
Abstract
Background
The value of aeroallergen skin testing is not known in IgE deficient individuals (IgE<2.5 kU/L).
Objective
To investigate the utility of skin prick (SPT), intradermal skin testing (IDST) and measuring serum specific IgE (ssIgE) in IgE deficient patients presenting with environmental allergy-like symptoms.
Methods
Individuals with IgE deficiency who had both SPT and IDST performed between 2010 to 2020 were matched (age and gender) to three different groups of non-IgE deficient patients with IgE≥2.5 kU/L (normal IgE [2.5 ≤ IgE<100], high IgE [100≤IgE<1000] and very high IgE levels [≥1000 kU/L]) who also had skin testing performed for evaluation of environmental allergy-like symptoms.
Results
Among 34 IgE deficient patients who completed SPT and IDST, 52.9% (18/34) had at least one positive skin test (4 ± 3 positive tests/patient), compared with 91.2% in those with normal, 94.1% with high or 97.1% with very high IgE levels (p < 0.01). In contrast, only one of the IgE deficient patients had detectable ssIgE, while ssIgE levels were significantly higher in all other IgE subgroups. Allergic immunotherapy was prescribed for 22.2% of the IgE-deficient patients with positive skin tests, similar to those with normal (2/31, 6.5%, p = 0.21), high IgE (9/32, 28.1%, p = 0.25) and very high IgE levels (8/33, 23.5%, p = 0.07), with similar efficacy in their symptoms control.
Conclusion
Individuals with IgE deficiency may present with environmental allergy-like symptoms. A combination of SPT and IDST is useful for diagnosing aeroallergen sensitizations in these patients, indicating the presence of skin mast cell-bound IgE in some of these individuals, despite very low serum IgE levels. Further studies are needed to assess the exact significance of positive skin tests and the benefits of immunotherapy in this group.
Keywords
Introduction
Immunoglobulin E (IgE) is the immunoglobulin isotype that mediates type I hypersensitivity reactions, such as environmental allergies. 1 The clinical evaluation of allergic rhinitis and asthma typically includes performing skin testing (skin prick testing [SPT] and/or intradermal skin testing [IDST]) and/or measuring serum specific IgE (ssIgE) to assess the presence of allergic reactivity to different aeroallergens. 2 Skin testing evaluates the presence of specific IgE bound on the surface of skin mast cells, while ssIgE testing assesses the amount of free IgE in the serum. It is generally accepted that high IgE levels are associated with higher rates of sensitization and atopy.2–4
Interestingly, although they have very low or absent serum IgE levels, IgE deficient patients (IgE<2.5 kU/L) can still develop chronic environmental allergy-like symptoms and 23%–73% of these patients have associated diagnoses of asthma and/or rhinitis.5–8 It has been our clinical experience that some patients with IgE deficiency who present with allergic-type respiratory symptoms have positive skin tests, despite having very low serum IgE levels. However, the diagnostic utility of performing allergy testing in IgE deficient patients, using a combination of SPT, IDST and ssIgE, has never been fully evaluated. One subgroup analysis in a study that looked at very low IgE levels in patients with common variable immunodeficiency found a rate of positive ssIgE of 3.5%, 6 however, skin testing was not performed and the rate of respiratory symptoms in that cohort was not reported. Another retrospective study evaluating the characteristics of IgE deficient patients, found that among 420 randomly selected adult patients seen in an Allergy-Immunology Clinic between 1990 to 1996, 44 individuals had IgE deficiency. In this group, the skin tests and ssIgE (as determined through radioimmunoallergosorbent test [RAST]) were negative in all patients, 5 but not all of them presented for evaluation of chronic respiratory symptoms. Moreover, it is not clear how frequently IDST were performed in this cohort. IDST are often done for a comprehensive evaluation of environmental allergies since they may detect as many as 10 to 30% additional sensitizations after negative SPT.9–11
It is important to fully evaluate the sensitization profile in patients presenting with chronic respiratory symptoms, since allergen immunotherapy is recommended in those individuals with proven environmental sensitizations in whom symptoms are not fully controlled with medical management. 12 In the present study, we evaluated the utility of performing SPT, IDST and measuring ssIgE to common northeastern U.S. aeroallergens in a cohort of patients with IgE deficiency presenting for evaluation of environmental allergy-type symptoms, compared with those of matched non-IgE deficient individuals (normal IgE [2.5 ≤ IgE<100], high IgE [100≤IgE<1000] and very high IgE levels [≥1000 kU/L]) with similar symptoms.
