
Abstract
Background
Despite the well-appreciated variability in sphenoid sinus anatomy, there are no documented cases of retrosphenoid cells in the literature to date.
Objective
This study defines and determines the prevalence of retrosphenoid cells as identified on computed tomography (CT) imaging and intraoperative endoscopy and reviews the prevalence of other related anatomical variants of the sphenoid sinus.
Methods
Retrospective study of 300 random noncontrast sinus CT scans of patients with chronic rhinosinusitis presenting to a tertiary rhinology center. All identifiable anatomic variations and any presence of retrosphenoid cells and their pneumatization patterns were recorded. The prevalence of various anatomic variations of the sphenoid sinus was also calculated.
Results
A total of 300 sinus CT scans were included in the study. Protrusion of both the internal carotid artery (42.6%) and optic nerve (19.7%) into the sinus was more prevalent than the dehiscence of either one. A retrosphenoid cell was identified in 2% of CT scans. Other anatomic variants were less prevalent.
Conclusion
Meticulous review of preoperative imaging is key in identifying rare and complex sphenoid cell variations in planning surgical approaches and potential treatment strategies for the unusually pneumatized sphenoid air cells. Various manifestations of sinus disease can be localized to this area, and suspicion of a retrosphenoid cell should be raised in patients presenting with recalcitrant headache.
Keywords
Introduction
The sphenoid sinuses are asymmetrically paired, measure approximately 2.2 cm in height, width, and anteroposterior diameter in the adult human, with a 3% incidence of inflammation. 1 The natural ostium of the sphenoid sinus is located superoanteriorly on the face of the sphenoid sinus and opens into the sphenoethmoid recess, medial to the superior turbinate. The mean distance of the sphenoid ostium from the nasal sill is 66 mm, and the mean distance of the posterior wall of the sphenoid from the sphenoid ostium is 14 mm.2,3 Infective organisms causing inflammation within the sphenoid are predominantly viral, bacterial, and/or fungal. Isolated involvement of the sphenoid sinus is rare. The most common presenting symptoms of sphenoid sinus disease are headaches and visual disturbances. Functional endoscopic sinus surgery for sphenoid sinusitis is complicated both by the considerable variability in sphenoid sinus anatomy and the relationship of the sphenoid sinus to critical surrounding neurovascular structures. 4 On occasion, cranial nerve involvement or intracranial complications can occur due to its proximity to the cavernous sinus and skull base. 5 Preoperative radiological scanning is routinely carried out for diagnosis, and triplanar image guidance systems are often used to evaluate the anatomy and variation within the region. 1 Anatomical variations of the optic nerve and internal carotid artery (ICA) occur as a result of variance in pneumatization of the sphenoid bone.
Retrosphenoid cells, an anatomical variant of the paranasal sinuses, are defined as an air- or tissue-filled cavity that occurs within the sphenoid sinus region, usually identified incidentally on scanning. Retrosphenoid cells are found within the posterior wall of the sphenoid sinus presenting as a space or cavity lying between the sphenoid sinus and the clivus. They lack an appreciable natural drainage pathway connecting it to the sphenoid sinus on all triplanar computed tomography (CT) imaging. These may be asymptomatic or may be a source of symptoms and infection. Due to their anatomic location, infection of these cells can theoretically lead to meningitis, cavernous sinus thrombosis, or even pneumocephalus. 6 Despite the well-appreciated variability in sphenoid sinus anatomy, there are no documented cases of retrosphenoid cells in the literature to date. Our center is the first to identify and describe the retrosphenoid cell.
In contrast, the sphenoethmoid air cells, commonly known as the Onodi air cells, lie superolateral to the sphenoid sinus and are considered part of the ethmoid complex. Variations exist in septation of the sphenoid sinuses along with differing pneumatization, which can affect endoscopic approaches to the sphenoid sinus.7,8
The purpose of this retrospective study was to determine the prevalence of retrosphenoid cells, an atypical anatomic variation of the sphenoid sinus, as identified on CT imaging and intraoperative endoscopy, as well as to study the prevalence of other related anatomical variants of the sphenoid sinus.
