
Abstract
Background
Transpalpebral frontal septectomy (TFS) can be performed for unilateral frontal sinusitis drainage (into the contralateral healthy frontal sinus) or to provide access to the lateral extent of the contralateral frontal sinus. This procedure has demonstrated its usefulness in several problematic situations for the endoscopic surgeon.
Objective
The main objective of our study was to evaluate the feasibility of TFS. Secondary objectives were to define outcomes, early and late complications, contraindications, and failure rates of the TFS.
Methods
We reviewed patient demographics including age and gender, indication for frontal septectomy, prior surgeries, failure rates and necessity of revision surgery, early and late complications, and the side of the approach (ipsi- or contralateral to the frontal sinus pathology). Twenty patients who had undergone TFS were included. Patients were classified into 2 groups according to the surgical indication: group 1—TFS performed for unilateral frontal sinusitis to drain a frontal sinus in the contralateral frontal sinus; and group 2—TFS performed to provide access to the lateral extent of the contralateral frontal sinus. Scarring was assessed using the SCAR-Q questionnaire.
Results
TFS was performed on all patients in Groups 1 and 2 (success rate = 100%). No patients had recurrence of the pathology 6 months after surgery (0%). No patient needed revision surgery (0%). One complication (frontal hypoesthesia) was reported 6 months after surgery. Mean SCAR-Q score was 99.3 ± 2.5 (min = 91/100, max = 100/100).
Conclusion
TFS was feasible for all patients in this study. This procedure permits drainage of the frontal sinus and gives access to the lateral extent of the contralateral frontal sinus, without visible scarring, and with few lasting complications. Authorization to conduct this study was obtained from the Ethical Committee of our institution (APHM, n°2019_65).
Keywords
Introduction
Technological progress over the past 20 years has made available mini-invasive surgical treatment for numerous sinus pathologies, especially with the rise of functional endoscopic sinus surgery.1,2 However, an endoscopic approach to the frontal sinus (FS) remains difficult because of its conformation and relationship with noble organs such as the orbits, the anterior skull base, and the brain. 3
Concerning FS, 2 situations remain problematic for endoscopic surgeons: first, in cases with pathologies affecting the lateral extent of the FS, endoscopic access through the frontal recess is often difficult because of the diameter, the medial position, and orientation of the latter, 4 thus imposing a wide, endoscopic bilateral approach such as the Draf III procedure; second, in cases with chronic unilateral frontal sinusitis due to frontal recess stenosis. These situations can be resolved by frontal septectomy. Endoscopic frontal septectomies preserving the healthy frontal recess (Draf IIc) have been described but require extensive surgical experience. 5 Classic frontal septectomies (Draf III) lead to wide opening of both FS recesses, thus exposing the patient to the risk of bilateral stenosis. Indeed, cases of bilateral frontal filling following Draf III have been reported.6,7 In each of the abovementioned problematic situations, external (transfacial or coronal) approaches make it possible to circumvent these problems. However, they may lead to major aesthetic sequelae (scars, alopecia) affecting patient quality of life. 8
A transpalpebral approach permitting a mini‐invasive and hidden approach to the FS has recently been reported and has shown its relevance in the 2 situations mentioned earlier.9 Indeed, it has been described to perform frontal septectomy providing access to the lateral extent of the contralateral FS, without affecting its recess, unlike other combined techniques described in the literature.10,11 Although this surgical procedure has been fully described, its feasibility and results have not been studied.
The main objective of our study was to evaluate the feasibility of transpalpebral frontal septectomy (TFS) as described by Michel et al. Secondary objectives were to define outcomes, complications, contraindications, and failure rates of TFS.
Materials and Methods
Ethical Standards
All patients gave written consent before participating in the study, which was conducted according to the Declaration of Helsinki. Authorization to conduct this study was obtained from the Ethical Committee of our institution (APHM, n°2019_65).
