
Abstract
Background
Outside-in frontal drill out entails drilling the frontal sinus floor in the midline before identifying and dissecting the frontal recesses. It is a more direct approach, especially in revision surgery or cases with challenging anatomy.
Objectives
The aim of this study was to highlight the anatomical and surgical concepts for easy and safe outside-in frontal drill out by a preclinical anatomic study on cadaveric heads. In addition, to review our experience with this approach over a 5-year period for challenging frontal sinus pathologies.
Methods
The study included 2 sectors; a preclinical study, in which 5 cadaveric heads were dissected and studied to identify and standardize the anatomical landmarks of this approach. This was followed by a clinical case series which included 22 patients with challenging frontal sinus pathologies that were treated with this proposed approach.
Results
We concluded from the anatomic study that the nasal spine of the frontal bone (NSFB) and its anatomical orientation in relation to the nasal branch of the anterior ethmoidal artery (NBAEA) is a consistent landmark that enables the surgeon to identify the correct coronal trajectory of drilling to avoid injury of the cribriform and the skull base. The clinical case series included 22 patients that were successfully treated with the proposed approach. No intraoperative nor postoperative complications were reported in this study. Long-term follow-up showed that the frontal neo-ostium was patent in all cases (n = 22).
Conclusion
Outside-in frontal drill-out is a safe and easy approach; especially in challenging frontal sinus pathologies; using the NSFB and its anatomical coronal orientation to the NBAEA as a consistent landmark, anterior to the skull base. This approach offers early, safe, and direct bone removal without the need for initial identification and dissection of the frontal recess.
Introduction
Traditionally, the Draf III approach involves identification of the frontal recess, then widening from within the frontal recess, anteromedially towards the contralateral side to create a single horseshoe-shaped neo-ostium; frequently referred to as the “inside-out” technique. 1 This approach involves dissecting through inflamed mucosa, polyps, and stenotic scarred tissue at the start of the operation. This can cause excess bleeding and takes considerable time before starting drilling. Moreover, frontal recess anatomy may be challenging due to scarring, osteoneogenesis, or anatomical distortion.2,3
On the other hand, the “outside-in” technique (also known as the midline approach or trans-septal approach) entails drilling the frontal sinus floor in the midline before dissecting any inflamed mucosa, which minimizes bleeding and identifies the frontal sinuses properly before reaching the frontal recess.2,4 Drilling is performed in the frontal sinus floor anterior to the cribriform to avoid skull base injury. A good knowledge of the anatomical landmarks is crucial in order to identify the posterior limit of dissection to avoid skull base injury. 5
Many landmarks have been described including soft tissue and bony landmarks. The first olfactory nerve has been used in the literature as the most consistent landmark.2,4,6 The nasal branch of the anterior ethmoidal artery (NBAEA) has been also described as a landmark for the cribriform plate.3,5,6 Regarding bony landmarks, the cribriform plate has many openings: the olfactory foramina, the ethmoidal slit (ES), and the cribroethmoidal foramen (CF).7,8 The cribroethmoidal groove is a groove carrying the NBAEA after arising from the CF. 9
The increased interest in extended endonasal frontal sinus surgery parallels a renewed attention to local anatomy of the median aspect of the frontal sinus floor. During Draf III frontal sinusotomy, an individual dense bone is encountered anteriorly and medially. This piece of bone has been called spina nasalis interna by Halle, 10 spina nasalis superior by Hajek, 11 and spina nasalis (anterior) ossis frontalis by Lang. 9 Looking from below, during routine endonasal surgery, it can be identified as a bony projection at the midline of the floor of the frontal sinus. The perpendicular plate of the ethmoid articulates superiorly with the nasal spine of the frontal bone and during superior septectomy, disarticulation is always needed.
Although the outside-in approach has advantages over the classic Draf III approach, it is still not widely practiced. Also, there is no standardization of this approach and its anatomical landmarks. Accordingly, this work was carried out to cast a shadow over the anatomical and surgical concepts for easy and safe outside-in frontal drill out by using the NSFB as a consistent landmark. This was verified by a preclinical anatomic study on cadaveric heads. In addition, we reviewed our experience with this approach over a 5-year period for challenging frontal sinus pathologies.
Methods
This study was conducted over 5 years (March 2016-March 2021) in the Otorhinolaryngology Department, Mansoura University Hospitals (MUH), Egypt. The study included 2 sectors; a preclinical study, in which 5 cadaveric heads were dissected to identify and standardize the anatomical landmarks of the outside-in frontal drill-out. This was followed by a clinical case series which included 22 patients with challenging frontal sinus pathologies that were treated with this approach. Informed written consents were obtained from patients, and the study was approved by the Mansoura Faculty of Medicine Institutional Research Board (MFM-IRB: R.21.06.1355).
