
Abstract
Background
Eosinophilic chronic rhinosinusitis (ECRS) is a chronic inflammatory condition of the paranasal sinuses characterized by intractable nasal polyps with prominent eosinophil infiltration. These eosinophils are presumably recruited from peripheral blood via vessels expressing peripheral lymph node addressin (PNAd), a set of glycoproteins decorated with 6-sulfo sialyl Lewis x (sLex) glycans that serve as L-selectin ligands. Based on the severity classification algorithm proposed by the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) study group, ECRS is divided into mild, moderate and severe groups; however, as yet there are few reports comparing the clinicopathological differences among these groups.
Objective
Our goal was to elucidate clinicopathological differences among the three different severities of ECRS with special reference to eosinophils and PNAd-expressing vessels.
Methods
We performed quantitative immunohistochemical analysis of PNAd-expressing vessels using surgical specimens of nasal polyps from patients exhibiting varying severity of ECRS (n = 35) and from individuals with non-ECRS (n = 10). To this end, we immunostained tissue sections with anti-PNAd and anti-CD34 monoclonal antibodies, and then determined the number of vessels immunolabeled with each antibody.
Results
The number of eosinophils infiltrating nasal polyps was correlated with ECRS severity. We also found that the PNAd + /CD34 + vessel ratio, namely, the percentage of PNAd-expressing vessels among all vessels, was positively correlated not only with ECRS severity but also with the number of eosinophils infiltrating nasal polyps formed in ECRS.
Conclusion
These results strongly suggest that PNAd-expressing vessels play at least a partial role in eosinophil recruitment to nasal polyps and consequent severity of ECRS.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a disease commonly seen in the daily practice of otorhinolaryngology. It is characterized by headache, posterior nasal drip and deposition of inflammatory exudate mainly in the maxillary sinus. Besides conventional CRS, otorhinolaryngologists sometimes detect CRS with intractable nasal polyps in the ethmoid sinus, which can cause olfactory disturbance and nasal obstruction. 1 While the mechanism underlying the formation of these refractory polyps is not fully understood, the polyps are resistant to antimicrobial agents but responsive to systemic steroids. Therefore, treatment of CRS with nasal polyps (CRSwNP) includes surgical removal of polyps by endoscopic sinus surgery (ESS) and systemic steroid administration to prevent their recurrence. 2
Histologically, refractory nasal polyps formed in CRSwNP are often infiltrated by a significant number of eosinophils. 3 In 2015, the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) study group focused on this histological feature and proposed diagnostic criteria for eosinophilic CRS (ECRS). 4 According to these criteria, ECRS is classified into three groups: mild, moderate, and severe (Figure 1 and Table 1). It is reasonable to assume that nasal polyps will more likely recur in severe ECRS and that histopathological differences underlie different severities of ECRS; however, as yet there is no quantitative histological analysis to support these conclusions.