Population
In this single-center study, all patients who had undergone TFS in our University Hospital were included. Exclusion criterion was age under 18 years. The pathology was considered too lateral to be reached through an endoscopic approach if it was more lateral than a vertical line passing through the infraorbital nerve. Patients were classified in 2 groups according to surgical indication: Group 1: TFS performed for unilateral frontal sinusitis drainage (into the contralateral healthy FS, Figure 1(A)). Preoperative CT scan of patients in group 1 (A) and group 2 (B). A, Patient with recurring frontal sinusitis due to left frontal recess stenosis. B, Frontal osteoma with retention in the lateral extent of the right frontal sinus (arrow). Group 2: TFS performed to provide access to the lateral extent of the contralateral FS (Figure 1(B)).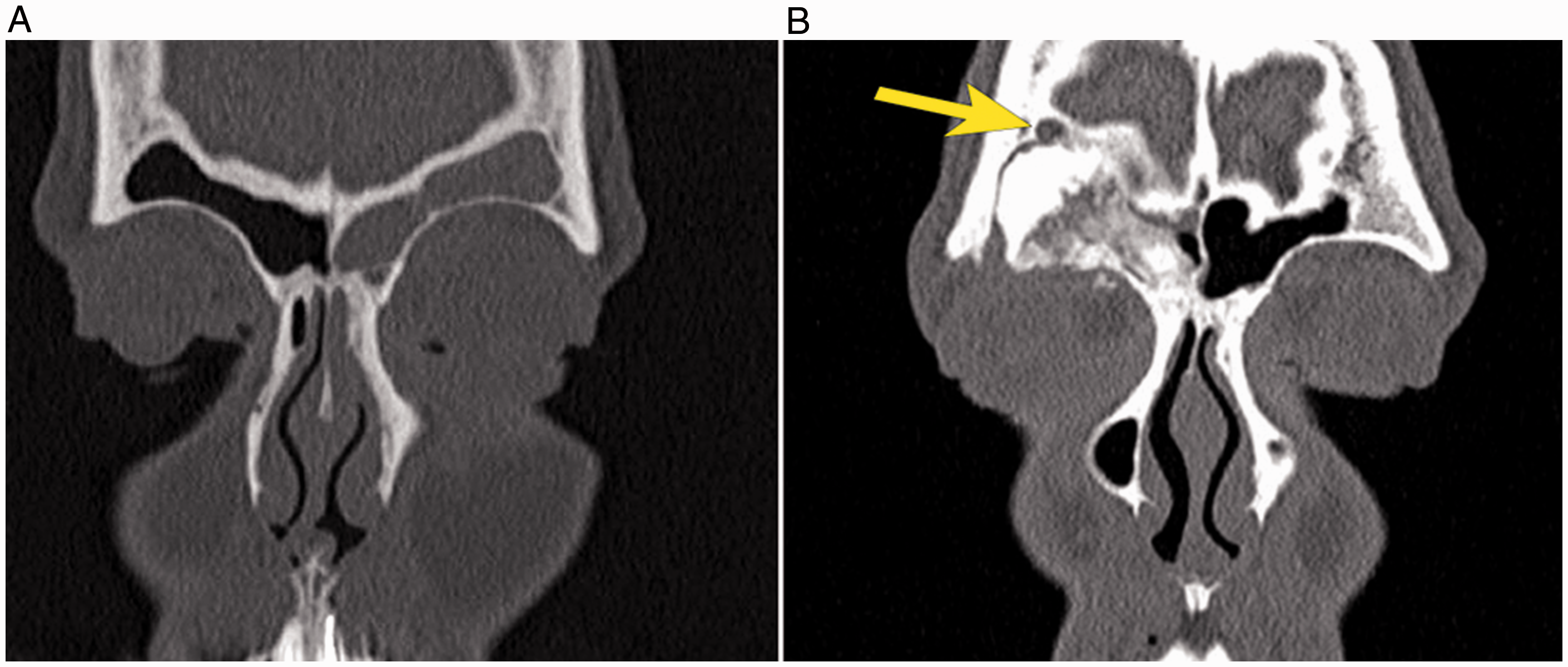
Surgical Procedure
Surgery was systematically performed with navigation (computer-assisted surgery, CAS; Fusion, Medtronic®, Jacksonville, Florida, USA). Surgical steps were described by Michel et al. 9 We used a 30° endoscope and a 3-mm diamond drill. The incision was similar to that for upper blepharoplasty incision. Once the superointernal orbital region is deperiosted, the area to be drilled is monitored by CAS (Figure 2(A)). The sinusotomy is performed by drilling the FS floor (1 × 1 cm; Figure 2(B)). Frontal septectomy was then performed using the diamond drill (Figure 2(C) and (D)). The endoscope stays outside the patient during drilling, thus allowing good maneuverability.