Preclinical Anatomic Study
Five cadaveric heads from voluntary body donators were provided by the University's Anatomy Department. The work was performed in the Surgical Lab of the Otolaryngology Department at MUH. All specimens underwent a multidetector computed tomography (CT) to confirm the anatomy and the pneumatization of the frontal sinuses.
Outside-in frontal drill-out was performed on the heads. The bony floor of the frontal sinus was exposed by elevation of an inverted U-shaped mucosal flap starting about 1 cm. anterior to the middle turbinate laterally, then across the roof of the nasal cavity, extending medially to the septum (Figure 1).
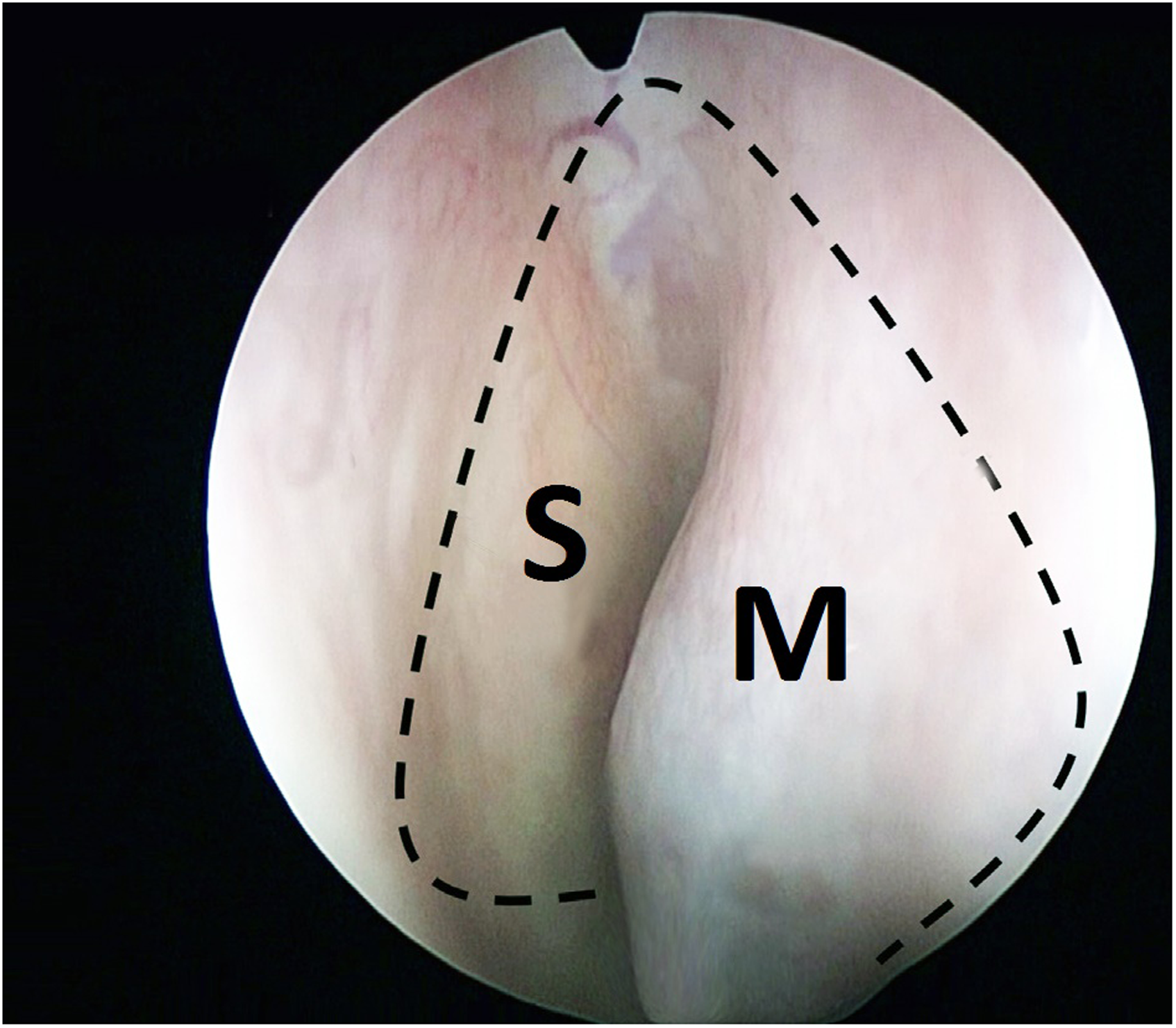
Endoscopic view showing the mucosal incision. S, septum; M, middle turbinate.