Methods
This was a retrospective, observational study approved by the Institutional Review Board of the Albert Einstein College of Medicine in the Bronx, NY. We used Clinical Looking Glass (CLG; a program that combines clinical and administrative data from the electronic medical records from our institution to output clinical cohorts) to find adult patients (age >18 years) who had total IgE levels measured between 2010 to 2020 at our institution, had associated ICD-9/10 diagnoses of rhinitis and had SPT and IDST performed. The rhinitis diagnoses recorded through CLG and gathered for this study were: 477.0-Rhinitis due to pollen, 477.8-Allergic rhinitis due to other allergen, 477.9-Allergic rhinitis, cause unspecified, J30.1-Allergic rhinitis due to pollen, J30.2-Other seasonal allergic rhinitis, J30.81-Allergic rhinitis due to animal (cat) (dog) hair and dander, J30.89-Other allergic rhinitis, J30.9-Allergic rhinitis, unspecified. We did not include patients with ICD-9/10 diagnoses of infectious rhinitis, rhinitis of pregnancy, vasomotor rhinitis, ulcerative rhinitis, atrophic rhinitis, nonallergic rhinitis, rhinitis medicamentosa or other types of drug induced rhinitis. From this cohort, patients with IgE deficiency (IgE<2.5 kU/L) were identified and matched (by age and gender) with patients with normal IgE (2.5 ≤ IgE<100 kU/L), high IgE (100≤IgE<1000 kU/L), and very high IgE levels (≥1000 kU/L).Chart reviews were performed and results of SPT, IDST and ssIgE, and the number of patients prescribed subcutaneous allergic immunotherapy (SCIT) were collected and analyzed. Only patients with selective IgE deficiency (without any other immunodeficiency diagnosis) were included in the study.
Skin Testing and SsIgE
Skin prick tests were performed using a battery of common Northeast United States allergens (mixed tree, birch, mixed grass, ragweed, mugwort, English plantain and mixed weed pollens, dog, cat, mouse and rat dander, cockroach, dust mite, mixed feathers and mixed molds [Greer Laboratories, Inc., Lenoir, NC]). The ComforTen applicator (Hollister-Stier Laboratories, Spokane, WA) was utilized to apply the allergen extracts. The tests were read after 15 to 20 min, with histamine dihydrochloride 10 mg/mL (Hollister-Stier Laboratories) as a positive control and glycerol saline 50% solution as a negative control. A SPT was deemed positive if the wheal diameter was at minimum 3 mm larger than the saline solution. An IDST test was performed if the SPT was negative to any specific allergen. Patients initially had IDST performed at low concentrations (1:100 w/v dilution of the stock solution; IDST-low strength). If the initial IDST testing was negative but the physician determined that additional testing was needed, a second IDST with concentrations ten times higher was performed at another visit (IDST-high strength).
Serum specific IgE to environmental antigens (similar to those used for SPT and IDST) were measured (ImmunoCAP, Phadia) if the physician decided that further testing was necessary based on symptoms. An ssIgE level ≥0.1 kU/L was considered to be positive.
Statistical Analysis
Descriptive statistics were applied to all variables. For comparing the mean levels of two variables between two groups, the 2-sample t test was performed. Categorical variables were compared with the use of Chi square or Fisher exact test for scarce data. A P-value less than 0.05 was considered to be statistically significant. The data was analyzed using SPSS statistical software, version 24.0 (IBM Corp, Armonk, New York).
Results
Characteristics of Patients Included in the Study
In total, 17,044 patients had total serum IgE levels performed and 410/17,044 (2.4%) were found to be IgE deficient (Figure 1). Out of 410 patients with IgE deficiency, 187 did not have associated rhinitis symptoms and were excluded. Out of the 223 IgE deficient patients with associated rhinitis diagnoses, 61 patients had no available skin tests for review or skin tests were not done, 42 patients had associated immunodeficiencies and 86 patients did not have full sets of skin tests performed and were excluded from the study. Overall, 34 patients with IgE deficiency with environmental allergy-like symptoms who had all three types of skin tests performed (SPT, IDST-low strength and IDST- high strength) were included in the final analysis.
