
Abstract
Background
Subcutaneous immunotherapy (SCIT) has been used for treating local allergic rhinitis (LAR) patients. However, the clinical efficacy and safety were still questioned.
Objective
This study was designed to estimate the efficacy and safety of SCIT for treating LAR patients through meta-analysis.
Methods
We systemically searched MEDLINE, Cochrane Library, and Embase publications. Randomized, double-blind, clinical trials for the efficacy and safety of Allergen Immunotherapy (AIT) for LAR were included. A meta-analysis of 4 clinical endpoints (combined symptom and medication scores [CSMS], symptom scores [SS], medication scores [MS] and rhinoconjunctivitis quality of life questionnaire [RQLQ]) and adverse events (AEs)) was performed after bias and heterogeneity assessments. The immunologic response results were summarized.
Results
Four RCTs with 134 patients were included. Four studies for analyzing primary outcomes (CSMS, SS, MS) and AEs, three for RQLQ results. The results indicated an important significant difference between SCIT and placebo groups, list as follows: CSMS (SMD = −2.42, 95% CI: −3.60 to −1.25, P < .0001), SS (SMD = −2.08, 95% CI −3.68 to −0.48, P = .01), MS (SMD = −1.43, 95% CI: −2.65 to −0.21, P = 0.02), RQLQ (SMD = −0.70, 95% CI −1.29 to −0.12, P = .02), Local AEs (RR = 4.13, 95% CI 1.08 to 15.77, P = .04). For immunologic response, significantly increased serum sIgG4 levels and improvements of allergen tolerance was observed after SCIT.
Conclusions
Our meta-analysis suggests that SCIT has a significant effect on improving symptoms and reducing medicine consumption for LAR patients. Larger and multicenter clinical trials are needed to clarify the safety and long-term efficacy.
Keywords
Introduction
Local Allergic Rhinitis (LAR), or “entopy”, as a new phenotype of rhinitis, is characterized by the localized nasal allergic response but lacks the evidence of systemic atopy. 1 The pathological features of LAR are associated with a Th2 nasal inflammation pattern, including local production of sIgE in nasal mucosa and a positive nasal allergen provocation test (NAPT) response to specific inhaled allergens.2–5 LAR patients display similar local eosinophilic inflammation and rhinitis symptoms with Allergic Rhinitis (AR) patients, but unlike AR, the skin prick test (SPT) and serum specific immunoglobulin E (sIgE) test negative in LAR patients.6,7
The current treatment programs of LAR are similar to AR, mainly contain health education, avoidance of allergens and pharmacotherapy (nasal corticosteroid, antihistamines, etc).6,8 Allergen Immunotherapy (AIT) is one of the treatment options for IgE-mediated allergic diseases and is currently considered to be the only therapeutic intervention that can rebalance the immune system and thus affect the natural course of allergic diseases, can be performed through subcutaneous (SCIT) and sublingual route (SLIT).9–12 Considered LAR is termed as a locally sIgE-mediated allergic disease; patients may benefit from AIT. Investigators have demonstrated significant effectiveness and good tolerance of SCIT in patients with LAR.13–17 The previous meta-analysis has already confirmed the long-term efficacy of AIT for food allergies, AR, allergic conjunctivitis, and allergic asthma.18–23 However, no meta-analysis has been conducted to illustrate whether AIT can be effective in LAR patients until now. We performed this meta-analysis and systematic review to examine the efficacy and safety of AIT for LAR.
Methods
Search Strategy
Two reviewers independently searched the following databases with English as the restricted language: MEDLINE, The Cochrane Library, and The Embase databases. The databases were searched from inception to March 21, 2021. They searched for Randomized Controlled Trials (RCTs) on the efficacy and safety of allergen immunotherapy of LAR. The keywords of search strategy were list as follows: “Local allerg*,” “local atopic*,” “entopy,” “Local respiratory allergy,” “LAR,” “immunotherapy,” “desensitization,” “immunologic,” “randomized controlled trial”.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Diagnosis of LAR: rhinitis symptoms (nasal running, blocking, itching, or sneezing) after allergen exposure; a positive NAPT to aeroallergens; negative SPT and absence of serum sIgE. (2) The treatment program of experiment group is AIT while placebo in control group. (3) Two groups share the similar in age, disease severity, and other essential conditions. (4) The type of study is all RCTs. The following exclusion criteria were recommended: not LAR, not RCTs, animal studies, reviews and duplicated studies.