The first identified landmark was the NBAEA in the ethmoidal groove of the nasal bone (Figure 2A). The flap was detached posteriorly until the exit of the artery from the CF. Flap elevation was continued more posteriorly until the identification of the olfactory nerves. The NBAEA and the olfactory nerves were identified in all heads.
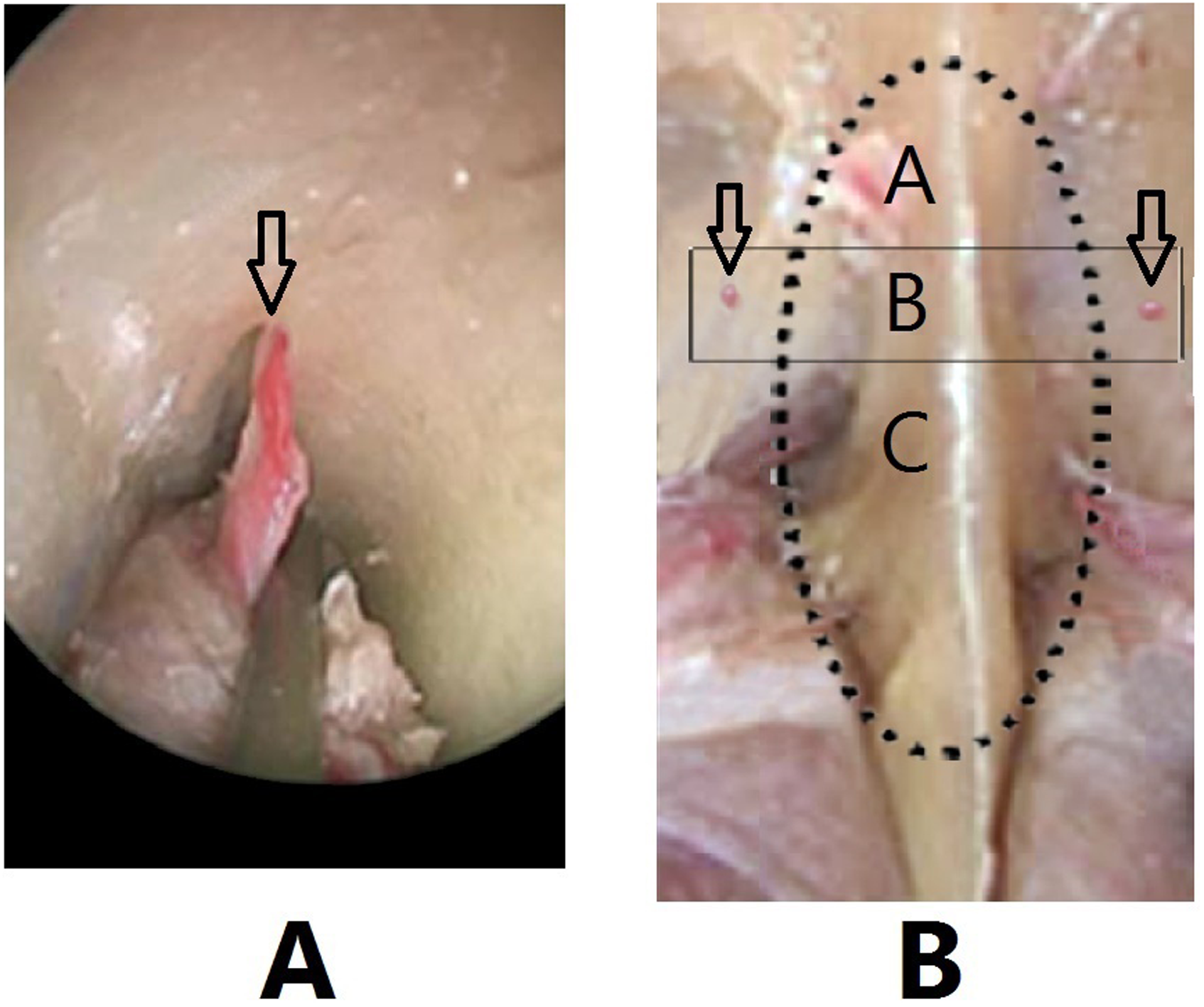
(A) The NBAEA (arrow). (B) The dotted line represents the NSFB. The arrows point to the CF containing the NBAEA. The rectangular area shows the correct coronal trajectory for safe drilling into the frontal sinus (zone B). Drilling anterior to this trajectory (zone A) will expose the dermis at the nasion, while drilling posterior to this trajectory (zone C) will cause skull base injury.