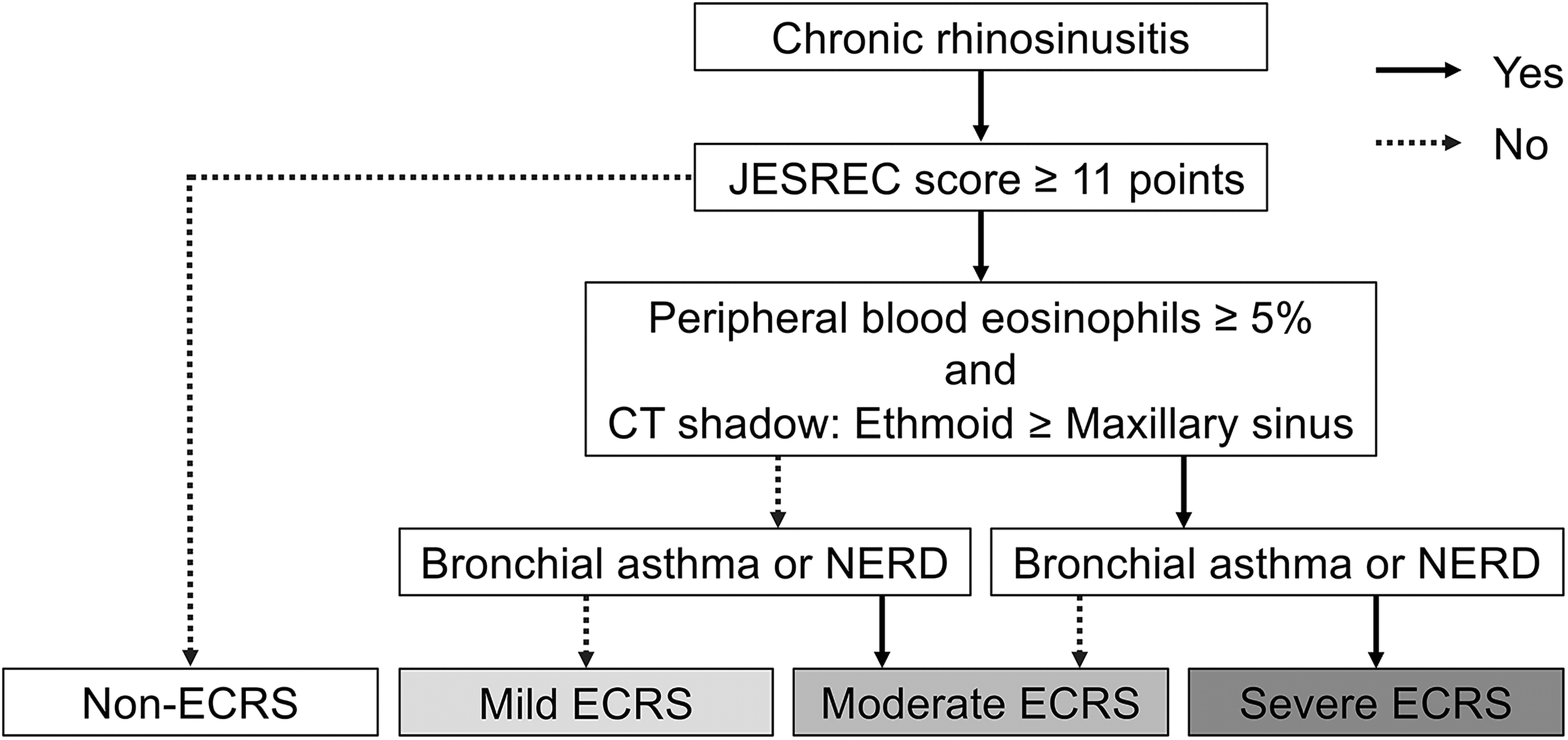
A partially modified version of the diagnostic flowchart proposed by the JESREC study group to determine ECRS severity. First, individuals who do not meet ECRS diagnostic criteria (ie, the sum of each criterion in Table 2 is less than 11 points) are classified as non-ECRS. Second, those who do meet diagnostic criteria (ie, the sum of each criterion in Table 2 is 11 points or more) are classified as having mild, moderate, or severe disease.
Criteria for the JESREC Score a .
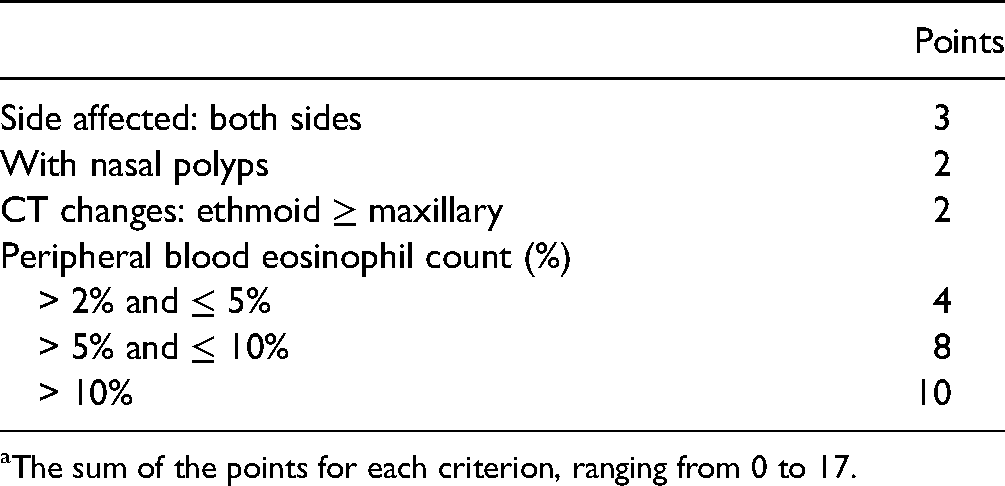
The sum of the points for each criterion, ranging from 0 to 17.