Patients and Methods
Patients
This study was a retrospective chart review conducted at St. Paul’s Hospital Sinus Centre in Vancouver, Canada, with approval from the University of British Columbia Research Ethics Board (H18-01068) and did not require patient consent. Individuals eligible for inclusion were patients diagnosed with sinus diseases by endoscopic and CT scan findings. Patients were excluded if they were below 19 years of age, had congenital craniofacial abnormalities, systemic bone disease, previous facial trauma, sinonasal tumor, and sphenoid sinus mucocoele, or diagnosed with cystic fibrosis, primary ciliary dyskinesia, Kartagener’s syndrome, or any improper development of sinus pneumatization.
Methods
A retrospective study of 300 random noncontrast sinus CT scans of patients presenting to the St. Paul’s Sinus Centre with either primary or recalcitrant chronic rhinosinusitis was performed. CT specifications included a slice thickness of 0.5 to 1 mm thick, with images taken in the axial plane and reformatted in the coronal and sagittal planes. Images were reviewed in both bone and soft tissue windows in all 3 planes. All identifiable anatomic variations and any evidence or presence of retrosphenoid cells and their pneumatization patterns were recorded.
Results
Three hundred eighty CT scans were reviewed; 80 scans met exclusion criteria. A total of 300 CT scans were included in the study. Results are summarized in Table 1. Six cases (2%) of retrosphenoid air cells were seen. Protrusion of both the ICA and optic nerve into the sinus was more prevalent than the dehiscence of either one. Moreover, 42.6% of scans had evidence of ICA wall protrusion. Bilateral protrusion of the ICA was seen in 55 cases (18.3%). In those patients with unilateral protrusion, the left side was more common than the right: 46 cases (15.3%) compared 28 cases (9.3%). Protrusion of the optic nerve was noted in 19.7% of scans, present bilaterally in 22 cases (7.3%), and more on left (7.7%) than on the right side (4.7%). There were no cases of bilateral dehiscence of either the optic nerve or the ICA. The sphenoethmoid (Onodi cells) air cells were mostly superolateral (16.6%) compared to centrally located which were present in only 2.3% of cases. The intersinus septum was central predominantly in 140 of 300 (46.6%) cases with no major preference to the left or right. Two sphenoid sinuses (0.6%) were identified without any septation. When present, most septations started out centrally (46.6%) at the sphenoid face before deviating posteriorly to either side. The sphenoid septum deviated to the left side in 24.7% of cases and to the right side in 27.3% of cases. Pneumatization of the anterior clinoid process is an uncommon variant, present in 17 cases bilaterally (5.7%) with unilateral anterior clinoid pneumatization being more common on the right side (7.3%) compared to 5.3% on the left side. Intraoperatively, we did not identify any obvious fontanelles or other potential drainage pathways of the retrosphenoid cell. It was decided to marsupialize the retrosphenoid cell into the sphenoid sinus due to its anatomic proximity while simultaneously establishing a wide drainage pathway for the sphenoid sinus itself (Figures 1–3).
Summary of Prevalence of Various Sphenoid Anatomic Variants (n = 300).
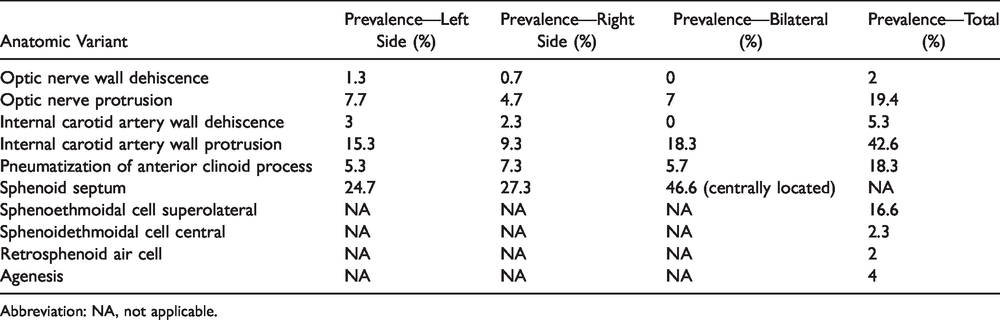
Abbreviation: NA, not applicable.