Regarding bony landmarks, the following structures were identified on each side of the perpendicular plate of the ethmoid. The most anterior landmark is the CF (Figure 2B), followed by the cribroethmoidal groove which runs in a posteromedial direction starting from the CF toward the ES. The CF and the cribroethmoidal groove were identified in 8 out of 10 sides of the 5 heads (80%). The ES and the foramina of the olfactory nerves were identified on the 10 sides (100%).
Disarticulation between the perpendicular plate and the NSFB was done to skeletonize the NSFB (Figure 2B). The superior parts of the perpendicular plate and the septal cartilage were resected (superior septectomy).
Drilling of the frontal sinus floor was then started in the midline; in the NSFB. To avoid skull base injury, drilling was done anterior to the cribriform plate, drilling started at the same coronal level of the CF, or the exit of the NBAEA (Figure 2B).
Once the frontal sinus was opened, it was widened by drilling or curved Kerrison rongeurs until the final horseshoe-shaped neo-ostium was created and enlarged to the maximum lateral and anteroposterior dimensions; from lamina papyracea to lamina papyracea and from the cribriform plate to the nasion.
The cadaveric study showed that the anatomic relationship of the NSFB to the NBAEA in the coronal plane is a consistent and reliable landmark demarcating the correct coronal trajectory into the midline of the frontal sinus floor anterior to the skull base.
Clinical Case Series
Outside-in frontal drill-out was performed in 22 patients. Identification of both the NBAEA and NPFB was the surgical keys that are relied upon for performing a safe procedure despite the challenging pathology and anatomy.
This study included 14 males and 8 females, with a mean age of 36.1 years (19-51 years). The indications were recurrent recalcitrant frontal sinusitis after previous failed surgeries (n = 9), inverted papilloma (n = 5), cerebrospinal rhinorrhea from frontal sinus posterior table defects (n = 3), frontal sinus osteoma (n = 2), frontal ossifying fibroma (n = 1), schwannoma in frontal sinus (n = 1), and frontal mucocele (n = 1).
Surgical Technique Tips
The procedure started with raising an inverted U-shaped mucosal flap to expose the frontal sinus floor by an incision starting 1 cm anterior to the axilla of the middle turbinate, extending medially onto the septum and laterally onto the lacrimal crest (Figure 3A). The flap was dissected posteriorly (Figure 3B). Bleeding was controlled with a monopolar tip if required. The flaps were then pushed posteriorly between the middle turbinate and the septum to avoid damage by the drill or microdebrider. The flaps were preserved to be used at the end of the procedure to cover exposed bone.

(A) The inverted U-shaped incision. (B) The mucoperiosteal flap dissection. (C) Identification of the NBAEA (the arrow) and the anterior ethmoidal nerve (the asterisk). (D) The multiple arrows point to the NSFB. The dotted line is the line of disarticulation between the perpendicular plate and the NSFB. The single arrow points to the NBAEA. The asterisk represents the anterior ethmoidal nerve that is sometimes identified as accompanying the NBAEA. The rectangular area is the correct and safe coronal trajectory for drilling.
Flap elevation continued posteriorly until the identification of the NBAEA (Figure 3C and D). The flap was dissected posteriorly until the exit of the NBAEA from the CF where it was coagulated and sectioned to continue flap elevation.
At this stage, disarticulation between the perpendicular plate of the ethmoid and the NSFB was done (Figure 3C), with performing a superior septectomy. Now the NPFB is clearly identified from both sides of the nose. Then, drilling of the NPFB was performed (Figure 4A) with a 30-degree endoscope and a 5-mm 15-degree diamond burr. Drilling was done in the same coronal plane of the NBAEA and the CF. Drilling was continued until the mucosa of the frontal sinus is identified and entered (Figure 4B).
