
Abstract
Background
Cone-beam computed tomography (CBCT) is a fast imaging technique with a substantially lower radiation dosage than conventional multidetector computed tomography (MDCT) for sinus imaging. Surgical navigation systems are increasingly being used in endoscopic sinus and skull base surgery, reducing perioperative morbidity.
Objective
To investigate CBCT as a low-radiation imaging modality for use in surgical navigation.
Methods
The required field of view was measured from the tip of the nose to the posterior clinoid process anteroposteriorly and the nasolabial angle to the roof of the frontal sinus superoinferiorly on 50 consecutive MDCT scans (male = 25; age = 17–85 years). A phantom head was manufactured by 3-dimensional printing and imaged using 3 CBCT scanners (Carestream, J Morita, and NewTom), a conventional MDCT scanner (Siemens), and highly accurate laser scanner (FARO). The phantom head was registered to 3 surgical navigation systems (Brainlab, Stryker, and Medtronic) using scans from each system.
Results
The required field of view (mean ± standard deviation) was measured as 107 ± 7.6 mm anteroposteriorly and 90.3 ± 9.6 mm superoinferiorly. Image error deviations from the laser scan (median ± interquartile range) were comparable for MDCT (0.19 ± 0.09 mm) and CBCT (CBCT 1: 0.15 ± 0.11 mm; CBCT 2: 0.33 ± 0.18 mm; and CBCT 3: 0.13 ± 0.13 mm) scanners. Fiducial registration error and target registration error were also comparable for MDCT- and CBCT-based navigation.
Conclusion
CBCT is a low-radiation preoperative imaging modality suitable for use in surgical navigation.
Keywords
Introduction
Chronic rhinosinusitis is a common condition with a prevalence of 10.9% in Europe, 1 which is routinely managed with complex endoscopic endonasal surgery (EES). 2 Preoperative imaging, typically multidetector computed tomography (MDCT), plays a vital role in the diagnosis of sinonasal pathology and is further used to guide surgical navigation systems.
Surgical navigation systems display the tracked position of surgical instruments on preoperative imaging, to help surgeons identify anatomical landmarks and pathological targets, reducing perioperative morbidity. 3 Surgical navigation systems are becoming increasingly common in otolaryngology theatres worldwide,4,5 with 94.6% of otolaryngologists reporting access to such systems in a 2010 survey of the American Rhinologic Society. 5
Cone-beam computed tomography (CBCT) is a fast, office-based imaging modality with a significantly lower radiation dosage than conventional MDCT, providing a dose reduction of 40% to 70% for sinus imaging.6,7 In summary, CBCT involves the emission of X-rays from an X-ray tube that is rotated around the patient opposite to a detector to collect an isotropic volume of data, which can be assembled into both multiplanar and 3-dimensional (3D) reconstructions. CBCT images provide high spatial resolution, which allows good visualization of submillimeter bony structures comparable to high-resolution MDCT. 8 In addition, CBCT scanners are cheaper than MDCT scanners, which in combination with their office availability, provides a more cost-effective imaging option for use in otolaryngology clinics. 9
However, considerable variation exists in the specifications of commercially available CBCT systems. 10 Otolaryngology surgeons must be aware of the CBCT specifications required for surgical navigation. Obvious requirements of preoperative imaging for surgical navigation are for it to include all relevant anatomical structures in its field of view and to be geometrically accurate. Currently, uncertainty exists regarding the adequacy of the field of view 11 and geometric accuracy12–15 of commercially available CBCT systems. Finally, surgeons need to be confident that the navigation accuracy of CBCT-based versus MDCT-based surgical navigation systems is comparable.16,17
This study aims to provide a technical evaluation of the suitability of CBCT-based surgical navigation for EES and to highlight the required specifications for CBCT systems to be used for this purpose.
Materials and Methods
The algorithm of this technical evaluation is outlined in Figure 1. In summary, this study evaluates 2 possible limitations of 3 commercially available CBCT systems: field of view and geometric accuracy, before assessing the compatibility of these 3 CBCT systems with 3 commercially available surgical navigation systems by measuring their fiducial registration error and target registration error.