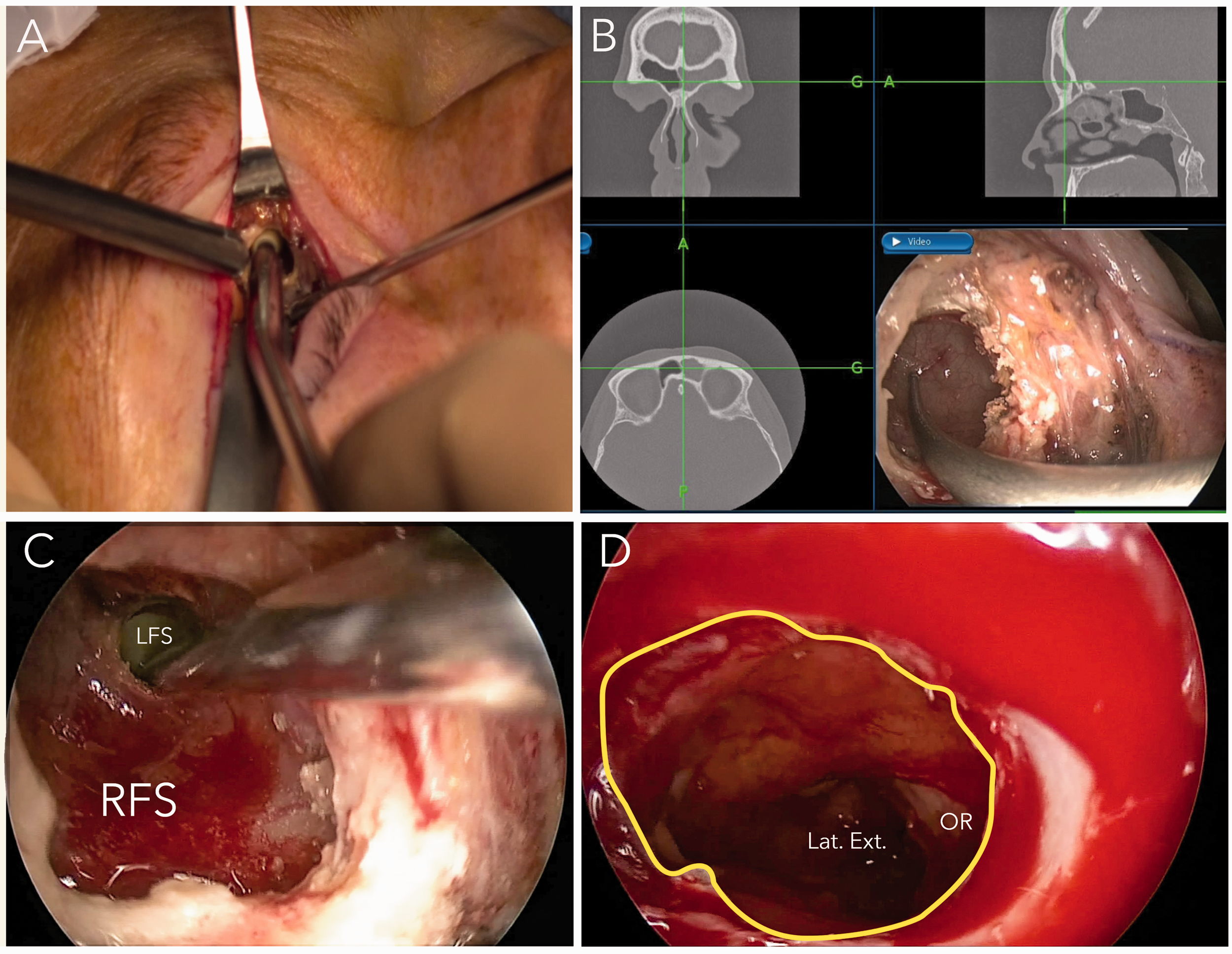
Intraoperative views. A, Sinusotomy with a 3-mm diamond drill. B, Locating the frontal septum using computer-assisted surgery. C, Drilling of the interfrontal septum. D, Endoscopic view of the left frontal sinus through the frontal septectomy (line in yellow). Lat.Ext., lateral extent of the left frontal sinus; LFS, left frontal sinus; OR, orbital roof; RFS, right frontal sinus (For interpretation of the references to colours in this figure legend, refer to the online version of this article).
Data Collection
We reviewed patient demographics including age and gender, indication for frontal septectomy, prior surgeries, failure rates and necessity of revision surgery, early and late complications, and the side of the approach (ipsi- or contralateral to the FS pathology).
Patients were clinically evaluated at days 1 and 10, and months 1, 3, and 6 after surgery. All patients had low-dose millimetric computed tomography (CT) scans preoperatively and 6 months after surgery.
Early complications (appeared within 72 h postoperatively) could be: nasal hemorrhage, orbital hematoma, orbital breach, frontal hypoesthesia, diplopia, and cerebrospinal fluid (CSF) leak. Late complications (still present 6 months after surgery) could be diplopia, frontal hypoesthesia, or scarring problems.
Main Objective
The main objective was to assess the feasibility of the TFS. Feasibility was defined as the ability to remove the intersinus septum.
Secondary Objectives
Secondary objectives were to evaluate the following:
Failure rate, defined as the presence or recurrence of the initial pathology 6 months after surgery (CT scan recurrence and/or sinus symptomatology). The side of the approach (ipsi- or contralateral to pathology). Early or late complications. The quality of the scarring evaluated 6 months after surgery with SCAR-Q Appearance scale.12 The SCAR-Q score is calculated from 0 to 100: the higher the score, the better the outcome. The SCAR-Q appearance scale is a patient-related outcome tool. This patient-reported outcome instruments focus mainly on measuring appearance, symptoms, and psychological issues (eg, “My scar is painful” and “I get upset when people see my scar”).
This self-questionnaire has been rigorously developed to evaluate the impact of scars in adults and children (surgical, traumatic, and burn scars).
Duration of surgery (min).
Results
Population
Between January 2017 and January 2019, 20 patients were included in the study (15 patients in group 1 and 5 patients in group 2). Mean age was 53 years old (10 males, 10 females, sex ratio = 1). Pathologies are reported in Table 1.
Distribution of Patients in Each Group According to Initial Pathology.
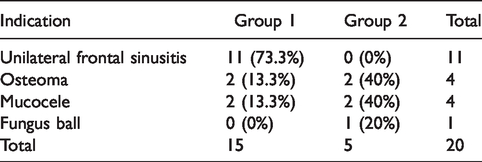
Group 1 predominantly comprised unilateral frontal sinusitis (73.3% of patients, n = 11). All patients with unilateral frontal sinusitis had previously undergone endoscopic endonasal surgery for FS drainage. Two patients in group 1 with mucoceles had also undergone anterior endoscopic surgery. Group 2 comprised various unilateral diseases (mucoceles, fungal balls, osteomas). No patient in group 2 had received prior surgery.