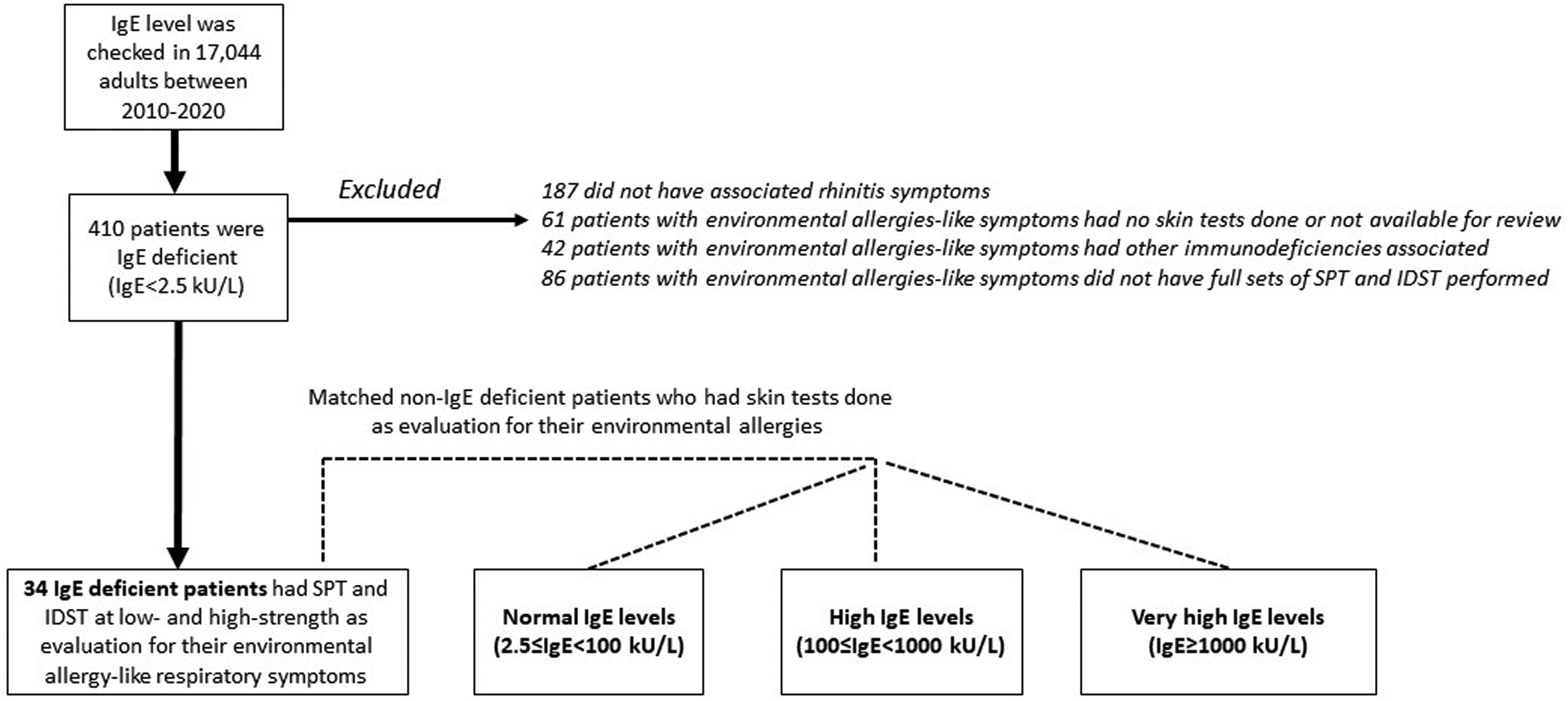
The study flow.
The majority of IgE deficient patients were female (28/34, 82.4%) with a mean age of 52 years (±15). The matching process resulted in a similar distribution among patients with non-IgE deficiency. (Table 1) The majority of the IgE deficient patients presented with perennial symptoms (26/34, 78.8%), and 54.5% (18/34) had associated eye symptoms. There were no significant differences between the four groups regarding asthma diagnoses, forced expiratory volume (FEV1), other immunoglobulin levels (IgG, IgA, IgM), or having been prescribed intranasal corticosteroids or montelukast.
Characteristics of Study Patients.