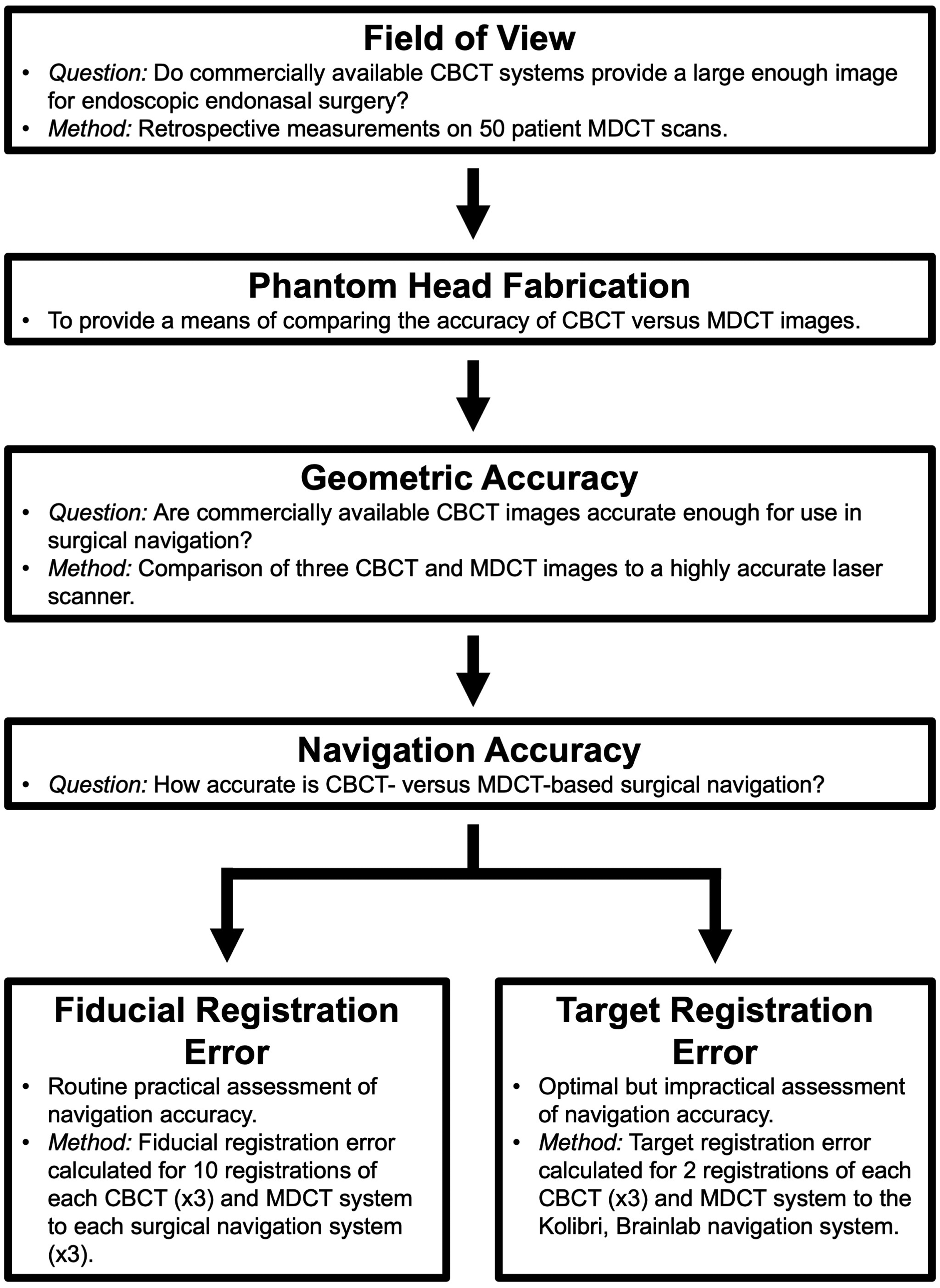
A flowchart of the algorithm of this technical evaluation of CBCT-based surgical navigation. CBCT, cone-beam computed tomography; MDCT, multidetector computed tomography.
