal deviation have been introduced; however, the perfect procedure has not yet been determined. Extracorporeal septoplasty is very effective in patients with severe caudal septal deviation, even in combination with a deviated nose.1,2 However, it is very time-consuming and needs an open rhinoplasty incision to make a new L-strut extracorporeally.
The cutting and suture technique is also very useful in patients with moderate-to-severe caudal septal deviation. 3 It can be used to shorten the length of the deviated caudal septum for affixing it in the middle of the nose. However, this procedure is also very time-consuming and has a few limitations. The most notable limitations are that overlapping of both cut edges can reduce the height of the nasal tip and that the septum might be very thick when a batten graft is added.
The partial cutting and suture technique is a modification of the cutting and suture technique that overcomes the limitations and simplifies the procedure of the cutting and suture technique. In this study, we describe the partial cutting and suture technique and evaluate its effectiveness.
Patients and Methods
Patients
The study was approved by the Institutional Review Board of the Ulsan University Hospital, South Korea. We retrospectively reviewed the medical records of patients who underwent anterior septoplasty using the partial cutting and suture technique between June 2015 and April 2017.
The patients who underwent other combined nasal procedures, such as polypectomy, adenoidectomy, endoscopic sinus surgery, etc., which can affect the Nasal Obstructive Symptoms Evaluation (NOSE) scale scores or the results of acoustic rhinometry were excluded. Profile photos of the patients were taken preoperatively to identify the occurrence of nasal saddling or tip dropping.
