
Abstract
Background
Topical nasal decongestant sprays are used commonly in routine otolaryngology practice to reduce the symptoms of nasal airway obstruction (NAO) through vasoconstriction, thereby reducing the bulk of vasoerectile tissue and increasing nasal airflow. Such tissue is found predominantly on the lateral wall of the nose within the inferior turbinates (ITs), but recent evidence suggests that it may also be found medially within the nasal septal swell body (SSB).
Objective
To determine whether isolated topical decongestion of the medial nasal wall, targeting the SSB, is as effective as isolated decongestion of the lateral nasal wall, targeting the IT, in maximizing nasal patency.
Methods
A double-blinded, randomized controlled, crossover study was performed investigating the effect of decongestion of the lateral nasal wall or septum in isolation on nasal airflow. Isolated decongestion was performed by placing a cottonoid, soaked in oxymetazoline and attached to a silastic sheet, into the nasal cavity randomly facing either the septum or lateral nasal wall, bilaterally. Anterior rhinomanometry, acoustic rhinometry, peak nasal inspiratory flow (PNIF), and subjective patient-reported outcomes (Sinonasal Outcome Test (SNOT-22) and Nasal Obstruction Symptom Evaluation (NOSE) scores) were recorded at baseline and postdecongestion. Decongestion of the alternate site was then performed at a later date.
Results
A total of 20 healthy volunteers (30% females, mean age 26.6 ± 3.8 years) were recruited. Improvements in nasal obstruction and SNOT-22 scores were found following decongestion of the septum compared with baseline (mean difference: 0.82, t = 2.32, P = .04; mean difference: 3.30, t = 2.50, P = .04, respectively). Improvements in mean inspiratory flow, minimal cross-sectional area, volume, and PNIF were also demonstrated.
Conclusion
This study suggests that the SSB contains erectile tissue that responds to topical decongestant therapy in a similar manner to IT tissue. The SSB may represent a novel target in surgery for NAO.
Introduction
Nasal airway obstruction (NAO) is one of the most common presenting complaints in general otolaryngology and specialist rhinology practice. 1 While the differential diagnoses are broad and may include underlying pathologies such as allergy, inflammatory conditions, neoplasia, or vascular malformations, many patients have an underlying, anatomical cause for their symptoms. 2 These are most commonly related to deviation of the nasal septum and inferior turbinate (IT) hypertrophy, both of which have been extensively studied with respect to their effect on nasal airflow, along with interventions that may correct such abnormalities.3–5
The ITs are long, soft tissue, and bony projections arising from the lateral nasal wall. Previous studies have demonstrated that, histologically, the ITs contain a stroma filled with arteriovenous channels. 6 These vessels are regulated by the autonomic nervous system, which facilitates their presumed role in regulation of nasal airflow, humidification of inspired air, thermoregulation, and filtration of particulate matter such as dust or pollen.
The vasoerectile nature of the ITs, driven by arteriovenous congestion, is believed to be the mechanism by which IT hypertrophy causes NAO. As a result, topical nasal decongestants used to treat NAO are believed to act primarily through vasoconstriction of these vessels, resulting in reduction in IT volume and improved nasal patency. Therefore, many clinicians recommend directing decongestant nasal sprays laterally to maximize particle deposition on IT tissue.
Recent evidence has suggested that, histologically, vascular erectile tissue can also be found within a localized region of the nasal septum, known as the septal swell body (SSB).7,8 The SSB is a distinct structure lying anteriorly and superiorly, composed of a thicker cartilage and mucosal surface, compared with the rest of the septum. The observation that the SSB contains vascular erectile tissue has led to the suggestion that the SSB may play a role in airflow regulation, in a similar manner to the ITs. While some observational studies have suggested that the SSB may be a potential therapeutic surgical target to address in recalcitrant NAO,9,10 no studies have investigated the effect that reduction in SSB volume, via topical decongestion, has on self-reported nasal obstruction scores and objective measurements of nasal airflow such as rhinomanometry, acoustic rhinometry, and peak nasal inspiratory flow (PNIF).
This study aims to compare the effectiveness of topical decongestant therapy directed solely at the medial nasal wall, including the SSB to topical decongestant therapy directed solely at the lateral nasal wall, including the ITs. Furthermore, comparison is made between these results. The results of this study may act as a predictor for the effectiveness of novel surgical procedures aimed at reducing SSB volume, as an alternative to, or in addition to, traditional techniques of IT reduction.