Field of View
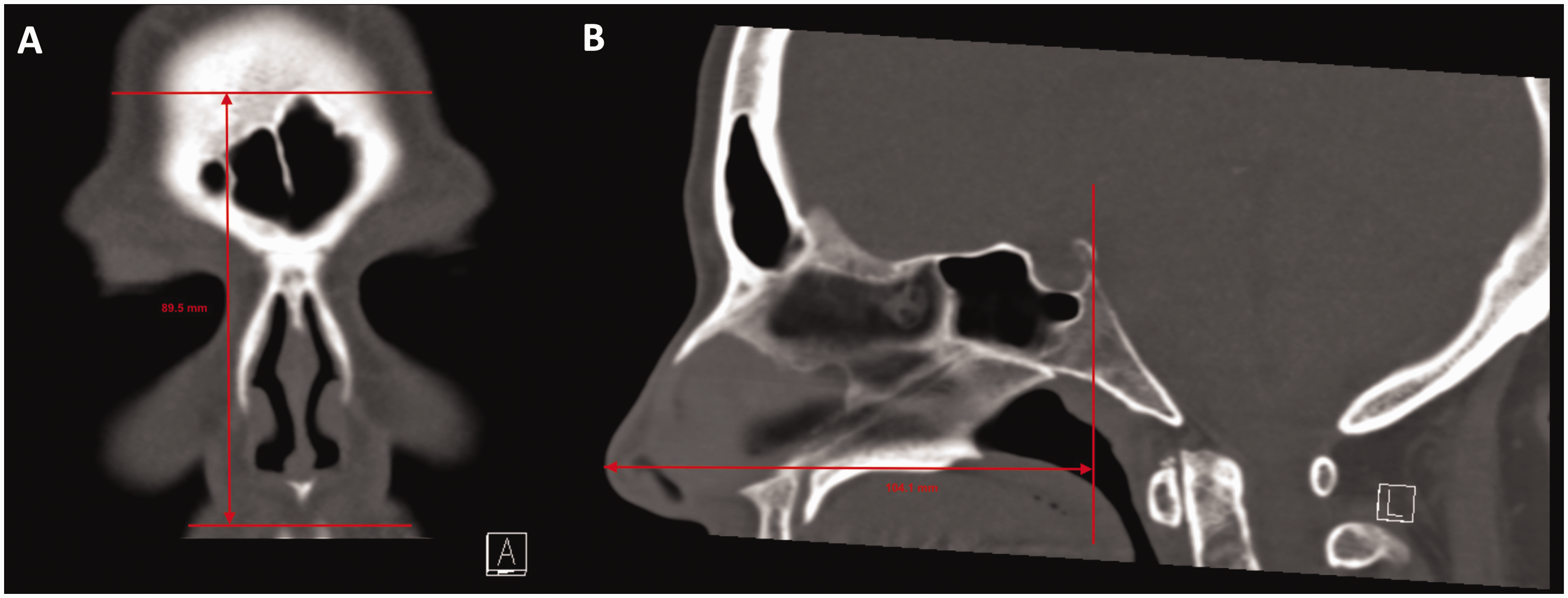
The minimum required field of view for EES on the sinuses and anterior skull base was investigated by measurements on 50 sequential MDCT sinus scans (1 mm slice thickness) requested by the ENT Department of the Queen Elizabeth Hospital Birmingham, between January and December 2017 (male = 25, age = 17–85 years; Figure 2). The required anterior–posterior distance was defined from the tip of the nose to the posterior clinoid process. The required superior–inferior distance was measured from the nasolabial angle to the roof of the frontal sinus.
Figure 2. The measurements used to define a minimum field of view for endoscopic endonasal surgery on the sinuses and anterior skull base, shown on a MDCT scan: (A) anterior-posterior distance, measured from the tip of the nose to the posterior clinoid process and (B) superior-inferior distance, measured from the nasolabial angle to the roof of the frontal sinus.
Phantom Head Fabrication
A phantom head with a radiodensity equivalent to skin was designed and manufactured by 3D printing. Ten MDCT scans of the head (male = 5; age = 20–80 years) requested by the Queen Elizabeth Hospital Birmingham ENT department in January 2017 were reviewed. The radiodensity of the skin was measured at 5 sites per scan using the syngo FASTview (Siemens, Munich, Germany) density tool: over the nasal bridge, right and left supraorbital regions, and right and left cheek. The mean density of skin of the head was 54.93 (±27.25) HU. The literature was searched for published radiodensities of rapid prototyping materials; polylactic acid was the thermoplastic polymer found with a radiodensity closest to that of skin of the head (66.34 ± 14.58 HU). 18
An MDCT scan was taken of an EES surgical trainer kit (Karl Storz, Tuttlingen, Germany). Image data were exported as DICOM files to Mimics v19 (Materialise, Leuven, Belgium). Radiodensity thresholding allowed isolation of the skin layer of the head, which was exported as a stereolithography file to Freeform (Geomagic, Morrisville, NC, USA) to add a posterior wall and 90 surface divots (2 mm diameter by 2 mm depth). Figure 3 shows the final phantom head design, which was 3D printed (Prusa, i3, Prusa Research, Praha, Czech Republic).