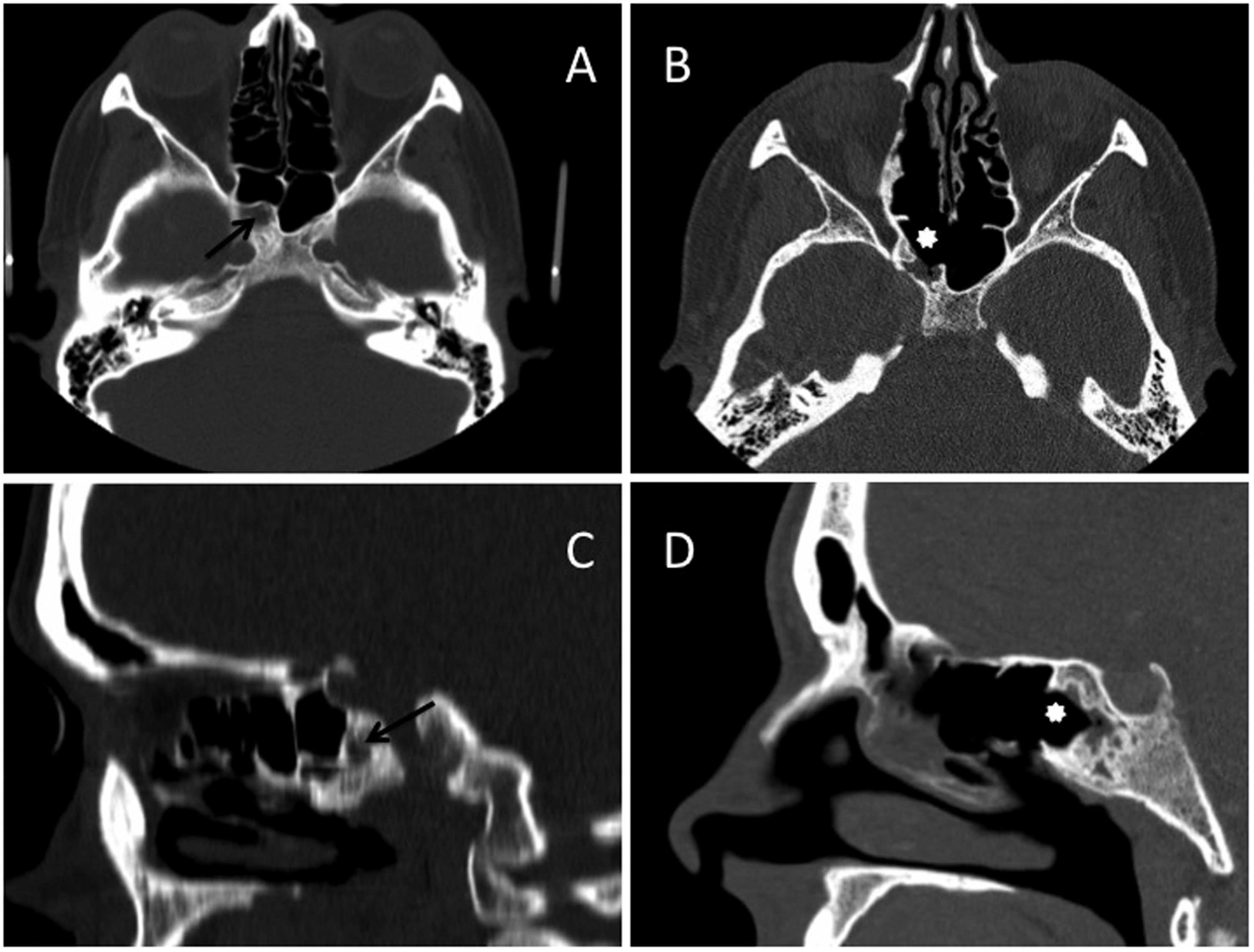
Pre- and postoperative CT images our patient with a retrosphenoid cell. (A) and (C) represent preoperative axial and sagittal scans, respectively. (B) and (D) represent postoperative axial and sagittal scans, respectively. Arrows: retrosphenoid sinus (preoperatively). Stars: retrosphenoid sinus (postoperatively). The anterior wall of the retrosphenoid sinus in (A) and (C) has been removed (B and D) to create a communication with and enable drainage through the sphenoid sinus proper.