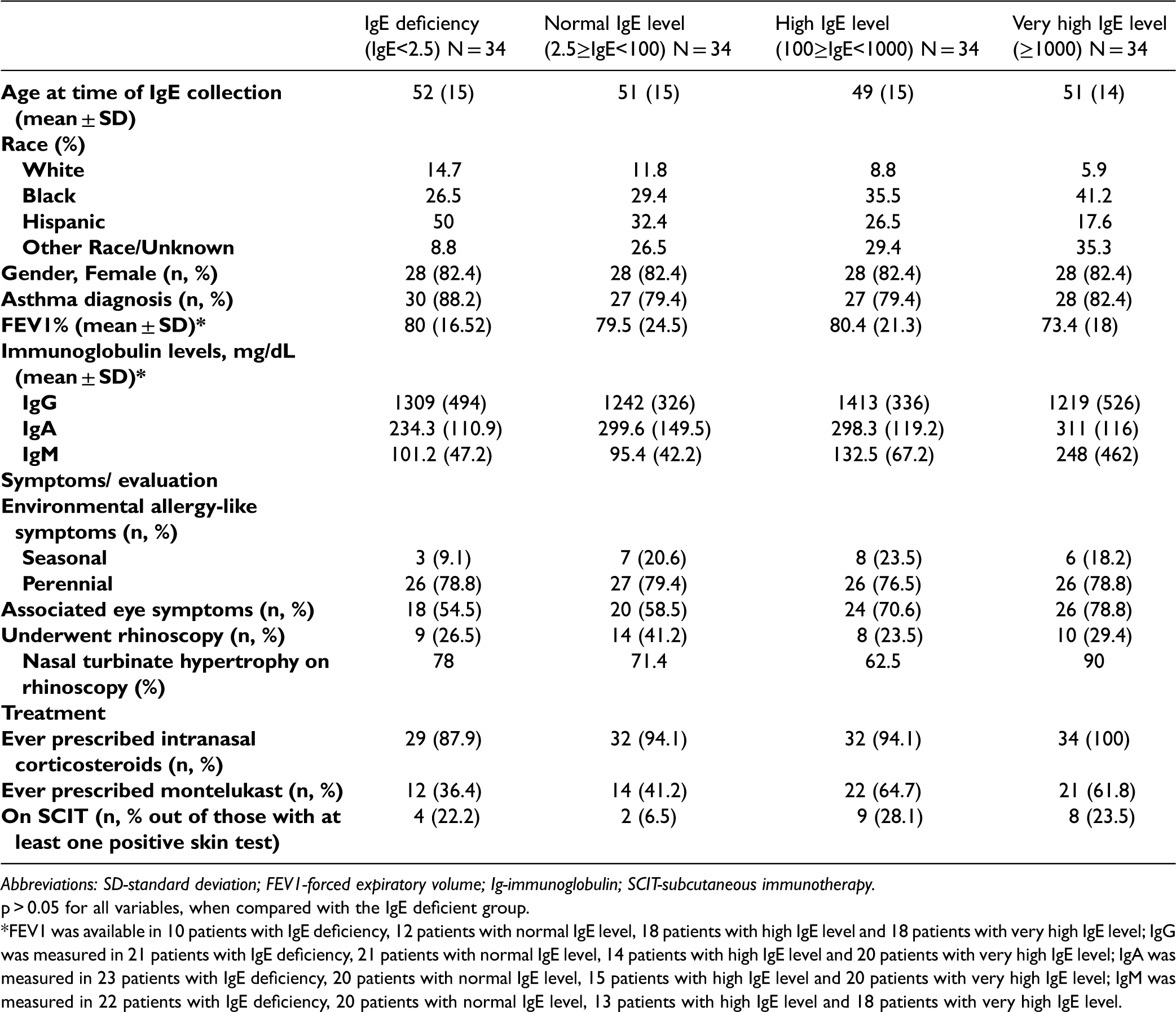
Abbreviations: SD-standard deviation; FEV1-forced expiratory volume; Ig-immunoglobulin; SCIT-subcutaneous immunotherapy.
p > 0.05 for all variables, when compared with the IgE deficient group.
*FEV1 was available in 10 patients with IgE deficiency, 12 patients with normal IgE level, 18 patients with high IgE level and 18 patients with very high IgE level; IgG was measured in 21 patients with IgE deficiency, 21 patients with normal IgE level, 14 patients with high IgE level and 20 patients with very high IgE level; IgA was measured in 23 patients with IgE deficiency, 20 patients with normal IgE level, 15 patients with high IgE level and 20 patients with very high IgE level; IgM was measured in 22 patients with IgE deficiency, 20 patients with normal IgE level, 13 patients with high IgE level and 18 patients with very high IgE level.