Materials and Methods
Subject Characteristics
A double-blinded, randomized controlled, crossover trial was performed. Healthy volunteers, recruited from a tertiary hospital medical school (Westmead Hospital, University of Sydney, Australia) were invited for screening between January 2018 and June 2018.
At screening, each subject underwent a detailed history and examination. Exclusion criteria were age younger than 18 years, previous history of nasal surgery, previous diagnosis of rhinitis or chronic rhinosinusitis, or the use of regular intranasal medications (including corticosteroid use and decongestant sprays). Anterior rhinoscopy and rigid nasendoscopy were performed in each eligible patient, and subjects were further excluded if there was significant nasal septal deviation, polyps, or gross IT hypertrophy. Examination and decision for inclusion were performed by 2 fellowship-trained rhinologists (J. C. and N. S.), and any disagreement was resolved by consensus following direct discussion.
Initial patient demographics of recruited patients were recorded including age, sex, and other medical history. Recruited patients were then brought back to clinic on a separate day for experimentation.
Ethical approval from the Western Sydney Local Health District was received prior to data collection.
Study Design
For each subject, 2 custom nasal devices (Figure 1) were created, designed to facilitate isolated application of topical decongestant on one side (either the medial or lateral nasal wall), while preventing decongestant from reaching the other side. This was created by cutting a 0.51 mm silastic sheet (Medtronic, Jacksonville, Florida) into the shape of the anterior nasal cavity and attaching a 13 mm × 76 mm cottonoid (Codman Surgical Patties, Integra Life Sciences, Fort Worth, Texas) onto only one side of the silastic. The cottonoid was then carefully soaked with oxymetazoline from a spray bottle (Drixine, Bayer, Leverkusen, Germany).
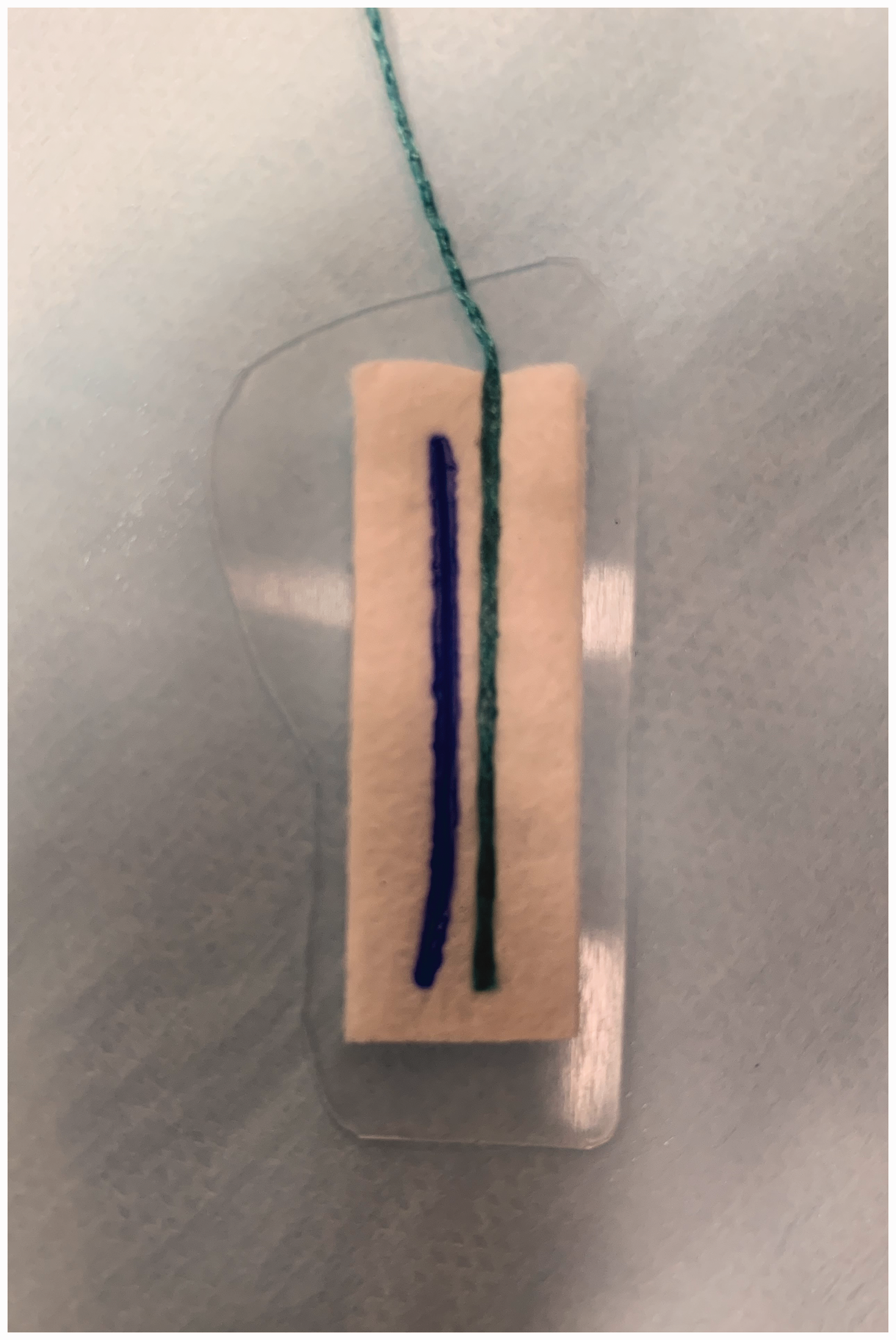
Photo of the created nasal device inserted into the nasal cavity. This device is created by attaching a cutting a 0.51 silastic sheet into the shape of the anterior nasal cavity and attaching a cottonoid to one side.