The stages of the deviation analysis between the highly accurate laser scan and CT data. A, The stereolithography file of the laser scan was defined as the reference index. B, The CT scan data were converted from DICOM data to stereolithography format. C, The CT scan and reference index were crudely aligned (prealignment). D, The CT scan and reference index were accurately superimposed and deviations were measured at 56 consistently visible points.
Computed Tomography
Three CBCT scanners were evaluated in this study: the CS9300 (Carestream Health, New York, NY, USA), 3D Accuitomo 170 (J Morita, Osaka, Japan), and 5G (NewTom, Verona, Italy). These CBCT scanners will be referred to as CBCT 1, CBCT 2, and CBCT 3, respectively. The 3 CBCT scanners were compared to a 64-slice MDCT scanner, SOMATOM Definition AS (Siemens, Munich, Germany). CBCT scans were performed according to each scanners’ standard sinus protocol with its maximum field of view (Table 1). MDCT scans were taken with the standard navigation protocol used at the Queen Elizabeth Hospital Birmingham: 80 mAs, 120 KV, 15.3 s, and 1 mm slice thickness.
CBCT Sinus Scanning Protocol Used in This Study.

Abbreviations: CBCT, cone-beam computed tomography; FOV, field of view.
Geometric Accuracy
The geometric accuracy of CBCT and MDCT scans was evaluated by comparison to a highly accurate laser scanner (FARO Quantum S, FARO, Lake Mary, FL, USA), accurate to 0.025 mm. 19 CBCT and MDCT scans were converted from a DICOM file to a stereolithography file (InVesalius v3, RTI Renato Archer, Campinas, Brazil) and then compared to the laser scan using an industrial inspection software (GOM inspect, GOM mbH, Braunschweig, Germany; Figure 3).
Surgical Navigation Systems
Three surgical navigation systems were used in this study: (1) Kolibri (Brainlab, Munich, Germany), (2) NAV3i (Stryker, Kalamazoo, MI, USA), and (3) StealthStation S7 (Medtronic, Minneapolis, MN, USA). Each surgical navigation system has its own patient tracker, which was attached securely to the phantom before registration could begin. All 3 surgical navigation systems offer a range of registration techniques including paired-point touching and surface matching. Optical tracking and paired-point registration was used in this study to allow comparison between the surgical navigation systems. The same 5 fiducial points across the temporal and frontal regions of the phantom were used for registration of each of the surgical navigation systems. Five fiducials were used for registration, as previous work has demonstrated that the use of more fiducials does not significantly improve target registration error. 17
Navigation Accuracy
Fiducial registration error
Fiducial registration error is the distance between matched fiducials in image and physical space following registration. 20 It is commonly displayed by commercial surgical navigation systems following registration, representing a routine and practical assessment of navigation accuracy. The phantom head was registered 10 times to all 3 surgical navigation systems used in this study with scans from the MDCT scanner and 3 CBCT scanners being studied. The fiducial registration error of each registration was recorded, and navigation accuracy was qualitatively assessed by touching pits on the phantom surface.
Target registration error
Target registration error is the best measure of registration accuracy, representing the overall accuracy of the navigation system. 17 It is the distance between matched points, other than registration fiducials, in image and physical space after registration. 20 However, the lack of well-defined landmarks in clinical imaging makes it difficult to calculate, remaining confined to academic assessments of navigation accuracy in phantom models. In this study, target sites were printed to have a 2 mm diameter, to ensure a close fit with the tracked pointer tool. A single optical surgical navigation system (Kolibri, Brainlab, Munich, Germany) was used to assess the target registration error of MDCT- versus CBCT-based surgical navigation for the scanners studied in this project, as a proof of principle of the comparable accuracy of CBCT and MDCT images. A surgical plan was prepared for each CT scan using iPlan Cranial 3.0 (Brainlab, Munich, Germany), the center of 56 surface divots were selected as target landmarks, 5 of which were used to register the phantom to the navigation system by paired-point matching. The head phantom was registered to the surgical navigation system using MDCT and CBCT scans, and the target registration error identifying 51 consistently visible preplanned surface landmarks was measured twice for each scan.
Statistics
Statistics were carried out using GraphPad Prism 7. Significance level was determined at the level of alpha <.05. The error deviation from the highly accurate laser scanner of the 3 CBCT scanners studied was compared to that of MDCT by a Friedman test with Dunn’s multiple comparison testing. The measured target registration errors were compared using a 1-way analysis of variance test, with an uncorrected Fisher’s least significant difference test for multiple comparisons of the 3 CBCT scans to MDCT. A Bonferonni adjustment was calculated for multiple comparisons of the 3 CBCT scanners to MDCT (α =.05/3 = .017).