Data Extraction
Two researchers independently screened the literature and extracted the data on the following details: the name of investigators, the year of publication, the title of the Journal, the sample size of total and each arm, the type of rhinitis, the schedule of AIT, the following-up time of study, combined symptom medication scores (CSMS), symptom scores (SS), medication scores (MS), rhinoconjunctivitis quality of life questionnaire (RQLQ) scores, adverse events(AEs), and immunologic response results (nasal tolerance of allergens, serum sIgE, serum specific immunoglobulin G4 [sIgG4]). The discrepancy was resolved by discussion, and the third author would decide if two authors could not make a consensus.
Quality Assessment
We assessed the quality of selected RCTs by using the risk of bias tool (Cochrane Handbook for Systematic Reviews of Interventions, Version5.1.0) in Revman5.4. Seven different aspects were evaluated and each aspect was assessed with “high risk,” “low risk,” and “unclear”. Another investigator would be consulted if agreements were not be reached.
Statistical Analysis
The data were analyzed by using Revman5.4 (Cochrane Collaboration, Oxford, UK). Four clinical endpoints (CSMS, SS, MS, RQLQ) and immunologic response results (allergen tolerance to NAPT, serum sIgE, and sIgG4) were summarized by mean ± SD and directly compared between groups. AEs were dichotomous outcomes, thus the relative risks (RR) with 95% confidence intervals (CIs) were used to estimate the results. I2 was used to assess heterogeneity, when P > .05 and I2 < 50%, indicated the heterogeneity of the study was small. Fixed effect models were used if the heterogeneity was present at I2 < 50%. Otherwise, random effect models were chosen. We considered P value < .05 as statistically significant.
Results
Search Results
A total of 247 pieces of research were identified according to inclusion criteria; 56, 55, and 136 were from PubMed, Embase, and Cochrane. 80 reports have been removed because of duplication. After screening the title and abstract, 157 records have been excluded due to they were reviews or not LAR or not RCTs. Therefore, 10 were selected for full texts assessment, and 6 studies were meeting reports. Finally, four studies met the eligibility criteria. The flowchart was shown in Figure 1.
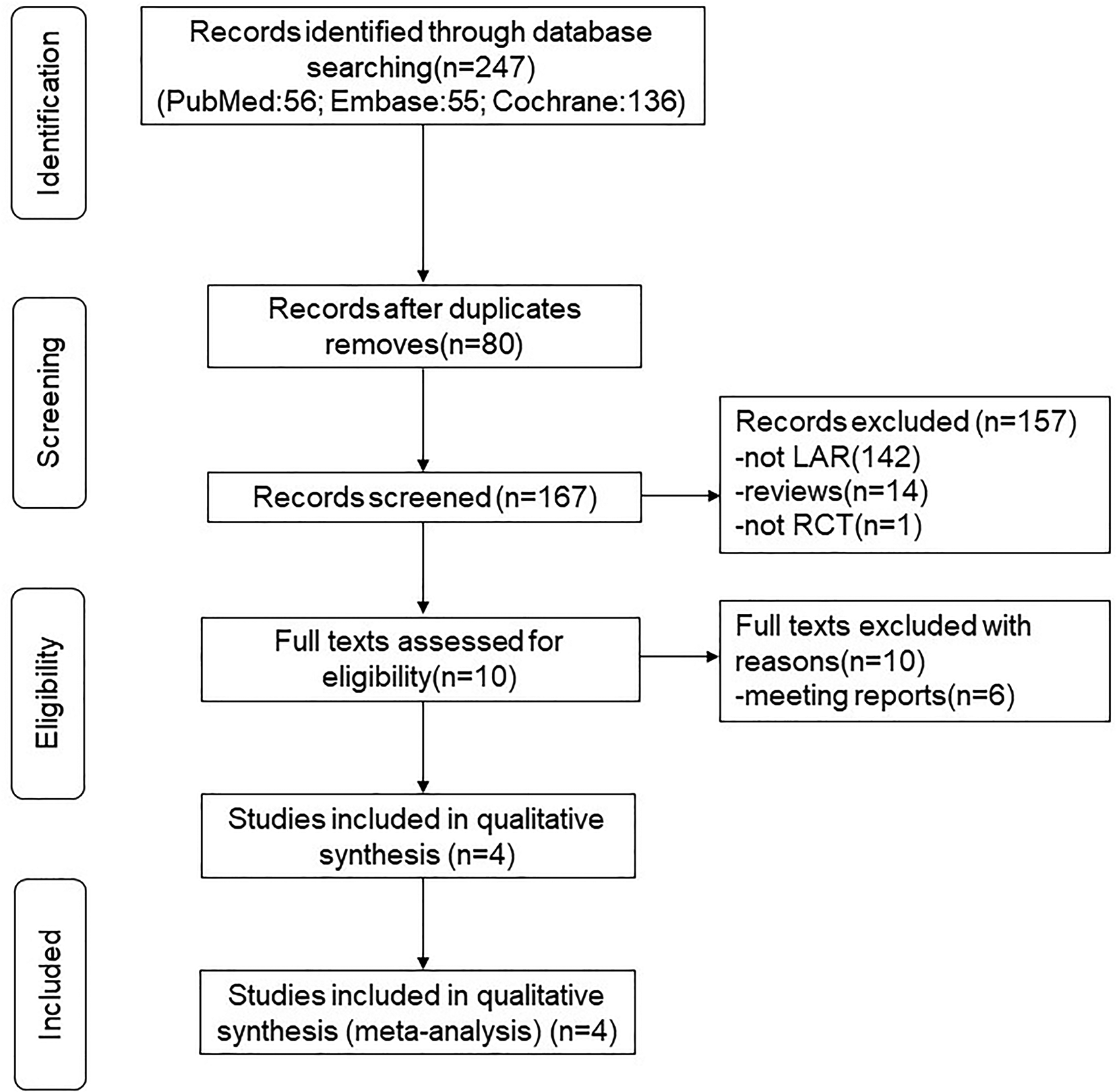
Flow chart of included and excluded studies.
Description of Included Studies and Risk of Bias
In this meta-analysis, we finally retrieved four RCTs, of total 134 LAR patients, 64 were treated with SCIT, and 70 were treated with placebo. In recruited studies, patients in two studies were allergic to birch pollen, one allergic to Dermatophagoides pteronyssinus (Dp) and one allergic to grass pollen. 