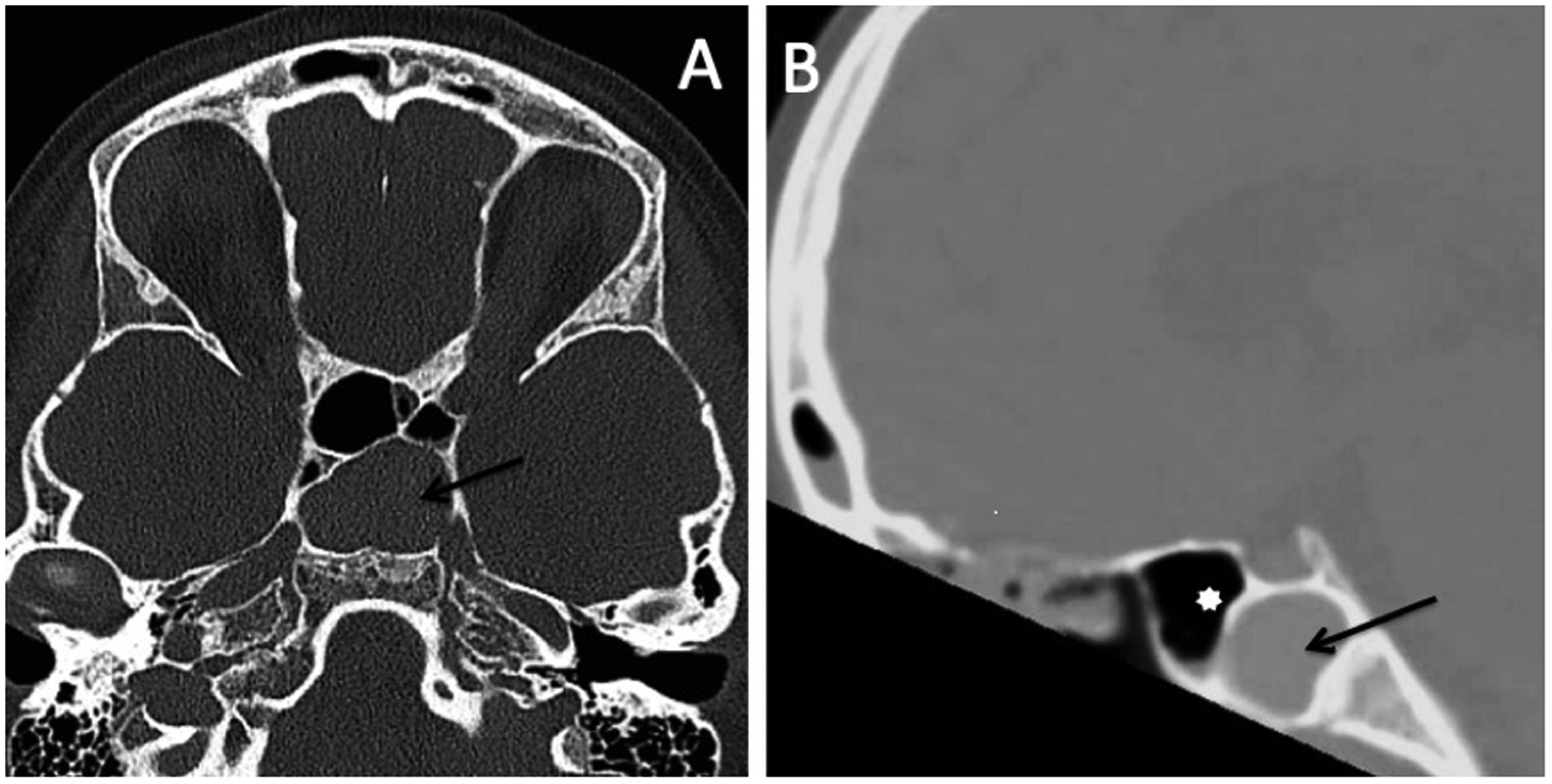
Axial (A) and sagittal (B) views of the opacified retrosphenoid cell in our pediatric patient. Star (B): true sphenoid sinus. Arrows (A and B): opacified retrosphenoid cell. Note that bilateral sphenoid sinuses are clear of disease.