Patients with IgE Deficiency and Chronic Respiratory Symptoms Have a High Rate of Sensitization on Skin Testing
At least one positive skin test (SPT and/or IDST) was found in 52.9% (18/34) of patients with IgE deficiency. As expected, the rates of sensitization in patients with normal (91.2%, 31/34), high (94.1%, 32/34) and very high IgE levels (97.1%, 33/34) were significantly higher than in the IgE deficient cohort (p < 0.01). (Figure 2A) Overall, the IgE deficiency group had a mean of 4 ± 3 positive tests/patient, which was similar to patients with normal IgE levels (5 ± 3, p = 0.18), but significantly lower than in those with high (10 ± 3, p < 0.001) or very high IgE levels (11 ± 3, p < 0.001) (Figure 2B).
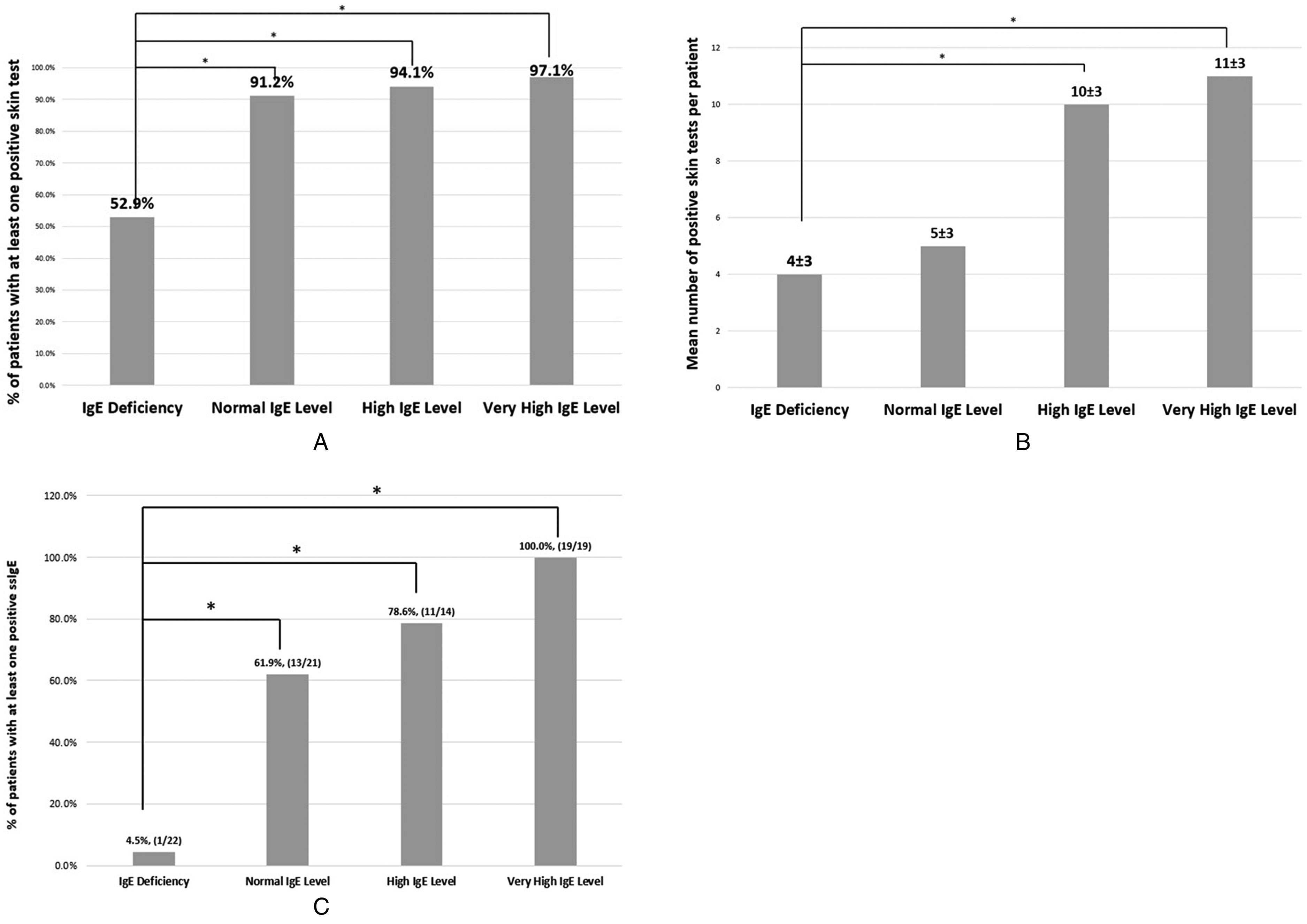
A. Overall positivity of skin tests in relation to IgE levels; B. Mean (±SD) number of positive skin tests per person; C. Overall positivity of ssIgE to environmental allergens. *p < 0.05, when comparing IgE deficient patients with Normal IgE level patients; IgE deficient patients with High IgE level patients; IgE deficient patients with Very High IgE level patients.