Main Objective
For all patients in groups 1 and 2, TFS could be performed (success rate = 100%).
Secondary Objective
Failure rate
Six months after surgery, all patients were asymptomatic and CT-scan interpretations were normal, specifically regarding the FS. No patient needed revision surgery (0%).
Side of the approach
Four patients (26.6%) in group 1 had an ipsilateral approach to the affected sinus. All patients in group 2 had a contralateral approach, allowing easier access to the lateral extent of the opposite FS.
Complications
Transient diplopia was observed in 2 patients (10%). The first case was intermittent diplopia present in the morning and was due to palpebral edema. The diplopia was no longer present 30 days postoperatively. The second case, consecutive to intraoperative disinsertion of the superior oblique muscle pulley, was resolved by 3 months postsurgery. Five cases (25%) of frontal hypoesthesia were observed, of which 4 disappeared in less than a month. No serious complication (hemorrhage, orbital hematoma, orbital breach, or CFS leak) was reported. Postoperative palpebral edema was described in all patients but was not considered a complication (less than 5 days).
We observed 5 early complications in group 1, 2 in Group 2. One hypoesthesia was reported 6 months after surgery. This was the first patient operated on in our center by this approach.
Scarring
No pathological scarring was described 6 months after surgery in either group. Average SCAR-Q score was 99.3 ± 2.5 (min = 91/100, max = 100/100).
Duration of surgery
Duration of surgery ranged from 36 to 300 minutes, with an average of 90 ± 68 minutes. The longest average surgical durations were found for osteoma procedures (161 ± 109 min), compared to other surgeries (75 ± 42 min). Average duration of the transpalpebral approach (skin incision to frontal septectomy included) was 30 ± 5 minutes.
Discussion
Synopsis of New Findings
The aim of our study was to evaluate the feasibility of TFS. TFS was feasible in 100% of patients, without serious complications (hemorrhage, orbital hematoma, orbital breach, or CSF leak). Other approaches allowing performance of a frontal septectomy have been described in the literature.13,14 The Draf III procedure makes it possible to remove interfrontal septum but requires an experienced operator, and complications have been described.6,15 For example, Lombardi et al. reported CSF leaks in the management of FS inverted papillomas. 16 In addition, significant failure rates have also been reported, mostly in cases of frontal sinusitis.17–19 Draf III failure is problematic because the 2 FS recesses are scarred and the surgeon has no adequate solution. 7 This endoscopic approach is also largely unsuitable for pathologies involving the lateral extent of the FS, as reported by several authors.4,20,21 Complications following Draf IIc have not been addressed in the literature. 5
External approaches are an alternative for interfrontal septum removal, as described by many authors. They avoid damaging the frontal recess by approaching the FS directly, whether a transfacial or a coronal incision is used.2,22–24 The coronal approach does not induce facial scarring but may be associated with permanent hypoesthesia or alopecia. 25 The transfacial approach is less exposed to these complications but can lead to a visible facial scar. With this approach, the lateral extent can be visualized using angled optics (30° or 70°), although surgical access remains difficult.
The transpalpebral approach solves these problems without aesthetic consequences. The SCAR-Q scores in our study testified to the invisibility of the scar. Over the past 2 years, since adopting this procedure, we have performed none of the previously mentioned external procedures for the indications studied here.
Applicability of the Surgical Procedure
The transpalpebral approach is simple and fast to perform. In our study, the transpalpebral approach always allowed to remove of the interfrontal septum. No problems were encountered, whatever the pathology involved (Figure 3).
A, Preoperative CT-scan showing left frontal sinusitis. B, Postoperative CT-scan after transpalpebral frontal septectomy.