Results
Field of View
The required dimensions of the field of view for EES on the sinuses and anterior skull base (mean ± standard deviation, range) were measured anteroposteriorly (107 ± 7.6 mm, 106.1–120.1 mm) and superoinferiorly (90.3 ± 9.6 mm, 73.1–114.8 mm).
This measured minimum required field of view for EES on the sinuses and anterior skull base was compared to the field of view provided by the 3 CBCT scanners used in this study (Table 1). All measured anteroposterior and superoinferior distances fitted within the maximum field of view sizes provided by these 3 CBCT scanners.
Geometric Accuracy
The median (±interquartile range) of the error deviation measured at 56 predefined points on 3 sequential scans was 0.19 (±0.09) mm for MDCT, 0.15 (±0.11) mm for CBCT 1, 0.33 (±0.18) mm for CBCT 2, and 0.13 (±0.13) mm for CBCT 3 (Figure 4). The error deviation of CBCT 1 (P = .0996) and CBCT 3 (P = .0256) was not significantly different to that of MDCT. However, the error deviation of CBCT 2 was significantly higher than MDCT (P < .0001).
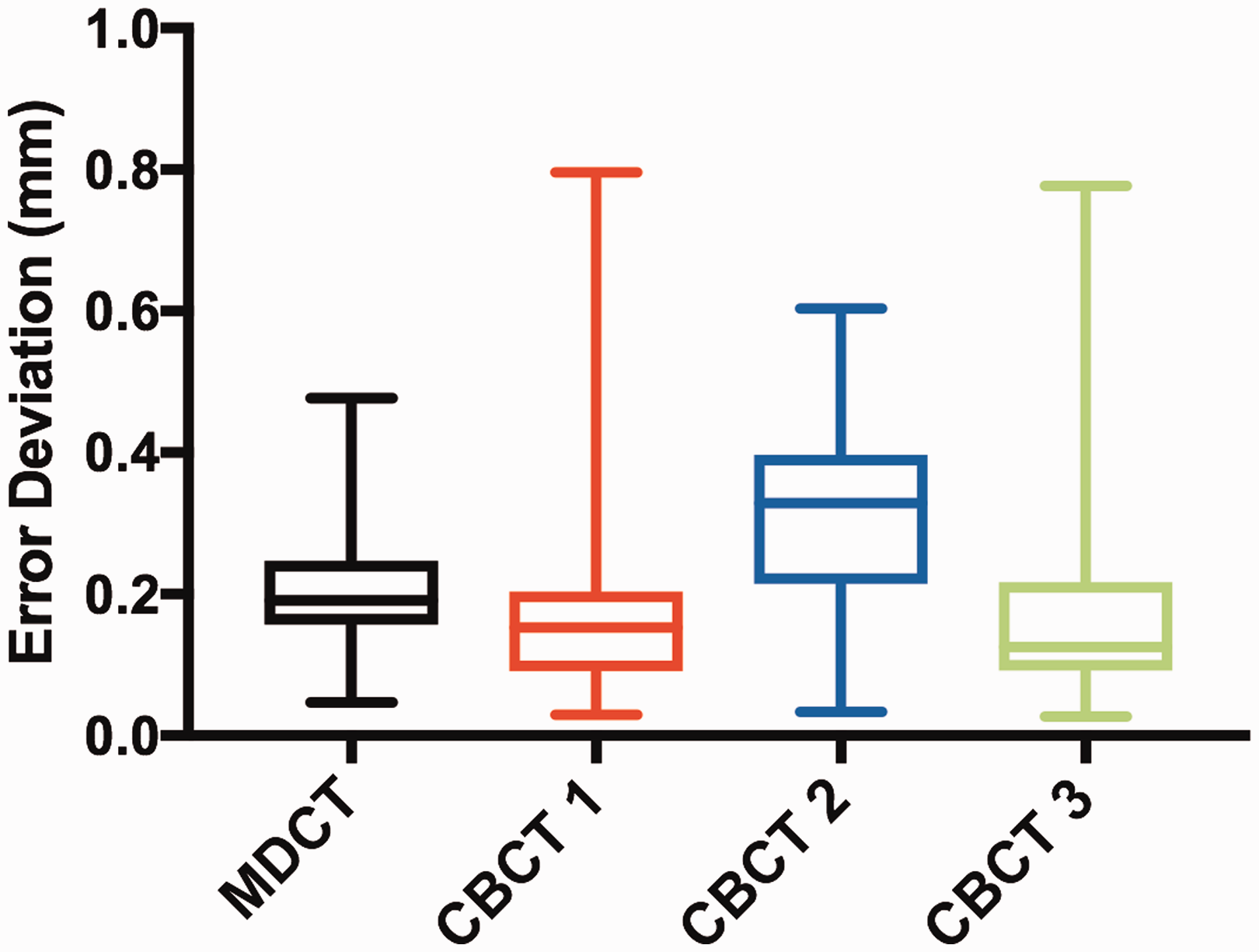
A graph of the error deviation of MDCT and CBCT scans compared to a highly accurate laser scanner, measured at 56 predefined points on 3 sequential scans. CBCT, cone-beam computed tomography; MDCT, multidetector computed tomography.