Aeroallergen Sensitizations Were Detected by Both SPT and IDST in IgE Deficient Patients
Figure 3A shows the distribution of positive SPT, IDST at low strength and IDST at high strength in the four groups. Positive SPT were detected in 8.8% (3/34) of IgE deficient patients, a rate significantly lower than in patients with normal (58.8%, 20/34, p < 0.001), high (88.1%, 30/34, p < 0.001) and very high (82.4%, 28/34, p < 0.001) IgE levels. A large proportion of IgE deficient patients had positive IDST at the low strength (20.6%, 7/34) which was significantly lower than patients with normal (61.8%, 21/34, p < 0.001), high (82.4%, 28/34, p < 0.001) or very high IgE levels (79.4%, 27/34, p < 0.001). Almost half of the IgE deficient individuals had positive IDST-high strength skin tests (47.1%). This rate was significantly different only from those with very high IgE levels (76.5%, p = 0.013). The rates of allergens sensitization in each of the four groups as found after performing all three types of skin tests are shown in Figure 3B. In IgE deficient individuals, the most prevalent positive skin tests were those to molds (32.4%) followed by tree pollen, dust mites, cockroach and cat allergens (23.5%).
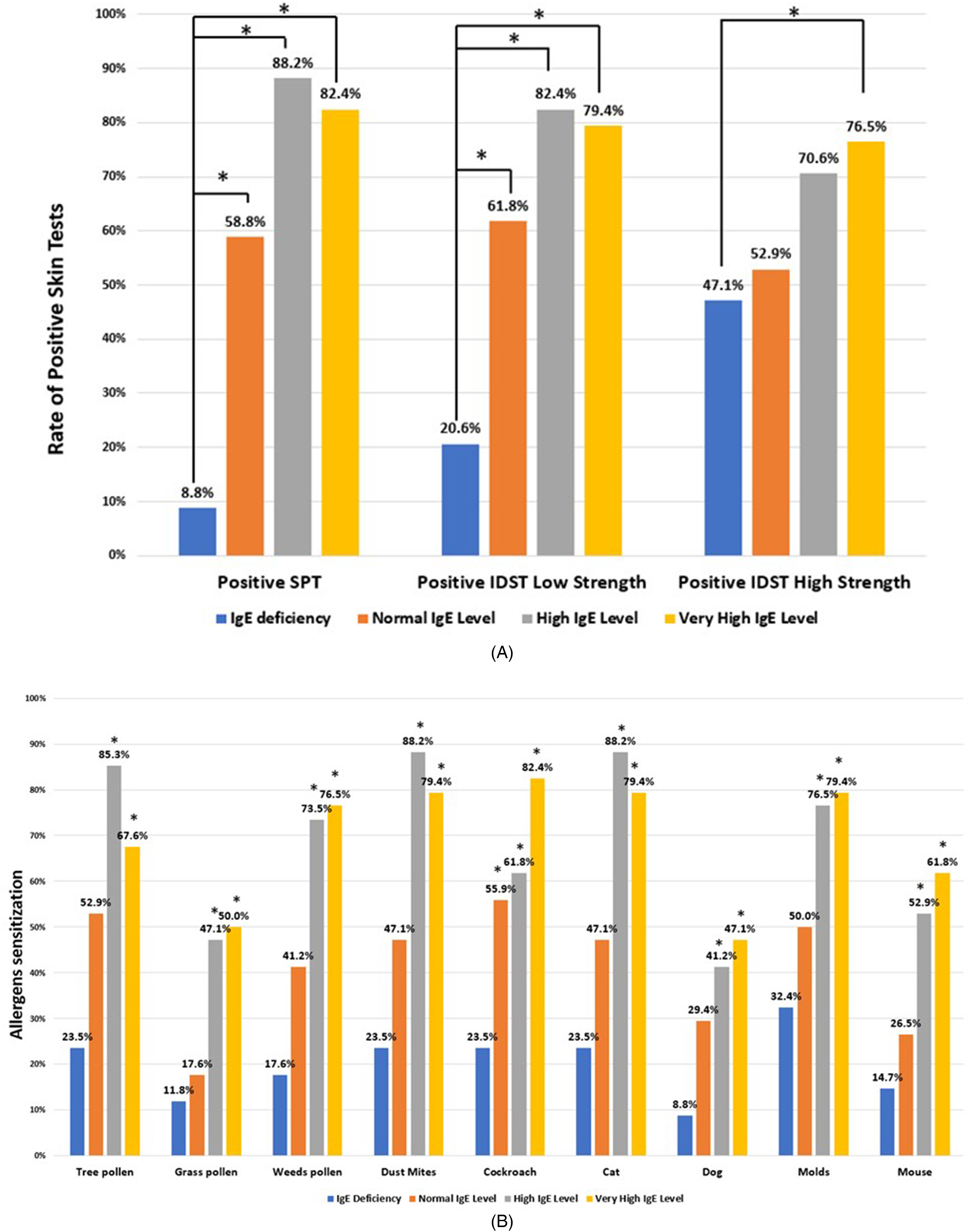
A.The rates of positive SPT and IDST in IgE deficient patients compared to those with normal, high and very high IgE levels. B. The rates of allergens sensitization in IgE deficient patients compared to those with normal, high and very high IgE levels. *p < 0.05, when comparing IgE deficient patients with Normal IgE level patients; IgE deficient patients with High IgE level patients; IgE deficient patients with Very High IgE level patients.
Serum specific IgE (ssIgE) testing was performed in 64.7% (22/34) of the IgE deficient patients (Figure 2C). Only one of the IgE deficient patients had detectable ssIgE (cockroach allergen [0.22 kU/L]). This patient also had a positive IDST at the low strength to the same allergen. Not surprisingly, ssIgE levels were significantly higher in all the other IgE subgroups than in the IgE deficient patients.
Immunotherapy status in the Analyzed Cohort