Prior to device placement, subjects completed a baseline SNOT-22 11 and NOSE 12 score questionnaire and underwent anterior rhinomanometry, acoustic rhinometry, and PNIF.
Subjects were then randomized to either having the soaked cottonoid side of the device applied to the lateral nasal wall or nasal septum. Randomization was performed using computer generation. Application of the device was performed by a blinded otolaryngology resident under direct rigid nasendoscopic vision, and subjects were also blinded to the direction which the device was facing using a blindfold. Subjects who were allocated to the lateral nasal wall arm had the cottonoid placed carefully over the full length of the IT, while those allocated to the nasal septum had the cottonoid placed over the SSB.
Devices were retained in each nasal cavity bilaterally for 10 minutes before removal. Following removal, subjects were then asked again to complete SNOT-22 and NOSE questionnaires as well as repeating all the objective nasal patency tests.
Crossover occurred at a second date, after approximately 2 to 3 weeks. Subjects who were randomized to the lateral nasal wall then had a new device with cottonoid applied to the septum and vice versa. Again, the self-reported questionnaires of the SNOT-22 and NOSE scores were recorded, and anterior rhinomanometry, acoustic rhinometry, and PNIF were performed.
Statistical Analysis
Descriptive data were presented as percentages for categorical variables and means with standard deviations for continuous variables in the normal distribution. Comparisons of categorical variables between the nasal septum and lateral nasal wall groups were performed using the χ2 test, while comparisons of continuous variables were performed using a paired t test.
All statistical analysis was performed using SPSS version 25 (SPSS Inc, IBM, Chicago, Illinois). Statistical significance was determined at the P < .05 level.
Results
A total of 20 subjects (30% females, mean age 26.6 ± 3.8 years) were recruited into the study and randomized. All subjects recruited had no other significant medical history. In total, 50% (n = 10) of subjects were randomized to isolated decongestion of the lateral nasal wall first, while the remaining 50% were randomized to the nasal septum.
Self-reported Questionnaires
Scores taken prior to any decongestion therapy were considered as baseline values. The mean NOSE score was 2.08 ± 2.1, the mean nasal obstruction score was 0.77 ± 1.09, and the mean SNOT-22 score was 8.23 ± 7.0.
Following isolated decongestion of the lateral nasal wall, the mean NOSE score was 0.75 ± 0.7, mean nasal obstruction score 0.13 ± 0.35, and mean SNOT-22 score 3.88 ± 3.8. Comparison of lateral decongestion with baseline levels demonstrated a statistically significant improvement in SNOT-22 score (mean difference: 3.43 ± 3.55, t = 2.55, P = .04). However, no statistically significant difference was noted for the NOSE score (mean difference: 1.00 ± 1.73, t = 1.53, P = .18) or nasal obstruction score (mean difference: 0.29 ± 0.76, t = 1.0, P = .36).
Following isolated decongestion of the septum, the mean NOSE score was 1.18 ± 1.6 and the mean SNOT-22 score was 4.55 ± 4.0. Nasal obstruction and SNOT-22 were noted to be significantly reduced when compared with baseline scores (mean difference: 0.82 ± 1.17, t = 2.32, P = .04; mean difference: 3.30, t = 2.50, P = .04, respectively). There was no difference in the NOSE score (mean difference: 1.18, t = 1.76, P = .11).