Navigation Accuracy
Fiducial registration error
Fiducial registration error was recorded for 10 registrations of the phantom head to 3 surgical navigation systems by paired-point touching of 5 fiducials using optical tracking (Table 2). All registrations using MDCT and CBCT scans were accepted as a “good” accuracy by the surgical navigation systems, allowing surgical navigation to begin, and were qualitatively accurate.
Fiducial Registration Error of MDCT- and CBCT-Based Registration to 3 Surgical Navigation Systems, Calculated From 10 Sequential Registrations (Mean ± Standard Deviation).
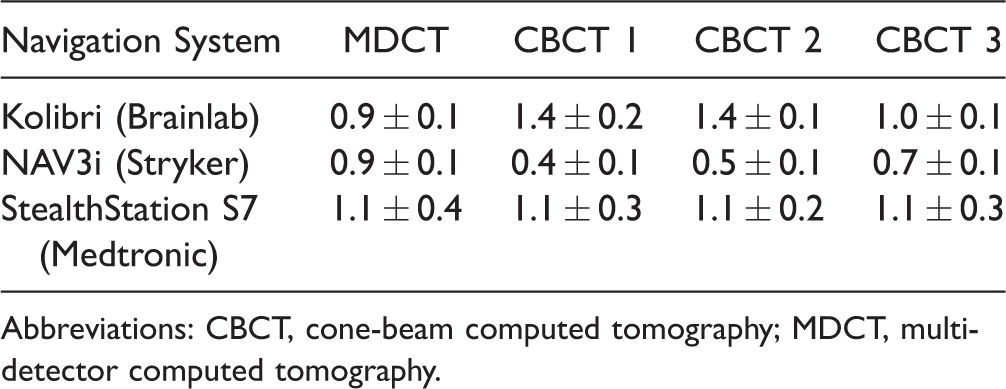
Abbreviations: CBCT, cone-beam computed tomography; MDCT, multidetector computed tomography.
Target registration error
The mean (±standard deviation) target registration error, measured at 51 preidentified landmarks for 2 registrations, was calculated as 1.07 (±0.35) mm for MDCT, 0.95 (±0.21) mm for CBCT 1, 1.17 (±0.31) mm for CBCT 2, and 0.89 (±0.27) mm for CBCT 3 (Figure 5). CBCT 3 provided a significantly lower target registration error than MDCT (P = .0024), while the target registration error using CBCT 1 (P = .0372) and CBCT 2 (P = .0749) was not significantly different from MDCT.