However, some situations may prevent the use of this approach:
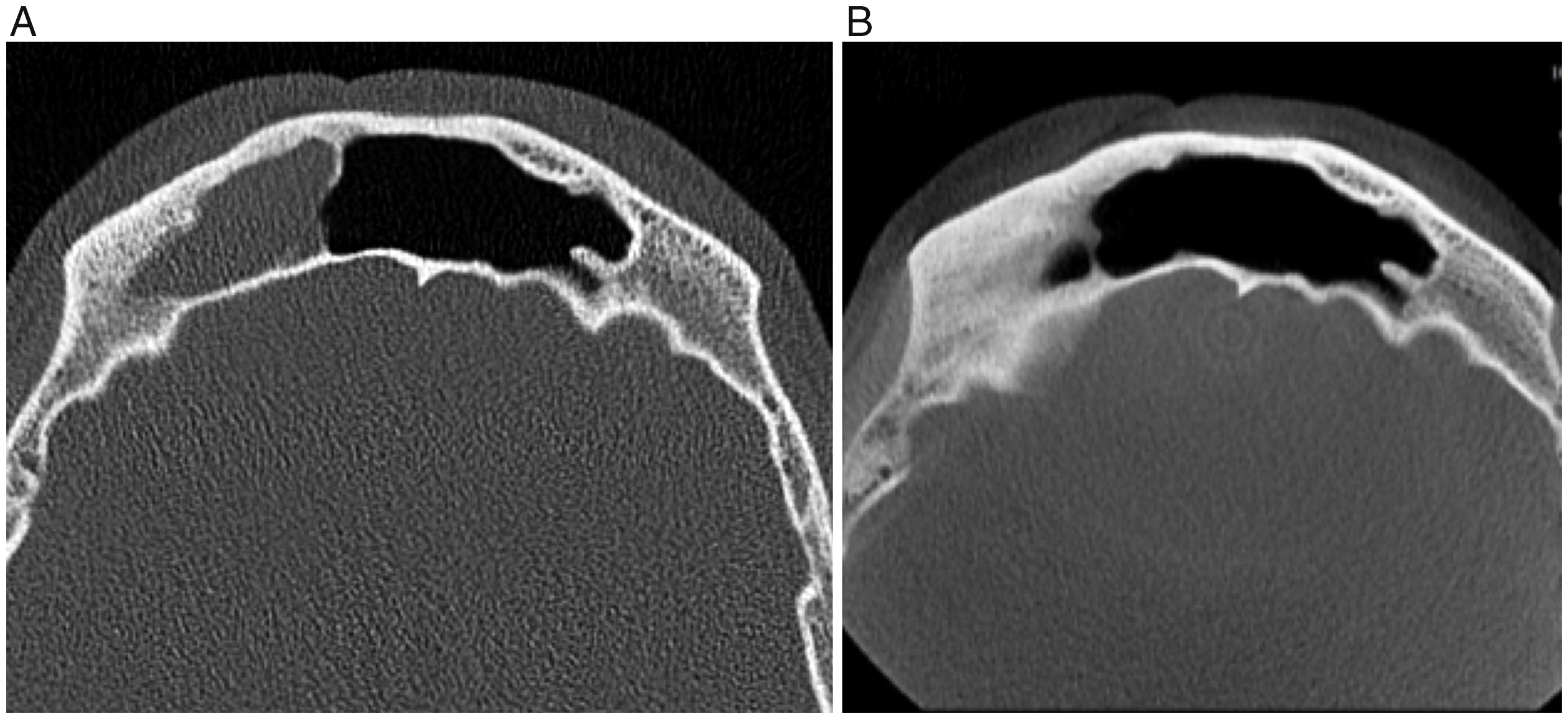
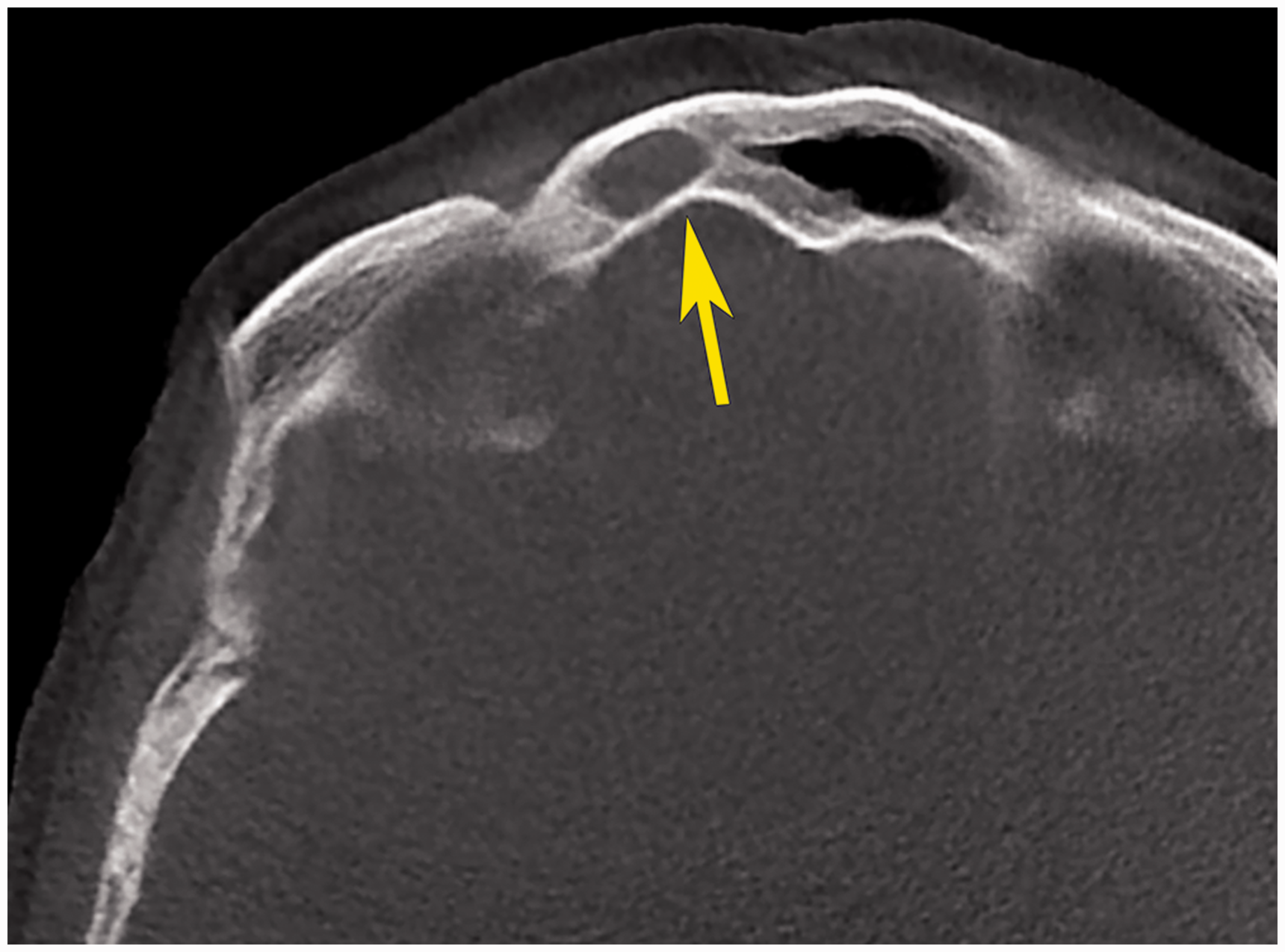
In cases of bilateral stenosis of frontal recesses: removing the interfrontal septum is nonessential as the 2 FS drainage systems are nonfunctional. In cases involving anatomical risk: FS depth <3 mm (risk of CFS leak), dehiscence of the FS posterior wall (Figure 4).