Overall, out of the 114 patients with at least one positive skin test, 23 patients (20.1%) had been placed on subcutaneous immunotherapy (SCIT). Four (4/18, 22.2%) of the IgE-deficient patients with at least one positive skin test were started on SCIT, a rate that was similar to those with normal (2/31, 6.5%, p = 0.215), high IgE (9/32, 28.1%, p = 0.255) and very high IgE levels (8/33, 23.5%, p = 0.07) (Table 1). The charts of patients receiving SCIT were reviewed for documentation of efficacy of immunotherapy. Overall, 5 patients stopped SCIT during the build-up phase (1 patients in the IgE deficiency group, 1 patient with normal IgE levels, 2 patients with high IgE levels and 1 patient with very high IgE measurements). According to provider's documentation, all 3 IgE-deficient patients on SCIT had significant improvement in their allergic rhinitis symptoms. The patient with normal IgE level on SCIT had persistent symptoms attributed to chronic rhinosinusitis. The majority of patients with high IgE levels had great improvement in their symptoms (6/7, 86%), while one patient with associated nasal polyps had minimal response to immunotherapy. Similarly, the majority of patients with very high IgE levels (6/7, 86%) who were on SCIT had improvement in their symptoms, while one patient with aspirin exacerbated respiratory disease had persistent respiratory disease.
Discussion
To the best of our knowledge, this is the first study characterizing the rate of environmental sensitizations in IgE deficient patients with environmental allergy-like symptoms who had complete evaluations with both SPT and IDST. Although these patients had very low or absent serum IgE levels, 52.9% of the IgE deficient individuals had at least one positive skin test after SPT and IDST were performed. The presence of positive skin tests in some of the IgE deficient patients suggests the existence of skin mast cell-bound IgE, despite very low IgE levels in the serum. These findings indicate that some of the environmental allergy-like symptoms seen in a large proportion of IgE deficient individuals,5,6,13,14 are type I hypersensitivity reactions which can be detected through a combination of SPT and IDST. Clinically, this is important, because in addition to medical management, the skin test results can be used to initiate SCIT, in a manner that is similar to non-IgE deficient individuals with environmental allergies. 12 Allergen immunotherapy may be equally helpful to IgE deficient individuals as it is to non-IgE deficiency individuals.