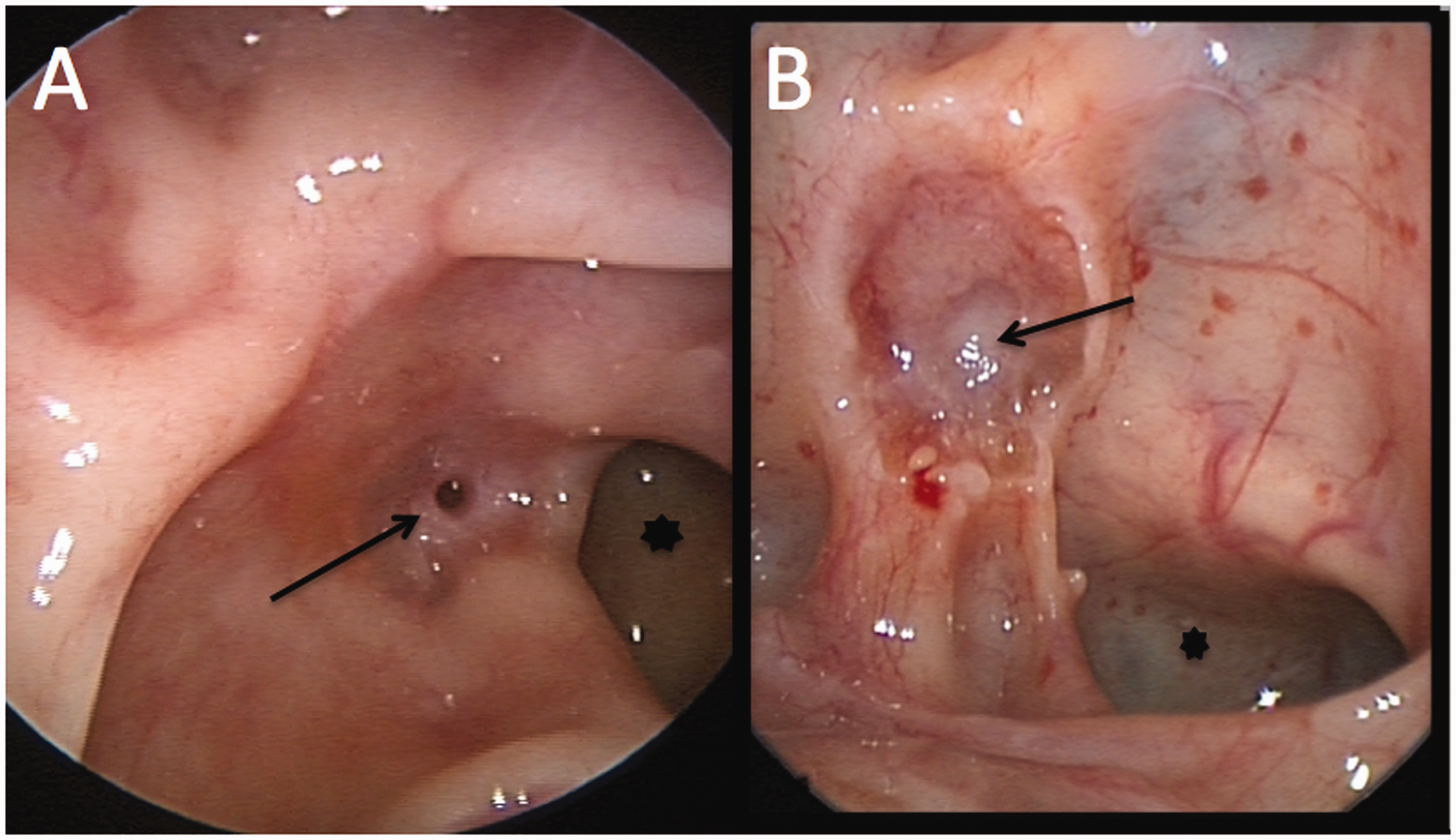
Postoperative endoscopic images of 2 of our patients with retrosphenoid cells. Arrow: retrosphenoid sinus; star: sphenoid sinus proper. A wide communication between the retrosphenoid sinus and the sphenoid sinus proper can be appreciated in both patients.