Surgical Techniques
A hemitransfixion incision was made 1–2-mm behind the anterior margin on the concave side of the anterior septum. After elevation of the mucoperichondrial flap of the incision side, the deviated septal bone and cartilage were selectively removed, preserving an at least 1.5-cm-long L-strut. An incision was made obliquely at the most curved portion on the caudal L-strut in the anteroposterior direction using a No. 15 blade. An anterior margin of about 2 mm was preserved without incision (Figures 1 and 3). Using a Freer elevator, the mucoperichondrial flap on the other side was partially elevated through an incision on the L-strut.
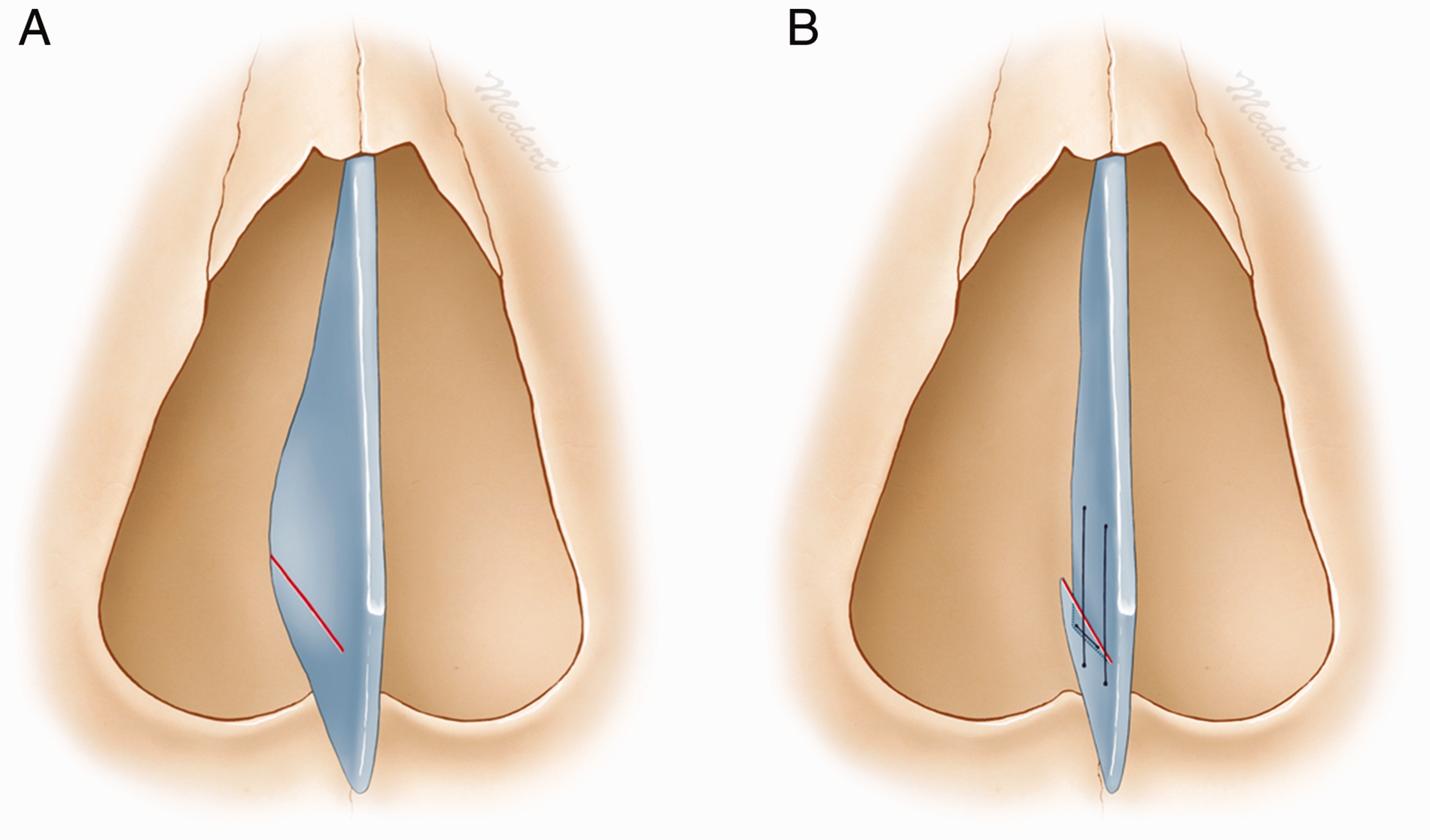
A, Illustration of the deviated caudal septum. Partial cutting was performed horizontally, preserving 2 mm of the anterior margin intact (red line). B, The 2 cut ends were overlapped, and 2 vertical sutures and 1 horizontal suture were applied in the midline. (For interpretation of the references to colours in this figure legend, refer to the online version of this article).
Two vertical sutures (5-0 polydioxanone sutures; Figures 2 and 3) were applied over the middle of the cut edges and then the posterior portion of the L-strut. This shortened the length of the curved caudal septum through overlap of the cut edges, enabling its affixation in the middle of the nose (Figure 2). These sutures ran from the lower part of the cut caudal strut under the elevated mucoperichondrial flap on the concave side