Anterior Rhinomanometry
Anterior rhinomanometry of the left nostril demonstrated a significantly increased mean inspiratory flow following decongestion of the septum and lateral nasal wall when compared with baseline levels (effect size: 0.53, P = .04; effect size: 0.94, P = .008, respectively). On the right nasal cavity, these results were also consistent (effect size: 0.34, P = .01; effect size: 1.07, P = .01, respectively).
Acoustic Rhinometry
On acoustic rhinometry, both decongestion of the septum and lateral wall increased minimal cross-sectional area of the left (effect size: 0.55, P = .01; effect size: 0.77, P = .04, respectively) and the right (effect size: 0.59, P = .02; effect size: 0.48, P = .04, respectively). Volume was also increased following decongestion of the septum and lateral wall on the left (effect size: 0.25, P = .02; effect size: 0.32, P = .0001, respectively) and the right (effect size: 0.46, P = .01; effect size: 0.31, P = .01, respectively).
Peak Nasal Inspiratory Flow
Both decongestion of the septum (effect size: 0.28, P < .001) and the lateral wall (effect size: 0.43, P < .001) resulted in significantly increased peak inspiratory flow compared with baseline.
Discussion
This crossover trial study demonstrated that decongestant therapy isolated to the nasal septum both reduces subjective nasal obstruction and other nasal-related symptoms and improves objective measures of nasal airflow including anterior rhinomanometry, acoustic rhinometry, and PNIF. In addition, measures of effect of improvement were comparable to that when decongestant was applied to the lateral nasal wall (ITs), the presumed area where the mechanism of action of decongestion is thought to primarily occur.
Wexler et al. 8 studied 14 mucosal biopsy specimens from the SSB and demonstrated that this tissue contained venous sinusoids and clusters of seromucinous glands, which histologically appeared very similar to turbinate tissue. By contrast, the anterior–inferior nasal septum consisted of mainly only transitional-type epithelium. Therefore, these authors suggested that the swell body be considered another expansile, vascular tissue of the nose.
The results of our study are consistent with this hypothesis. In addition, our data suggest that the SSB, at least in healthy subjects, also undergoes vasoconstrictive changes following decongestant therapy, resulting in volume reduction and improved nasal patency. Therefore, there may be a need to reconsider the long-held belief that nasal sprays should be directed laterally away from the septum, as septal deposition may also confer symptomatic benefit.
It also may follow that the SSB’s vasoerectile nature may mean it has a normal, physiological size fluctuation that, when impaired, may cause it to become hypertrophic, thus mimicking the pathology seen in hypertrophied ITs. In such patients, a large SSB may contribute to pathological nasal obstruction and may benefit from surgical intervention. Early studies by both Yu et al. 9 and Catalano et al. 10 have demonstrated some promise in SSB intervention in patients with NAO. Yu et al. demonstrated that patients who underwent both SSB reduction and inferior turbinoplasty experienced improved nasal obstruction visual analogue scores compared with those who underwent inferior turbinoplasty alone. Catalano et al. demonstrated significant improvements in NOSE scores after coblation of the SSB in patients with intractable NAO despite previous septoplasty, turbinate reduction, and internal nasal valve repair.
Several limitations exist within this study. First, the overall cohort size remains small, and all subjects were healthy with no previous complaints of nasal obstruction and no prior history of sinonasal disease, and therefore do not require medical treatments such as topical decongestion use. As a result, the results of the study may not reflect those patients who have NAO and pathology and do require medical treatment clinically. Nevertheless, a statistically significant improvement in nasal outcomes was identified in most subjective and objective tests despite this limitation. Second, there is no certainty that the device created completely prevented decongestant leak to other parts of the nasal cavity, and therefore results may be overestimated. However, cottonoids 13 have had a long history of successful use in endoscopic sinus surgery to apply medication to a localized area of mucosa, and silastic sheets 14 are routinely used to successfully separate postoperative mucosal surfaces in many sinonasal procedures.
Nevertheless, future research is warranted to determine the effect of topical decongestants isolated to the SSB in patients with symptomatic NAO as well as the use of other topical nasal medications on the SSB (such as antihistamine or corticosteroid sprays). A potential follow-up study would be to add a further test group targeting both the lateral nasal wall and septum, to determine whether any additional benefit is achieved by delivery to both sites. Other further studies may investigate novel surgical procedures involving the SSB to establish its potential as a surgical target in NAO, in recalcitrant cases, in cases of surgical failure, as an adjunct to IT procedures or even as a potential stand-alone procedure.
Conclusion
The SSB contains erectile tissue that responds to isolated decongestant therapy, resulting in measurable improvements in nasal patency, in a manner comparable to IT tissue. The SSB may represent a novel target in surgery for NAO.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.