Univariate Analysis of Clinical Information Relevant to Cases Examined in This Study.
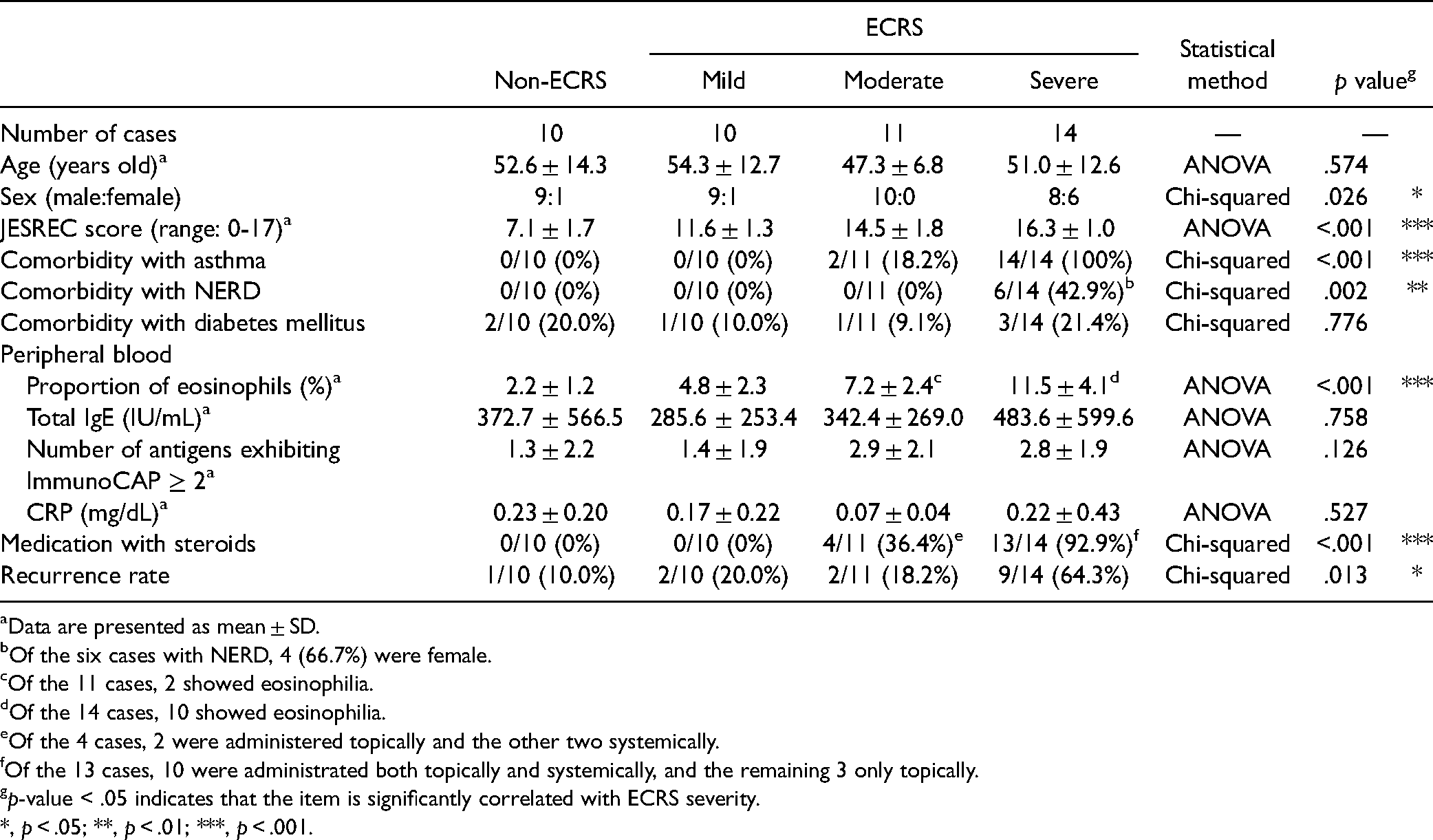
Data are presented as mean ± SD.