2 RCTs conducted by Bozek and 2 RCTs from Rondon did not overlap in timeframe. We confirmed that the same patients are not being studied more than once. More details were given in Table 1. The risk of bias of each literature is shown in Figure 2(A) and summarize in Figure 2(B).
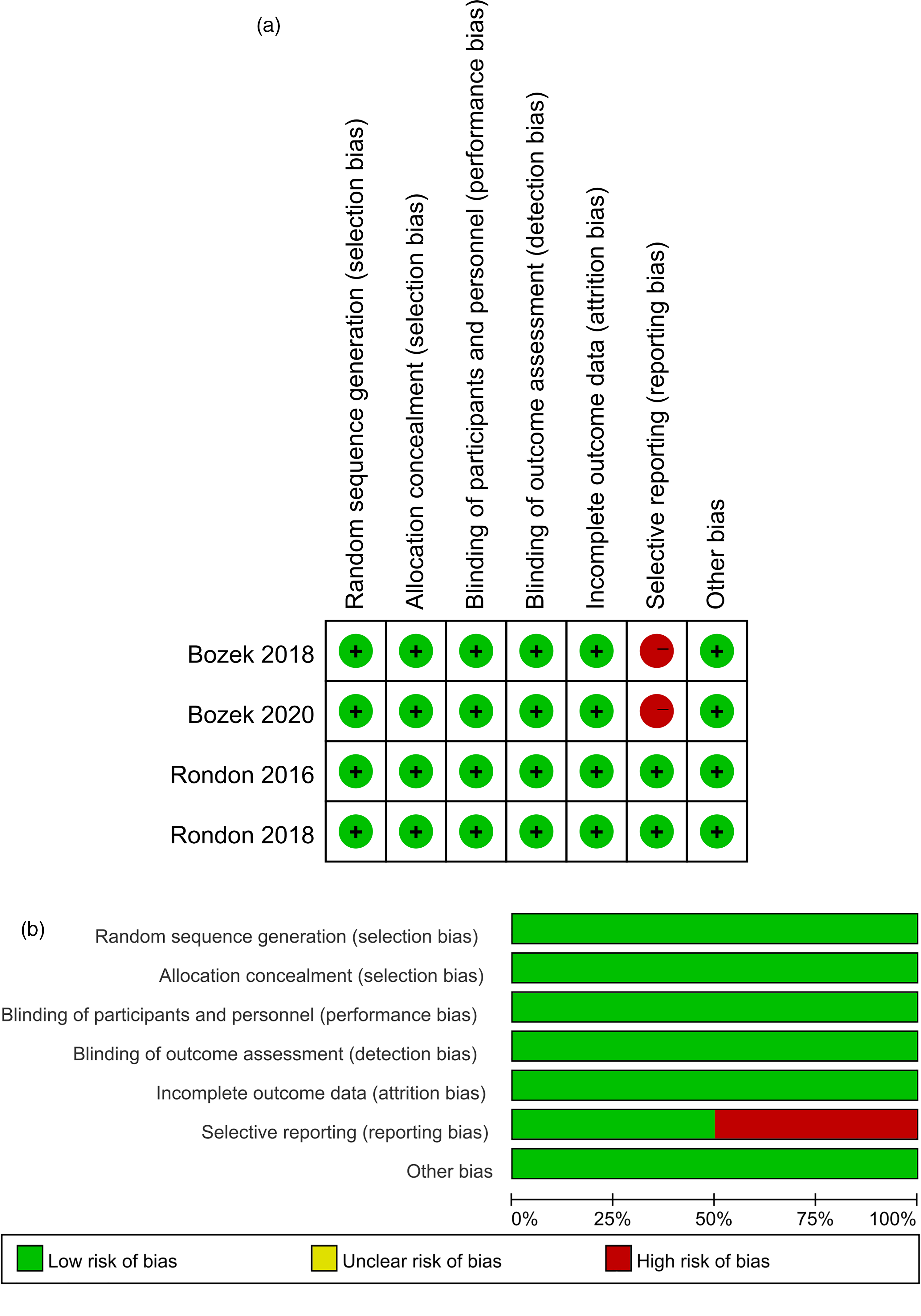
(A) risk of bias summary. Each risk of bias item for each included study. (B) Risk of bias graph. Each risk of bias item shown as a percentage across all included studies.
Basic Characteristic of the Literature.
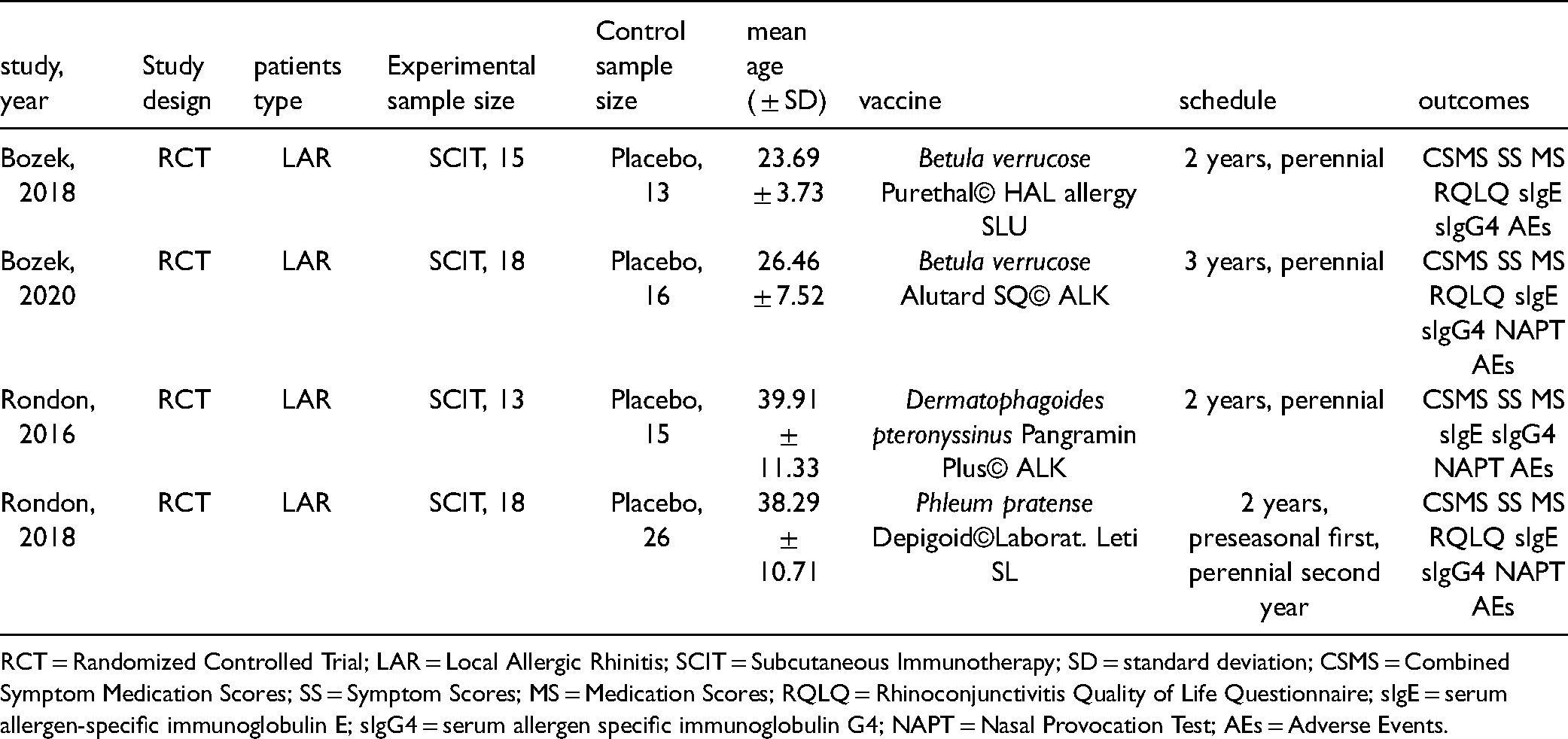
RCT = Randomized Controlled Trial; LAR = Local Allergic Rhinitis; SCIT = Subcutaneous Immunotherapy; SD = standard deviation; CSMS = Combined Symptom Medication Scores; SS = Symptom Scores; MS = Medication Scores; RQLQ = Rhinoconjunctivitis Quality of Life Questionnaire; sIgE = serum allergen-specific immunoglobulin E; sIgG4 = serum allergen specific immunoglobulin G4; NAPT = Nasal Provocation Test; AEs = Adverse Events.
Meta-Analysis Results
Combined Symptom Medication Scores (CSMS)