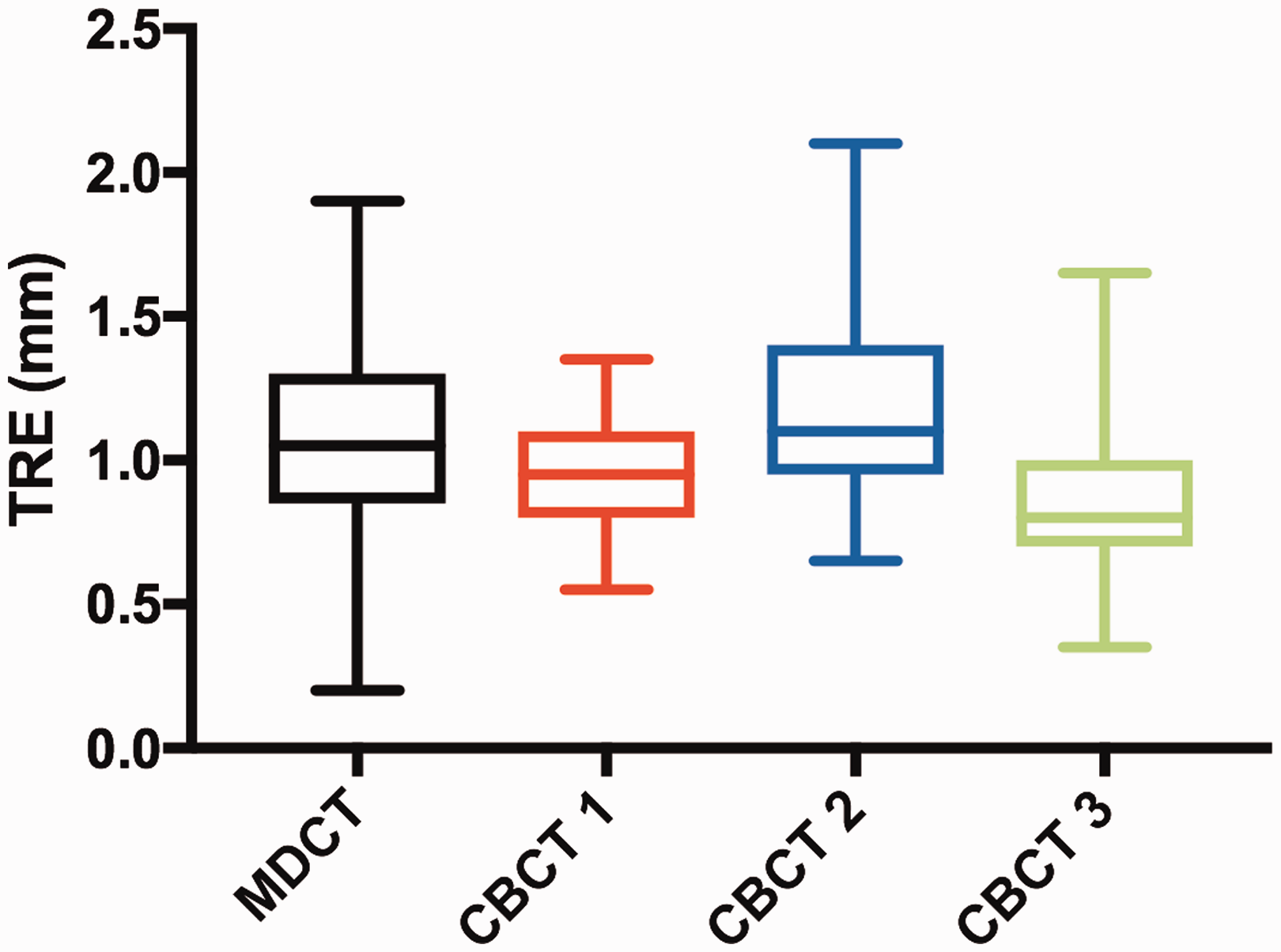
A graph of the target registration error of MDCT- and CBCT-based surgical navigation, measured over 51 predefined points using an optical surgical navigation system (Kolibri, Brainlab, Munich, Germany). CBCT, cone-beam computed tomography; MDCT, multidetector computed tomography; TRE, target registration error.
Discussion
Field of View
For a preoperative scan to be used for surgical navigation, it must show all the anatomical landmarks of interest for the procedure within its field of view. The 3 commercially available CBCT scanners investigated in this study provided a field of view that is sufficient for EES on the sinuses and anterior skull base, based on the minimum field of view measurements made in this study.
The minimum anteroposterior dimension was defined as the distance from the tip of the nose to the posterior clinoid process of the sphenoid bone. The minimum superoinferior dimension was defined as the distance from the nasolabial angle to the roof of the frontal sinus. The whole surface of the nose was included in the image, as it is required for patient-to-image registration by surface matching. The posterior clinoid process defines the posterior border of the sella turcica, ensuring the transsellar approach to the pituitary gland is visible. Pituitary adenomas are the most commonly encountered anterior skull base pathology, making up 49.8% of anterior skull base surgery cases, 21 demonstrating a key potential use of CBCT. Adequate visualization of the frontal recess is essential for functional endoscopic sinus surgery on the frontal recess, which is classified as an advanced procedure and is often aided by the use of surgical navigation systems. 22
Geometric Accuracy
All of the CBCT and MDCT scanners were deemed highly accurate; median error deviations ranged from 0.13 to 0.33 mm relative to a highly accurate laser scan. The error deviations of CBCT 1 and 3 were not significantly different from that of MDCT, although their means were slightly lower. The accuracy of CBCT 2 was significantly lower than that of MDCT, although its mean error deviation was only 0.138 mm greater, which is not clinically significant.