Of the six cases with NERD, 4 (66.7%) were female.
Of the 11 cases, 2 showed eosinophilia.
Of the 14 cases, 10 showed eosinophilia.
Of the 4 cases, 2 were administered topically and the other two systemically.
Of the 13 cases, 10 were administrated both topically and systemically, and the remaining 3 only topically.
p-value < .05 indicates that the item is significantly correlated with ECRS severity.
*, p < .05; **, p < .01; ***, p < .001.
L-selectin and its ligands reportedly function at least partially in the “rolling” of eosinophils along the vessel wall, an important step that is a prerequisite for eosinophil recruitment.5–8 The L-selectin ligand has been shown to be a set of sialomucins whose carbohydrate moieties are capped with 6-sulfo sialyl Lewis x (sLex) structures, collectively referred to as peripheral lymph node addressin (PNAd). 9 Under physiological conditions, PNAd is constitutively expressed on high endothelial venules (HEVs) in secondary lymphoid organs, and researchers have used the MECA-79 monoclonal antibody to detect these vessels. 10
We previously showed that PNAd is induced on vessels in nasal polyps associated with CRS, and that the percentage of PNAd-expressing vessels in ECRS is significantly greater than that seen in non-ECRS. 8 These PNAd-expressing vessels often exhibit eosinophils attached to their luminal surfaces, which are presumed to be in the process of infiltration. We also previously showed that the percentage of PNAd-expressing vessels is positively correlated with the degree of chronic inflammation in various chronic inflammatory diseases other than ECRS, such as chronic Helicobacter pylori gastritis,11,12 ulcerative colitis,13,14 and benign prostatic hyperplasia-associated chronic prostatitis. 15 Thus, it is reasonable to hypothesize that the greater the percentage of PNAd-expressing vessels, the greater the number of eosinophils infiltrating nasal polyps and the consequent severity of ECRS.
To test this hypothesis, in the present study we performed quantitative immunohistochemical analysis of PNAd-expressing vessels using nasal polyp tissues from patients showing various severity of ECRS and non-ECRS, with special reference to the number of infiltrating eosinophils.
Materials and Methods
Patients and Tissue Samples
Eligible patients had undergone ESS for CRSwNP at the University of Fukui Hospital, from January 2016 to December 2020. Formalin-fixed, paraffin-embedded (FFPE) tissue blocks of surgically resected nasal polyps from these patients were collected from the pathology archives. Diagnosis and severity of ECRS were assessed according to the JESREC criteria (Figure 1 and Table 1). 4 Consequently, 10 cases of non-ECRS, 10 cases of mild ECRS, 11 cases of moderate ECRS, and 14 cases of severe ECRS were included in the analysis. Analysis of human nasal polyp tissues was approved by the Research Ethics Committee of the University of Fukui (reference number 20150041, approved on October 6, 2015). Written informed consent was obtained from all patients.