All studies recruited provided sufficient data for meta-analysis. The calculation of CSMS varied among trials, three trials used a sum of symptom scores and medication scores as CSMS, one trial used the average symptom scores combined medication scores as CSMS. The result of the SCIT versus placebo group is shown in Figure 3. The analysis indicated that compared with placebo group, SCIT produced a clinical improvement with a significant reduction in mean CSMS (SMD −2.42, 95%CI −3.60 to −1.25, P < .0001, I2 = 94%). However, there was significant heterogeneity among studies, the random-effects model was chosen.

Efficacy of SCIT in reducing combined symptom and medication scores (SMD = −2.42, CI −3.60 to −1.25, P < .0001, I2 = 94%).
Symptom Scores (SS)
Four studies, including 64 patients in SCIT group and 70 patients in placebo group were analyzed. Scoring criteria for SS varied among trials, one study used the combination of nasal symptoms and ocular itching score, two studies used nasal and ocular symptom scores, and one study used the average of total symptom scores (nasal, ocular, bronchial scores). The forest plot is shown in Figure 4. Overall, the SCIT significantly reduced the SS, which indicates a 2.08 reduction in the standard studies (SMD −2.08, 95%CI −3.68 to −0.48, P = .01). Moreover, random-effects model was used for analysis due to significant heterogeneity (I2 = 98%).

Efficacy of SCIT in reducing symptom scores (SMD = −2.08, 95%CI −3.68 to −0.48, P = .01, I2 = 98%).