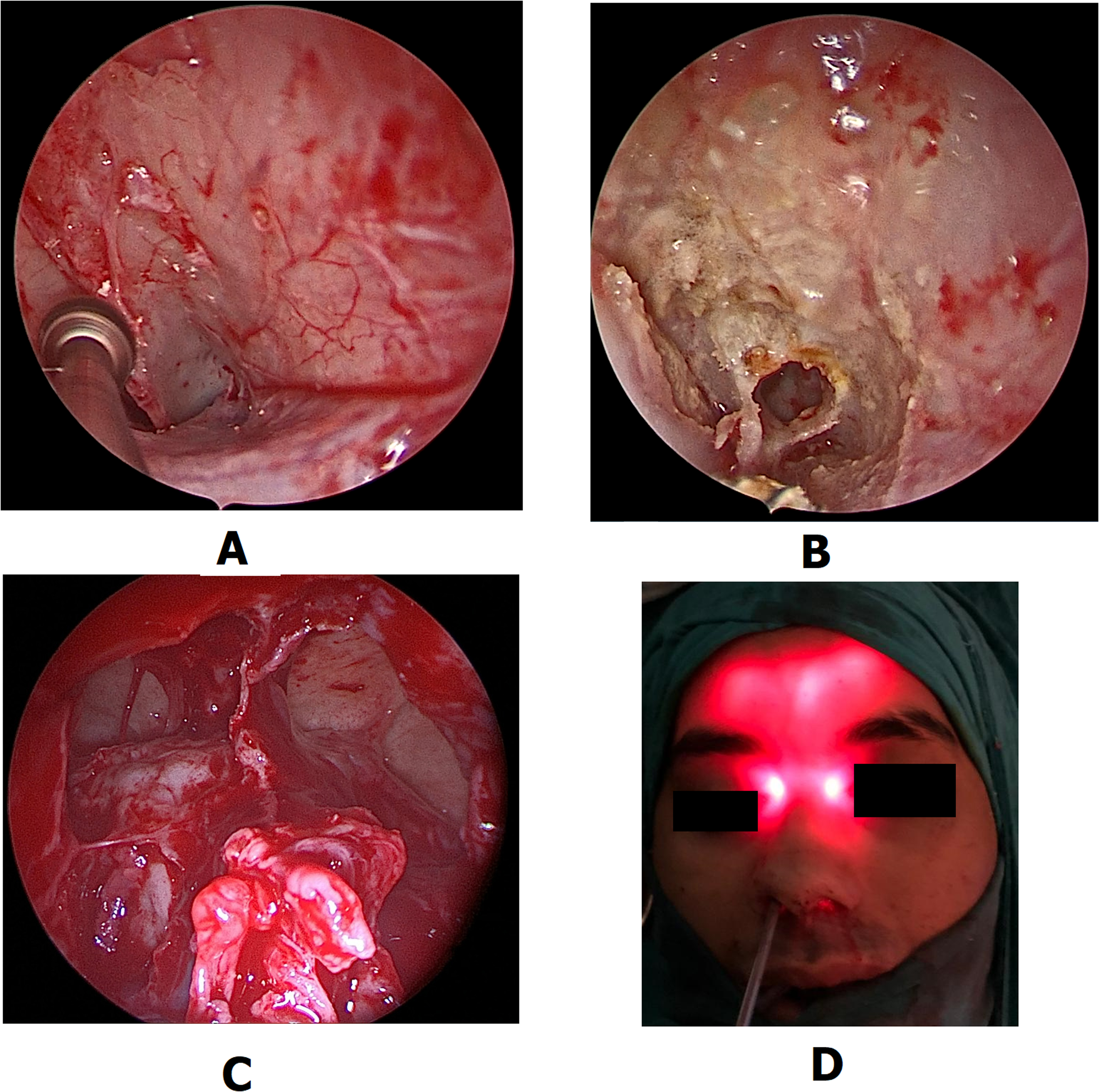
(A) Drilling of the nasal spine of the frontal bone (NSFB). (B) The first entry into the frontal sinus. (C) Safe widening of both frontal sinuses with creation of the single neo-ostium. (D) Intra-operative trans-illumination of the frontal sinus.
Once bilateral frontal sinuses were clearly visualized, any remaining frontal recess partitions and the interfrontal sinus septum were removed (Figure 4C). Bone was removed by the drill or Kerrison rongeurs. All interfrontal cells were effectively removed.
The mucosal flaps were used to cover the exposed bone to allow rapid healing. No frontal sinus stents were used in this study. At the end of the procedure, adequate hemostasis was achieved, and no nasal packing was performed.
Postoperative Care
Patients were discharged on the next postoperative day. Systemic antibiotics and analgesics were prescribed for one week. Saline irrigation was started on the first postoperative day and was maintained for several weeks until good healing is observed. Frequent endoscopic assessments in the outpatient clinic were scheduled, once per week. Removal of blood clots, crusts, and secretions was done. Assessment of the patency of the neo-ostium was observed.
Results
The approach was successfully performed in 22 patients. Patients’ clinical data are shown in Table 1.