Immunoglobulin E differs from other immunoglobulins by having the lowest serum concentration and half-life, and being predominantly located in the tissues, bound to its high affinity mast cell receptors (FcεRI). 15 Class switch recombination and somatic hypermutation resulting in IgE synthesis and secretion occur in the lymph nodes draining the site of antigen entry, but IgE is also produced locally, at the site of the allergic inflammation.16–18 As a result, the vast majority of all IgE is found in the bound form 19,20 which traditional serum testing is unable to measure. The results of this study, demonstrating a discordance between serum and cell-bound IgE levels in many IgE deficient individuals, illustrate the inadequacy of using only serum IgE levels as a correct measurement of total body IgE. 21 On the other hand, a prior study showed that when the IgE levels where re-measured in 21 pregnant women with IgE deficiency (IgE<2 IU/mL) using a lower detection limit of 0.02 IU/mL (at this time in the clinical practice, for the majority of laboratories, the lowest limit of detection is 2 kU/L), all of them but one had detectable IgE levels ranging between 0.5 and 2.1 IU/mL. 14 Therefore, it appears that some IgE deficient patients produce enough IgE to prime mast cells, whereas others either produce no IgE at all or might produce IgE in very small amounts that cannot stimulate the mast cells during the skin tests placement. We demonstrate in this study, that by performing skin tests, we could detect aeroallergen sensitizations in more than half of IgE deficient patients presenting with environmental allergy-like symptoms, which may be used to initiate targeted environmental control measures and SCIT.
In contrast, half of IgE deficient individuals presenting with chronic respiratory symptoms had no detectable positive skin tests. There are a number of possibilities to explain the complete absence of allergic sensitization in these patients with chronic respiratory symptoms. For one, it is known that serum IgE levels can affect mast cell FcεRI expression. For example, in IgE-deficient mice, the expression of FcεRI on mast cells is only 20% of normal, 22 so it is possible that very low serum IgE levels in humans may also lead to downregulation of the high affinity IgE receptors, which might explain the negative skin tests in the rest of our cohort. It has also been suggested that IgE might have a protective mucosal effect, 23 so its absence in IgE deficient patients may contribute to chronic respiratory symptoms. Finally, the presence of exclusive local IgE production as has been described in local allergic rhinitis, 24 might explain the presence of respiratory symptoms in some of these IgE deficient patients.
Our study has several limitations. This was a relatively small, retrospective, observational chart review analysis which limits the generalizability of these results. However, this is the first study characterizing patients with IgE deficiency presenting for evaluation of environmental allergy-like symptoms, comparing the results of skin testing and ssIgE in this cohort with those individuals with normal, high and very high IgE levels. Moreover, because we included in the analysis only patients with selective IgE deficiency who presented with environmental allergy-like symptoms and who had all three sets of skin tests performed for complete assessment of their respiratory symptoms, we have been able to characterize a somewhat unique cohort of patients. Another possible limitation of the study is that using IDST to detect additional allergic sensitizations, raises the possibility that positive reactions were due to non-specific skin irritation rather than true allergic sensitizations. However, it is generally accepted that when SPT is negative despite a convincing clinical history, IDST for aeroallergens may be useful, particularly for assessing sensitization to low-potency aeroallergen extracts. 25 Furthermore, the fact that 52.9% of the IgE deficient patients had no reaction to the high strength IDST indicates that the test extract strengths used were not inherently irritating. At this time, there is no data about which is the right type of skin tests (SPT only vs. combination of SPT and IDST) to be used to detect environmental sensitizations in patients with IgE deficiency. Therefore, for a more comprehensive evaluation and to better describe IgE deficient individuals presenting for evaluation of environmental allergy-like symptoms, we chose to include in our studied cohort only patients who had all three skin tests performed (hence the limited sample size).
In conclusion, despite having absent or very low serum IgE levels, we have found that SPT and IDST are useful for detecting environmental sensitization in IgE deficient patients with allergy-like symptoms. These findings suggest the presence of cell-bound IgE in these individuals. Skin test results can be useful for initiating immunotherapy in appropriate individuals. Further research through larger prospective studies is needed to clearly establish the mechanisms through which some IgE deficient patients present with chronic respiratory symptoms, the exact significance of positive skin tests and to assess the benefits of allergen immunotherapy in these individuals.
Footnotes
Author Contributions
BC participated in chart review and manuscript preparation; YO participated in chart review; DR participated in manuscript preparation; DF participated in chart review and manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.