to the opposite side of the convex nasal cavity. The needle entered at the same point at which it exited and exited just above the site from under the mucosal space. It reentered at the upper point in the convex nasal cavity and then tied in the concave side (Figure 4). Then, a horizontal suture was applied on the overlapping edges of the septum to prevent extensive overlap with time (Figure 3). This was initiated in the anterior portion and was buried under the mucosa in the same manner as for vertical sutures. After confirmation of straightening of the caudal septum and widening of the nasal cavity, the hemitransfixion incision was closed with 5-0 Vicryl Rapide.
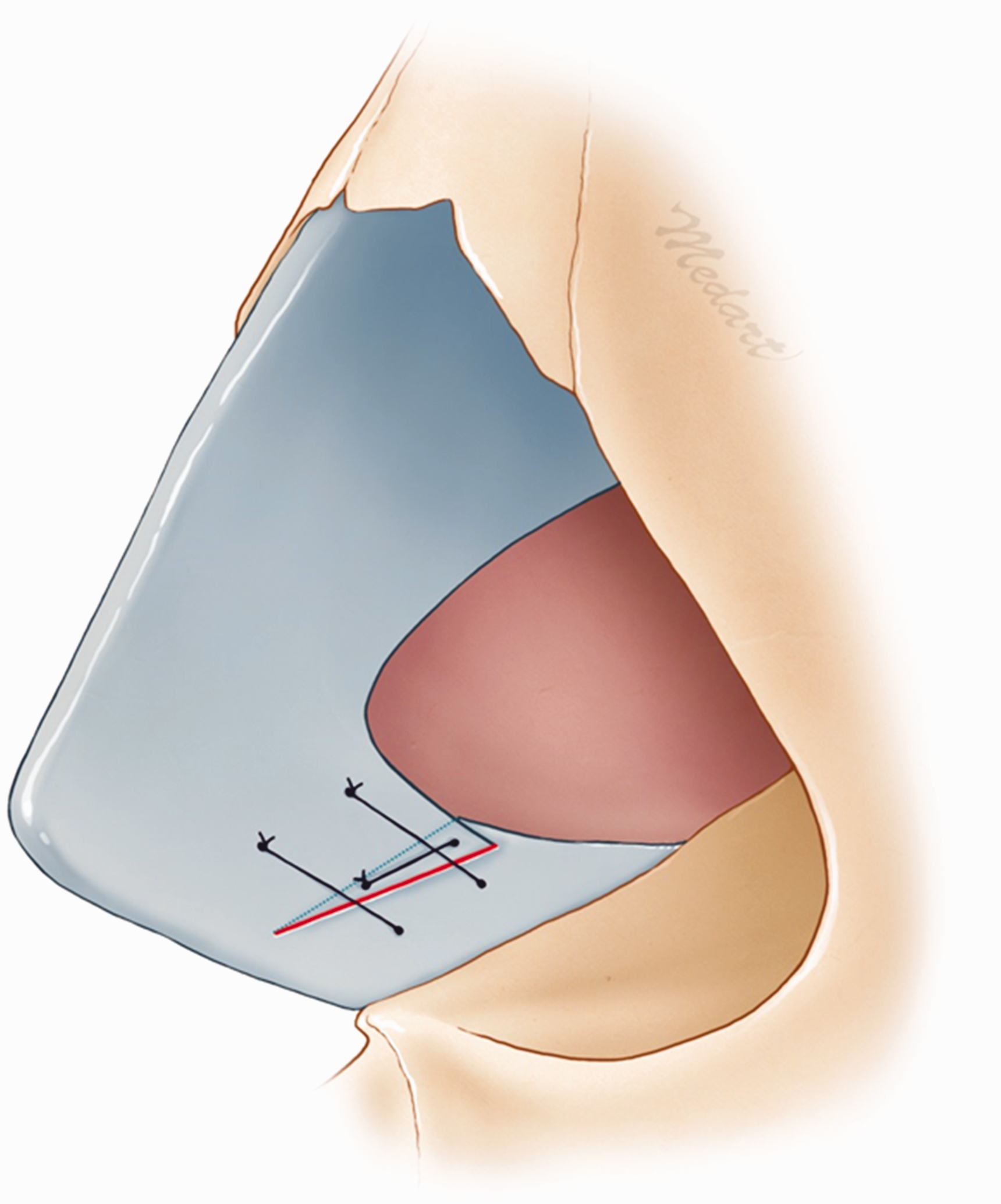
Sagittal view of the cut and overlapped septum. Two vertical sutures in the middle and posterior portion of the L-strut and 1 horizontal suture on the overlapped septum were applied.
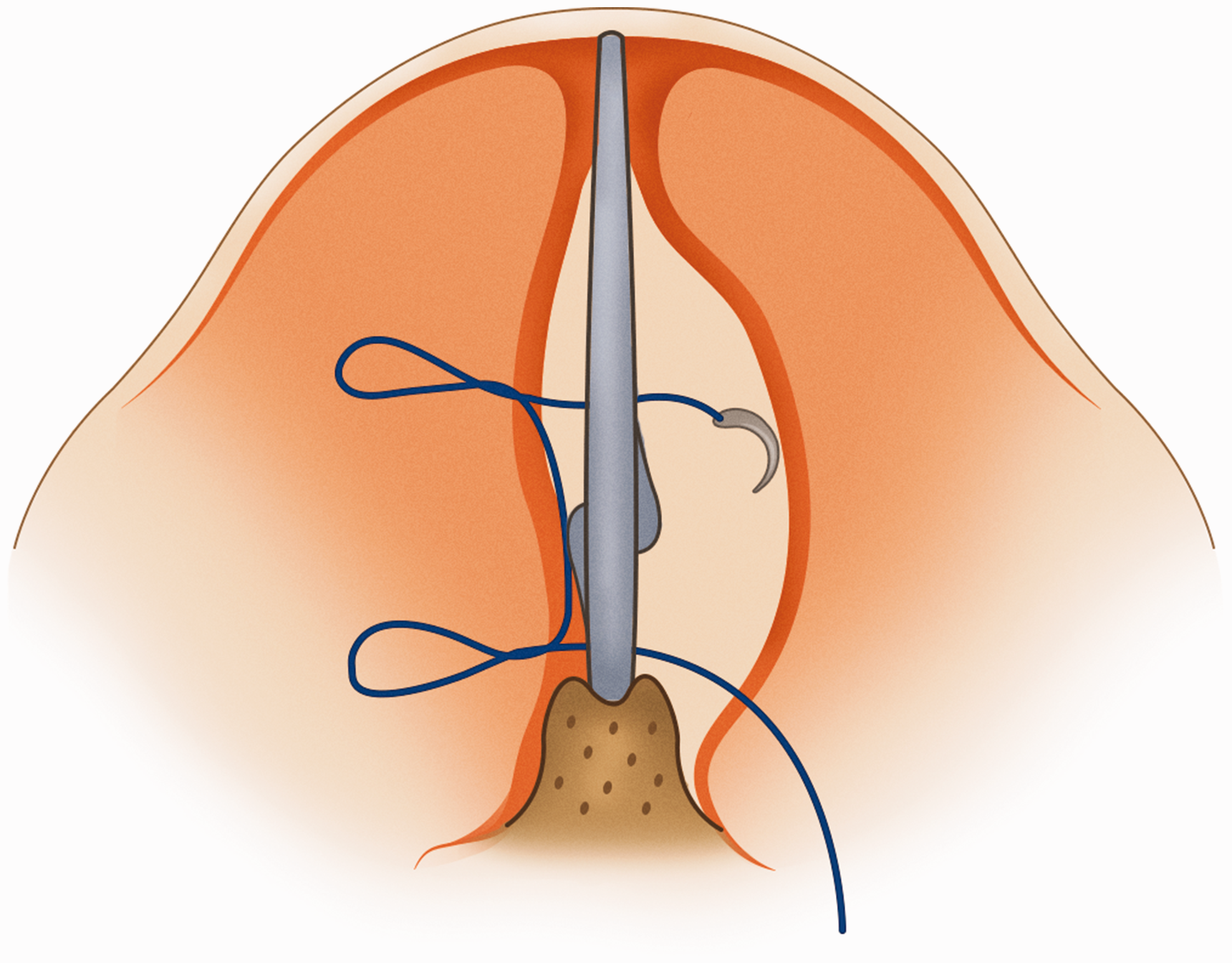
Illustration of the buried suture. All sutures were buried to prevent crust formation and suture loosening.
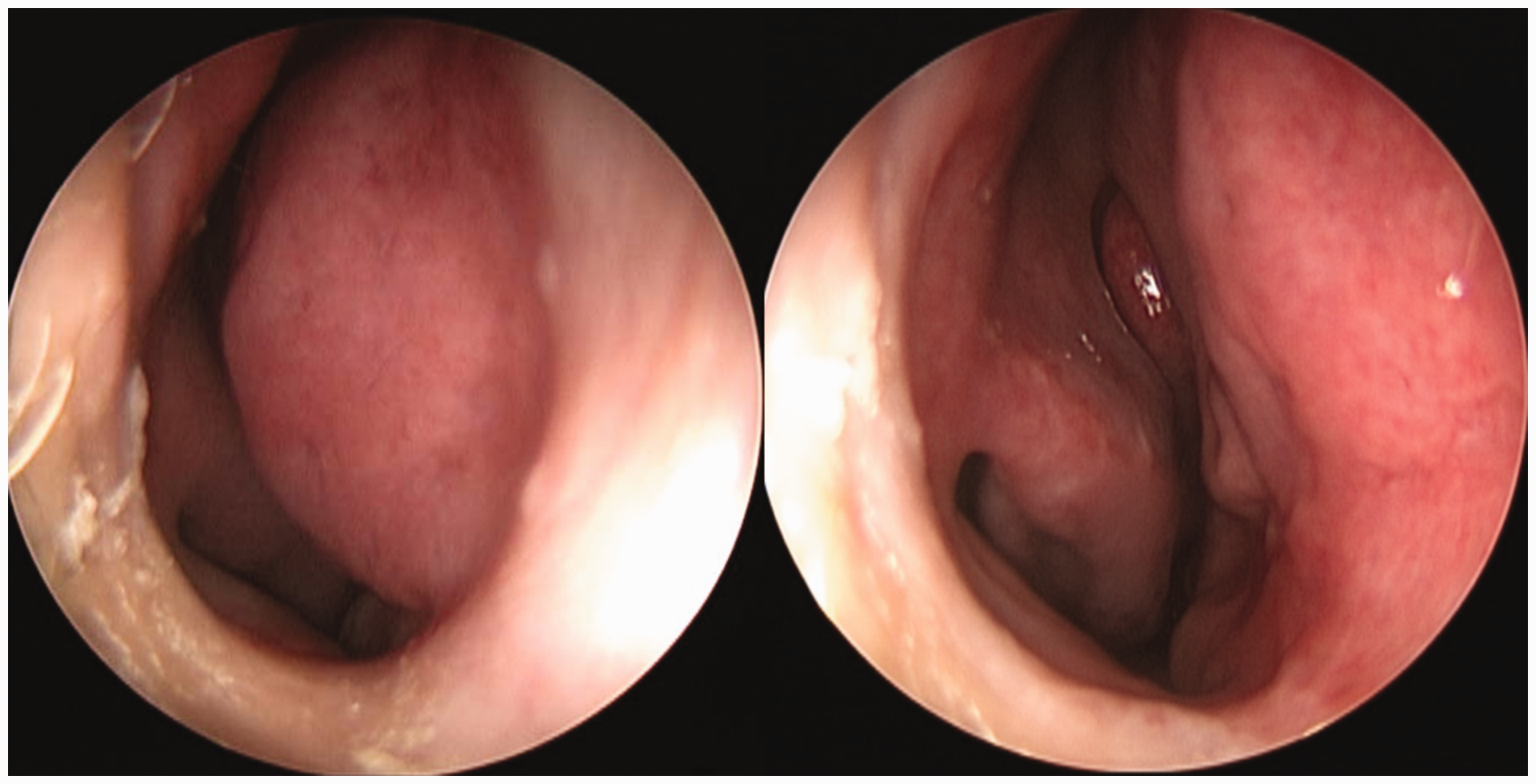
Pre- and postoperative photographs of the caudal septal deviation.
Statistical Analysis
A paired t test was used for statistical analysis. We compared the preoperative and 3-month postoperative Korean version NOSE scale scores and the results of acoustic rhinometry.
Results
Thirty-one patients (25 males, 6 females; mean age: 36.5
Discussion