Patients’ Data.
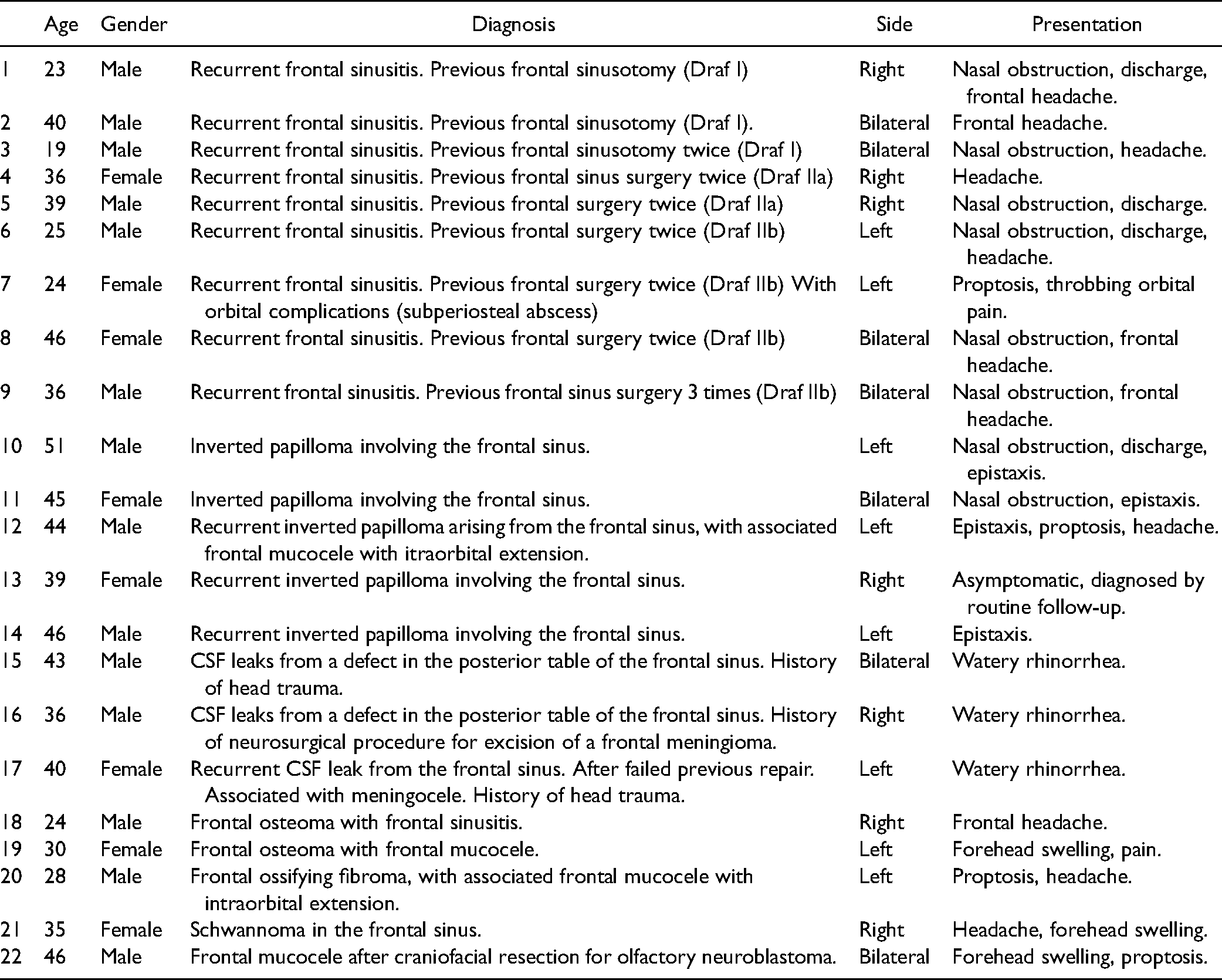
Nine patients (40.9%) had recurrent sinusitis involving the frontal sinus after multiple previous failed endoscopic surgeries. Scarring and/or osteoneogenesis of the frontal recess was detected in these 9 patients at the site of the previous surgeries. Five patients in this study (22.7%), had inverted papilloma involving the frontal sinus, either primary (n = 2) or recurrent (n = 3) after previous surgery. Three patients (13.6%) had CSF rhinorrhea with the defect located in the posterior wall of the frontal sinus. Two patients (9.1%) had frontal osteoma. One patient (4.5%) had a large frontoethmoidal ossifying fibroma, that was associated with a mucocele with intraorbital extension. One patient had a tumor in the frontal sinus that was proved to be schwannoma by histopathology. Lastly, one patient had bilateral frontal mucocele, with a history of craniofacial resection of olfactory neuroblastoma 12 years ago.