This study adds weight to a previous study showing that CBCT scanners can have an equivalent geometric accuracy to MDCT scanners, 14 supporting the suggestion that CBCT systems have a suitable geometric accuracy for use by surgical navigation systems. However, as in other studies, there was variation in the accuracy of different CBCT systems. 12 It may be of value for centers to independently evaluate the accuracy of their CBCT system, using the highly accurate approach demonstrated in this study, so that they may start to utilize it for surgical navigation.
This study is the first to have used the novel technique of determining image accuracy outlined by Wilmowsky et al. 23 to compare the accuracy of CBCT and MDCT scans. This technique involves using industrial inspection software to superimpose the CBCT or MDCT scan being evaluated onto data from a highly accurate laser scan and to measure deviation between the 2 data sets. This allows a 3D assessment of spatial accuracy of the CT scan, which is more appropriate than the 2D measurements made with digital calipers in previous studies.12,24,25
Navigation Accuracy
Fiducial registration error
CBCT scans from all 3 scanners evaluated provided a comparable fiducial registration error (<1.4 mm) and qualitative accuracy to MDCT, demonstrating their compatibility with 3 commercially available surgical navigation systems. Although fiducial registration error is only a crude measure of navigation accuracy, it is the measure routinely reported by surgical navigation systems to allow surgeons to assess the accuracy of patient-to-image registrations in combination with qualitative assessments before their use intraoperatively.
Target registration error
The mean target registration error for CBCT-based surgical navigation varied between 0.89 and 1.17 mm for the 3 CBCT systems evaluated, which was equivalent to or better than the measured target registration error of MDCT-based surgical navigation. In this study, the mean target registration error of MDCT- and CBCT-based surgical navigation was <2 mm, which has been suggested as the minimum accuracy required for surgical navigation systems to be clinically useful during surgery. 26 This builds on evidence from a previous study that CBCT- and MDCT-guided surgical navigation systems are of comparable accuracy. 16 However, only surface level targets were used in this study, which may not be representative of deeper sinus structures.
Target registration error is the best available measure of the registration accuracy of surgical navigation systems. 20 The comparable target registration error of CBCT- and MDCT-based navigation strengthens our finding of comparable fiducial registration error between the 2 imaging modalities.
Image Quality
In addition to the geometric accuracy of the preoperative imaging modality, the utility of surgical navigation also depends on its image quality. An advantage of CBCT images is their good visualization of bony structures comparable to MDCT, a limitation is their inferior soft tissue resolution.6,8
Interestingly, a retrospective review of 57 patients with sinonasal polyposis and 90 patients with normal radiological findings, reported CBCT to have significantly superior image quality in individuals without polyposis and significantly worse in those with polyposis. 27 Image quality was assessed by grading the visibility of bony structures. Although extensive soft tissue swelling in sinonasal polyposis reduced the visibility of bony structures in CBCT images, the image quality was still deemed adequate to assess patients. 27 Thus, although CBCT images provide excellent visualization of bony structures, they are not appropriate for patients suspected of having primarily soft tissue pathology such as sinonasal tumors, mucoceles, or encephaloceles. 6
A retrospective review evaluated the number of sinonasal abnormalities that would be missed in patients with rhinosinusitis receiving CBCT sinus scans opposed to MDCT scans by evaluating bone-windowed MDCT images as simulated CBCT images. 28 After reviewing 361 patient images, it was concluded that only 3.3% of sinonasal abnormalities would be missed, which would have altered patient management in 1.1% of cases. 28 Thus with careful selection of patients, CBCT imaging offers an appropriate lower radiation imaging modality for sinus scanning.
Conclusion
Commercially available CBCT devices provide a sufficient field of view to assess sinus and anterior skull base pathology. In addition, CBCT scans have comparable geometric accuracy to MDCT images, allowing image-to-patient registration by surgical navigation systems with an accuracy equivalent to or better than MDCT. Thus, CBCT presents a viable alternative to MDCT for accurate surgical navigation during EES on the sinuses or anterior skull base, with a substantially lower radiation dose than conventional MDCT. However, CBCT images are of more limited use when assessing primarily soft tissue diseases, and many CBCT scanners do not allow the use of radiological contrast.
Footnotes
Acknowledgments
The authors would like to thank Cavendish Imaging, the Westbourne Centre, Autodesk, and Adriana Anastasio at the Queen Elizabeth Hospital for their assistance in this project.
Authors’ Note
This study was presented at a scientific meeting BACO International 2018, Manchester Central, Manchester, UK, July 4–6, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.