Caudal septal deviation can be corrected by repositioning the caudal septum in the midline of the nose after reducing its length. Extracorporeal septoplasty is an effective method to shorten and straighten the curved septum in patients with severely deviated noses.1,2 However, it can cause dorsal instability in the keystone area. Anterior septal reconstruction (ASR) is a good modification of extracorporeal septoplasty. It preserves the dorsal strut to preserve the dorsal support in the keystone area.4,5 Furthermore, it also needs to be performed using the external rhinoplasty approach.
In cases of caudal deviation without nasal deviation, resection of the excessive cartilage at the bottom of the maxillary crest is often performed. The anchoring suture technique to pull and fix the resected posterior caudal strut at the anterior maxillary spine soft tissue can be used, in addition to ensuring that the septum is located on the midline.6,7 However, the septum can slip from the midline of the maxillary crest when the suture loosens or the soft tissue stretches out, which can lead to undercorrection of the deviated septum, persistent nasal obstruction, or even a saddle nose.
The cutting and suture technique is an excellent method to correct a caudal deviation, which maintains stability between the caudal septum and maxillary crest. The most deviated portion of the caudal septum is cut horizontally and overlapped to reduce its length. Then the overlapping cartilages are sutured at the midline of the nose. 3 This technique has several drawbacks. First, suturing at the posterior portion while maintaining the exact midline position is not easy. Second, the septal batten graft, which is often used in combination with the overlapped cartilage for more support, can make the caudal septum too thick at the overlapped portion. Finally, the overlapping caudal ends can cause slight tip lowering in patients without a deviated nose.
The partial cutting and suture technique focuses on how to perform caudal septoplasty easily and effectively. Preserving about 2 mm of the caudal end can prevent nasal tip lowering and make suturing easy. Mucoperichondrial flap elevation through partial cutting site can aid in septal movement to midline, removing soft tissue memory. Two vertical sutures can straighten the septum with maximal overlapping of the upper and lower cut ends at the midline. The horizontal suture avoids the development of a saddle nose, as overlap at the posterior caudal cut end continues with time. An additional batten graft is not needed for straightening and support. All sutures were buried sutures, thus preventing crust formation and loosening of the sutures in the nasal cavity.
The partial cutting and suture technique has 2 limitations. It is not useful if the caudal septum is displaced from the maxillary crest. If the bone-cartilage connection at the maxillary crest is not in the midline, we often use a batten graft on the other side or in the midline. It is also not suitable for patients with a deviated nose along with caudal septal deviation. In these cases, the caudal outline is not in the middle and thus the deviated caudal septum should be cut completely. ASR is preferred in such cases.
Conclusion
The partial cutting and suture technique is relatively easy and is very effective in correcting caudal septal deviation without tip lowering and nasal-valve narrowing. Further study is needed to evaluate the long-term results of this technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.