Operative time ranged from 55 to 195 min (average 112 min.). No intraoperative nor postoperative complications, in the form of orbital or intracranial injury or severe bleeding, were reported in this study. Follow-up period ranged from 14 to 60 months (average 40 months). Long-term follow-up showed that the frontal neo-ostium was patent in all cases (n = 22) (Figure 5). All patients (n = 22) were symptom-free in the follow-up period and no further surgical procedures were indicated.
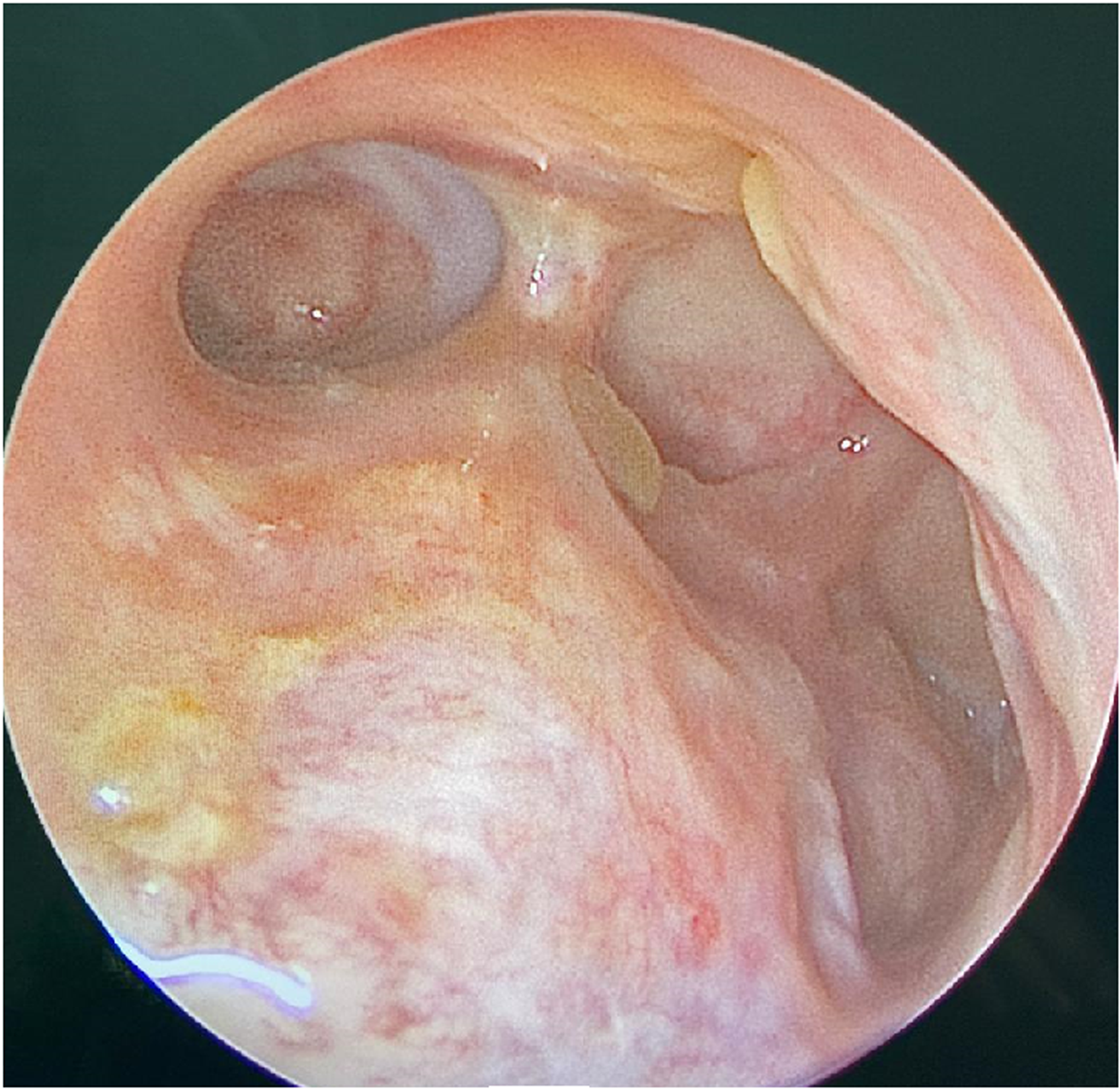
Postoperative endoscopic assessment showing long-term patency of the frontal sinusotomy.