Contraindication of TFS. Axial CT-scan view showing frontal sinus depth <3 mm (arrow). If CAS is unavailable.
TFS may be proposed first line for group 2 patients when impossibility of accessing the lateral extent of the FS is predictable and as second line for group 1 patients (TFS aiming to drain FS in the contralateral FS). An exclusive endoscopic approach should remain the gold standard.
Evaluation of Secondary Objectives
In our study, no patient had a recurrence of their frontal pathology 6 months postoperatively, thus testifying to the degree of control achievable by this approach. The most common early complication was hypoesthesia in the V1 nerve area, initially reported in 5 patients. This hypoesthesia especially involved the supra-trochlear nerve, more medial than the supraorbital nerve. In 1 patient, hypoesthesia had partially subsided but persisted 6 months after surgery. This was the first patient operated on by this approach, for which the V1 pedicle was stretched during surgery.
No case of intraorbital hematoma was found in our series. The anterior ethmoidal artery is not visible during the procedure and remains protected. Careful hemostasis of the corrugator muscle is required to avoid significant bruising. No serious complication such as orbital breaches or CFS leaks was reported. Optimal visualization of the posterior and inferior walls of the FS guarantees safety against these complications.
We also confirmed the need for CAS. This technology optimizes surgical landmarks, especially when performing frontal sinusotomy and drilling the interfrontal septum.
Comparison With Other Studies
To date, no study has been published describing a transpalpebral approach performed contralaterally to the pathologic FS. Indeed, all published approaches access the pathological FS directly.10,11,26 In these studies, it appeared logical to combine the transpalpebral approach with endoscopic surgery in order to permeabilize the FS and avoid recurrence.
Albathi et al. described combined endonasal and transpalpebral approaches for the management of inverted papillomas with extension to the lateral extent of the FS. 10 They performed a bony flap laterally to the supraorbital and supratrochlear pedicles, allowing direct access to the lateral extent of the FS. In their study, this procedure was associated with Draf IIb or Draf III.
Knipe et al. also described a transpalpebral approach for the management of FS disease when associated with ophthalmologic complications. 11 In their study, access to the sinus was obtained directly through the bony defect secondary to infection. They did not perform frontal septectomy. We believe that the absence of permeabilization of the FS exposes the patient to a high risk of recurrence.
A study conducted on cadavers by Steele et al. 4 showed the interest of the transpalpebral approach associated with a lateral frontal sinusotomy allowing direct access to the lateral extent of the FS. This research also confirmed the difficulties of accessing the lateral extent of the FS using endoscopic approaches, even Draf III, especially regarding control of the posterior wall of the FS (0% access in 24 dissections).
If performed contralaterally, TFS gives easy access to the lateral extent of the FS. This explains why 100% of patients in Group 2 had a contralateral approach to the disease. However, an ipsilateral approach was used in 4 patients in group 1 because of a preexisting bone defect (complication of sinusitis) located next to the area targeted for sinusotomy. In these cases, access to the lateral extent of the opposite FS was not the purpose of the surgery.
Although mucociliary clearance may argue against the success of TFS, the literature demonstrates the effectiveness of the technique. 2 Reh et al. showed that drainage of FS secretion via the opposite side was compatible with mucociliary activity. 27
Limits
The main limit of TFS is the need for CAS. However, many operating rooms are now equipped with surgical guidance systems.
The main limitation of our study is the duration of follow-up. In our investigation, the results obtained are encouraging, especially regarding surgical feasibility and clinical success. However, cases of recurrence years after a surgical procedure have been reported in the literature. A prospective study on a larger population with a 5-year follow-up would provide a better understanding of long-term outcomes associated with TFS. Moreover, evaluation of patients’ symptoms was based exclusively on patient interviews.
Conclusion
TFS was feasible for all of patients in this study. This procedure allows drainage of the FS and provides access to the lateral extent of the contralateral FS, without visible scarring, and with few lasting complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.