Medication Scores (MS)
MS were available for all trials. The rescue medicines were slightly different in each study, mainly contained systemic/topical antihistamines or systemic/nasal corticosteroids. The heterogenetic test has shown that I2 = 98%, significant heterogenetic observed among trials, and the random-effects model was used (Figure 5). Meta-analysis indicated a statistical difference in MS between two groups. The SMD was −1.43 (95%CI: −2.65 to −0.21, P = .02), indicates that SCIT leads to an important improvement in the symptom and reduction in rescue medication.

Efficacy of SCIT in reducing medication scores (SMD = −1.43[95%CI: −2.65 to −0.21, P = .02, I2 = 98%].
RQLQ Scores
In RQLQ scores analysis, three RCTs,13,14,16 provided sufficient data for meta-analysis, including 51 in SCIT group and 55 in placebo group. The heterogenetic test (I2 = 87%) indicated significant heterogenetic. Therefore, random-effects model was used for meta-analysis. The result showed that SCIT reduced the RQLQ scores compared with placebo (SMD −0.70, 95% CI −1.29 to −0.12, P = .02), indicating SCIT has significant efficacy in improving the Quality of life for LAR patients (Figure 6).

Efficacy of SCIT in reducing RQLQ scores (SMD −0.70, 95%CI −1.29 to −0.12, P = .02, I2 = 87%).
Adverse Events (AEs)
AEs could be divided into systemic and local AEs. Four studies provided data on systemic and local AEs. There were no systemic AEs in SCIT groups (n = 64) or placebo groups (n = 70). Two studies16,17 provided sufficient data to conduct meta-analysis, the proportion of patients who had local AEs was 22.6% (7/31) and 4.88% (3/41) in SCIT group and placebo group. The heterogenetic test was I2 = 0%, with low heterogenetic. Therefore, fixed-effects model was adopted. The results indicated more local AEs occurring in SCIT group than placebo group (RR = 4.13, 95% CI 1.08 to 15.77, P = .04). The forest plot is shown in Figure 7. While another two studies reported the local AEs occurrence rate of total injections but lack of specific injection number, thus we made a description instead of meta-analysis. The results indicated the occurrence rate of total injections of local AEs was higher in SCIT group.

Safety of SCIT in local adverse events (RR = 4.13, 95%CI 1.08 to 15.77, P = .04, I2 = 0%).
Nasal Tolerance to Allergen
To evaluate the improvements of tolerance for specific allergen at the beginning and the end of the study, NAPT was used in three studies.14,16,17 Due to the units of measurement were different, meta-analysis could not perform. However, compared with placebo group and baseline, all studies demonstrated that SCIT leads to a significant improvement in allergen tolerance in LAR measured by NAPT.
SIgE and sIgG4
All studies included have examined the trend of serum sIgE and sIgG4 during the test. Because of the different specific allergens, we do not make the meta-analysis. In three trials,13,14,17 the concentration of sIgE was gradually increased, peaked at sixth month, gradually decreased, and finally returned to undetectable. And in two studies,16,17 the concentration of sIgE turned to be detectable in several patients in both SCIT and placebo groups during the trials. The concentration of sIgG4 showed the same trend in all studies, gradually increasing and became significantly higher than placebo group and baseline after 12 or 18 months.
Discussion
Current clinical evidence for the application of AIT in LAR is limited, the clinical effectiveness and tolerance still not completely clear.24,25 After systematic search, only RCTs related to SCIT for LAR were studied. Therefore, we conducted a meta-analysis to explore the clinical efficacy and safety of SCIT conducted in LAR patients. As far as we know, this is the first meta-analysis of this topic.
We primally performed a meta-analysis of clinical endpoints (CSMS, SS, and MS). Comparison between SCIT and placebo groups demonstrated the positive clinical effect of SCIT treatment, with significantly lower mean CSMS, SS, and MS. Except for symptom and medication scores, three studies introduced RQLQ scores in their trials. As an important parameter for adult quality of life assessment, it measures the individual perceived benefits of patients and also helps to analyze the cost-effectiveness of treatment intervention.26,27 Our analysis shows that SCIT produced a remarkable improvement compared to placebo of mean RQLQ scores, that is, the quality of life of LAR patients can be improved by SCIT. Overall, SCIT can effectively control the symptoms and reduce the rescue medication for LAR patients.