Discussion
Draf III sinusotomy may involve difficulty in intraoperative identification of the frontal sinus, especially in revision surgery with lost anatomical landmarks, scarring, and reactive bone sclerosis.2,3 In these situations, the outside-in approach offers a more direct and safe approach without the need for initial identification of the frontal recess. This approach has been described before as the medial approach, 5 or the midline approach, 3 or the trans-septal approach, 4 or the outside-in frontal drill-out. 2 However, this approach is not widely practiced, and its landmarks are yet to be standardized.
The unfamiliarity of the surgeons with this approach may prompt anxiety because of the risk of injury to the cribriform plate and skull base. Familiarizing oneself with the anatomy of the cribriform plate and its landmarks gives the surgeon confidence in performing a safe outside-in frontal drill-out.
From Draf's first description of the Draf III procedure, the landmarks of the frontal drill-out remain unchanged. 12 Draf reported that the first olfactory nerve is an important landmark, and this landmark is still used widely in the literature.2,4,6 However, the olfactory nerve is not an ideal landmark for a few reasons. First, identifying the first olfactory fila can be challenging in some patients due to pathology or scarring in the olfactory cleft. Second, the anterior-most aspect of the olfactory fossa may extend anterior to the first olfactory fila, and, therefore, the skull base could still be injured. Third, dissection of the olfactory fila can cause CSF leak if the dural extension of the olfactory nerve sheath is violated. 13 In this study, the NSFB and its anatomical relationship with the NBAEA and the CF, was used as a safe and consistent anatomical landmark for the frontal sinus floor in the midline. In a radiological and cadaveric study by Craig et al, 13 it was confirmed that the NSFB almost always lies anterior to the olfactory fossa, and, therefore, its relationship makes it a safe and reliable landmark for avoiding skull base injury during frontal drill-out.
Lang 9 observed that the NSFB is encountered in nearly every paranasal sinus system. This work; whether in the anatomical study or the clinical series; confirms the previously mentioned data and the authors believe that the NPFB is a consistent bony landmark that is not properly defined in the literature in spite of being a key to safe midline entry to the floor of the frontal sinus. No reported significant anatomical variations of the NPFB have been recognized, making it a standard reference for surgeons performing outside-in frontal drill-out.
Some investigators have demonstrated the importance of the NBAEA in frontal sinus surgery.3,5,6 Sahu and Casiano 3 reported that this artery is consistently present, they identified this artery as it exits its bony canal anterior to the cribriform plate, in 11 cadaveric heads. In this study, the NBAEA was identified in all the cadaveric heads, as well as all cases.
Patron et al 5 concluded that the bony landmarks are consistent and reliable. The ES and the CF are important landmarks. They also concluded that the cribroethmoidal groove is an important landmark because it contains the NBAEA. Hooper 7 described the cribriform plate's foramina on dry skulls and revealed that ES is a consistent landmark. Similarly, Escalard et al 14 performed an anatomical study on dry skulls; ES was present on 92% of sides, and CF was present on 100% of sides. In our preclinical anatomic study on 5 cadaveric heads, the ES and the foramina of the olfactory nerves were identified on 100% (10 sides), however, both the CF and the cribroethmoidal groove were identified on 8 sides (80%).
Computer-assisted navigation can help in the identification of surgical landmarks intraoperatively. 2 There are however limitations to its use, including cost, availability, as well as the presence of disease obscuring anatomical landmarks. 5 The use of the NSFB as a fixed reliable anatomical landmark for safe access to the frontal sinus is very helpful for surgeons, especially when a navigation system is not available.
No complications were encountered in our series, this was similar to previous studies,2,4 in which no major complications were reported. Nishiike et al 4 reported a minor complication in the form of temporary olfactory disturbance postoperatively, but the symptom disappeared a few months after the stent was removed. This was attributed to the stent which changed the air current or caused crusting around the olfactory cleft. In our study stents were not preferred.
Conclusion
Outside-in frontal drill-out is a safe and easy approach; especially in challenging frontal sinus pathologies; using the NSFB and its anatomical coronal orientation to the NBAEA as a consistent landmark, anterior to the skull base. It is a more direct approach compared to the classic inside-out technique. It offers early, safe, and direct bone removal without the need for initial identification and dissection of the frontal recess which may be difficult and time consuming.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. This work was carried out in the Otorhinolaryngology Department, Faculty of Medicine, Mansoura University, Egypt.