Discussion
The sphenoid sinus may show varying degrees and directions of pneumatization in each individual, with its various extensions bringing it in close relationship to the cavernous sinus, ICA, optic nerve, frontal lobe, ventral surface of the brainstem, cranial nerves III to VI, and pituitary gland. 9 The pneumatization pattern of the sphenoid region greatly influences the surgical approach for managing disease in this area. The degree of pneumatization depends on the position of the sinus in relation to the sella turcica and has been historically categorized into conchal, sellar, presellar, and postsellar types. 10 The sellar pneumatization type has been the most prevalent among pneumatization types in previous studies, with an average of 80.9% in 11 studies performed on Caucasians and an average of 64.8% in 6 studies performed on Chinese individuals. 11 In most cases, a single intersphenoid septum lies between the 2 sphenoid sinuses. Rarely, however, there is a presence of more than 1 septum (accessory septae). Occasionally, there may even be no septum at all with a single sphenoid sinus occupying the sphenoid pneumatization on both sides. This situation was present in 2 of our patients. The direction of the septa may be transverse, medial, or lateral. The sella turcica may be seen as a prominent bulge in the roof of a well-pneumatized sphenoid sinus. The sphenoid bone may present as nonpneumatized. 12
Anatomic variations of the sphenoid sinus are well documented. The Onodi cell is a posterior ethmoid air cell typically found posterolateral or superiorly (central Onodi cell) to the sphenoid sinus 13 and is in close proximity to at least 1 optic nerve or ICA, leaving a higher risk of complications. The sphenoid sinus is located medially and inferiorly to the Onodi cell. The incidence of Onodi cells as detected by CT scans is commonly cited as 8% to 24%.14–16 Nouraei et al. found that the most common anatomic variant with potential implications for operative safety in their series was pneumatization of the anterior clinoid process. 17 This usually occurs from the most posterior ethmoid cells and can surround the optic nerve, which increases the risk of injury to the nerve during surgery. Nouraei et al., Bolger et al., and Arslan et al. found the prevalence of anterior clinoid pneumatization to be 17.6%, 13.3%, and 6%, respectively.17–19
The sphenoid sinus may develop normally or deviate from the norm and develop accessory ostia. They may present with overpneumatization, underdevelopment, or complete absence. 20 Arrested sphenoid pneumatization has been described as a benign developmental variant where red marrow is replaced by early fatty mucous conversion and often confused with a skull base disease process. 21 Hypoplasia of the sphenoid sinus with a nonaerated segment usually reveals regions with normal trabecular bone. Agenesis of sphenoid sinus is rare and occurs in 1% to 1.5%. 22
Despite the well-appreciated variability in sphenoid sinus anatomy, there are no documented cases of retrosphenoid cells in the literature to date. The retrosphenoid cell is distinguished from an Onodi cell in that it occurs truly posterior to the sphenoid sinus—between the sphenoid sinus and the clivus—and lacks a natural drainage pathway connecting to the sphenoid sinus on all triplanar CT imaging. The presence of a retrosphenoid cell may be an important consideration in those patients presenting with recalcitrant headaches and pain, including patients that have undergone previous sinonasal surgery. Mischaracterization of these cells as sphenoethmoidal air cells (aka Onodi cells) may lead to incomplete surgery, increased risk of intraoperative complications, and ongoing patient symptomatology necessitating revision surgery.
Conclusion
Unrecognized and/or inaccurate diagnosis of anatomic features on CT scan of the sinuses may contribute to difficulties in interpretation, diagnosis, and intervention of sinus disease. The ability to identify and recognize anatomic variations on imaging provides the surgeon with the knowledge to accurately diagnose and treat chronic sinus disease, ultimately improving patient outcomes. This study supports the initiative of meticulous review of preoperative imaging to identify rare and complex sphenoid cell variations in planning surgical approaches and potential treatment strategies for the unusually pneumatized sphenoid air cells. 23 Various manifestations of sinus disease can be localized to this area, and suspicion of a retrosphenoid cell should be raised in patients presenting with recalcitrant headache.
Footnotes
Authors’ Note
This study was presented at the Rhinoworld Meeting on June 5–9, 2019, in Chicago, IL, USA.
Acknowledgments
The authors acknowledge Alysha Rasool, Jamil Manji, and Fahad Alasousi for assistance with protocol development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.