AEs of SCIT in LAR patients is another important outcome that clinical focus on. In our meta-analysis, SCIT was well tolerated, with no systemic AEs occurred in SCIT group. However, all studies included demonstrated that the local AEs were more frequent in SCIT group. We compared the incidence rates of local AEs in two RCTs16,17 and indicated that SCIT was more likely to induce local AEs. Another two results also indicated that the occurrence rate of local AEs was higher in SCIT group than placebo group though the data was not sufficient for meta-analysis. And the same trends in agreement with studies performed in allergic rhinitis treated with SCIT. 28 However, in the study of AIT in other allergic diseases, the incidence of systemic adverse events was about 1% per injection, and fatal allergic reactions occasionally occurred. 29 Regarding no fetal adverse occurred in current RCTs for SCIT conducted in LAR, multiple centers, large samples, and more prolonged clinical observation trials are needed to clarify the tolerance of SCIT for LAR patients.
In addition to clinical outcomes and AEs, the immunologic response results were summarized as well. NAPT, serum sIgE and serum sIgG4 have been used to assess responses to AIT in allergic diseases.30–32 NAPT induced reactions in the nasal mucosa through control and standardized exposure to allergens. Thus, NAPT has been measured in AIT for SAR patients to control inconstancy in allergen exposure. 29 The IgG isotype is regarding as a blocking antibody, which competes with IgE for the same epitope and binds to allergens.33–37 Therefore, we extracted the data of allergen tolerance by NAPT, serum sIgE and sIgG4 as objective responses. However, the data is not sufficient to make the meta-analysis because of the different measurement units; we finally make a summary for the trend of these immunologic response results. Compared with placebo group, we found SCIT improved the tolerance to allergens for LAR patients. Except for the improvement of nasal tolerance, a significant increase of serum sIgG4 was observed among studies. The same trends have been reported in AIT for patients with allergic diseases.30,31 The positive results in nasal tolerance and serum sIgG4 give the evidence that AIT is a reasonable method for the treatment of LAR. The negative results of sIgE are an integral part of the diagnosis of LAR. Among the included studies, three13,14,17 suggested that sIgE increased temporarily, peaking at the sixth month, and then gradually decreased, finally became undetectable again. Temporarily increasing and followed by a reduction in sIgE also observed in AIT, treating grass pollen sensitization patients. 30 In two studies,16,17 several patients in the SCIT and placebo group became sIgE positive after the end of the first year of treatment. It may be related to the natural course of the disease16,17 or due to too much repetition of intradermal skin test.16–18 Therefore, there is no evidence that SCIT will change the state of local allergies in patients with LAR. However, due to the few studies and short observation time, whether SCIT will change the immune status of LAR patients is still under question.
The heterogeneity of the four main outcomes is high. However, the heterogeneity in the region of AIT for the treatment of allergic diseases has been identified by previous studies. 23 Firstly, the clinical-methodological heterogeneity is likely related to the different ages, severity of rhinitis of included participants, and small sample size in all trials. And the source of between-study heterogeneity is mainly due to the various doses of allergens and different allergen extraction in commercial desensitizers among studies. The treatment schedule and observation period are also varied among studies. Furthermore, in this area of AIT, there lacks a consistent scoring algorithm for CSMS, SS, MS. 23 Due to the high heterogeneity, we adopted a randomized controlled model for analysis, however, the factors mentioned above are quite difficult to quantify or adjust for our meta-analysis.
Our meta-analysis has certain limitations. We only included four RCTs, and the total number was relatively small. This may mainly because LAR patients could easily miss due to negative skin tests. Moreover, SCIT treatment takes a quite long period, usually 2 to 3 years. Also, we use English as search language when conduct searches and due to the positive outcomes, that would be more likely to published compare with the negative one, language and publication bias should be considered. And in this analysis, we did not analyze the publication bias due to number of studies was inadequate.
Overall, in our meta-analysis and systematic review, SCIT has a significant effect on reducing symptom scores and reducing the use of emergency medicine. However, larger, multicenter and longer-term RCTs are needed to evaluate the prevalence of adverse events and long-term efficacy.
Footnotes
Acknowledgments
We would like to express our deepest gratitude to Zexi, Xu and Pan, Song for the constant encouragement and guidance for the whole study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 81873693).
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.