Immunohistochemistry
Monoclonal antibodies used as primary antibodies were QBEND10 (mouse IgG; Immunotech, Marseille, France) directed against human CD34, which is a marker of vascular endothelial cells, 16 and MECA-79 (rat IgM; BD Biosciences, Franklin Lakes, NJ), which recognizes 6-sulfo N-acetyllactosamine attached to extended core 1 O-glycans that constitutes PNAd.10,17 Immunohistochemical staining for CD34 was performed using the Histofine system (Nichirei Biosciences, Tokyo, Japan) as per the manufacturer's protocols, 18 and that for PNAd was conducted using an indirect method previously described. 8
Counting of Eosinophils in Tissue Specimens
We first examined hematoxylin and eosin (H&E)-stained tissue specimens under a light microscope and identified three high-power fields (HPFs) of view (using x400 magnification) with the highest number of eosinophils (“hot spots”). We then counted eosinophils in these three areas without knowledge of clinical information. The average number of eosinophils per HPF served as the eosinophil count of each sample.
Quantification of PNAd-Expressing Vessels
We first scanned the entire area of tissue specimens immunostained for PNAd and identified three “hot spots” of PNAd-positive vessels at a magnification of x200. We then determined the number of PNAd-positive vessels in the 3 areas without knowledge of clinical information. The number of CD34-positive vessels in the corresponding areas was also determined. For each sample, the number of PNAd-positive vessels was divided by the number of CD34-positive vessels to calculate the percentage of PNAd-positive vessels among all vessels (the PNAd + /CD34 + vessel ratio).
Statistical Analysis
Correlations between ECRS severity and eosinophil number or the PNAd + /CD34 + vessel ratio were statistically analyzed by one-way analysis of variance (ANOVA) with a Tukey-Kramer post hoc test. Differences between severe ECRS with and without NERD were statistically analyzed by Student's t-test. The correlation of the PNAd + /CD34 + vessel ratio with eosinophil number was statistically analyzed by simple linear regression analysis. All statistical analyses were done using JMP 16 software (SAS Institute, Cary, NC). p-values less than .05 were considered significant.
Results
Cases of Severe ECRS Show Significantly Higher Recurrence Rate
We first analyzed the clinical characteristics of patients showing differing ECRS severities (Table 2 and Supplemental Table 1). There was no difference in average age among groups, but the proportion of females was significantly higher in severe ECRS compared to other groups, presumably due to the higher prevalence of non-steroidal anti-inflammatory drug (NSAID)-exacerbated respiratory disease (NERD) in females. 19 Patients with severe ECRS had a higher incidence of asthma and NERD and a higher proportion of eosinophils in peripheral blood, possibly due to the inclusion of these items in the JESREC criteria used to determine ECRS severity. 4 While total IgE levels and the number of specific antigens revealed by ImmunoCAP 20 did not differ among groups, the number of patients who received preoperative steroids was significantly greater in severe ECRS. There was no difference in the number of diabetic patients or in levels of serum C-reactive protein (CRP) among groups. It is noteworthy that the postoperative recurrence rate was significantly higher in cases of severe ECRS (64.3%) than in other groups. Given that recurrence rates of mild (20.0%) and moderate (18.2%) ECRS did not differ, we combined these two groups into a single “mild/moderate” ECRS group for the following analyses.
Eosinophil Number Is Correlated with ECRS Severity
Here, we analyzed cases with a pathologically confirmed diagnosis of ECRS, although disease severity varied. Thus, all cases met the histological criteria for ECRS, namely, an average of ≥70 eosinophils in three HPFs analyzed at x400 magnification. 4 However, based on H&E staining, the number of eosinophils infiltrating nasal polyps in severe ECRS appeared to exceed that seen in mild/moderate or non-ECRS (Figure 2, left column). To confirm that observation, we then counted eosinophils shown in the analysis in Figure 2 (left column) and performed a one-way ANOVA comparing their number across various conditions of ECRS severity. As shown in Figure 3 (left panel), the number of eosinophils was correlated with ECRS severity (F = 8.967, p < .001). Moreover, when severe ECRS cases were further subdivided as those with and without NERD, the number of eosinophils in the former exceeded that in the latter with high statistical significance (p < .001) (Figure 3, right panel).

Induction of PNAd-positive vessels in nasal polyps. Serial tissue sections of nasal polyps formed in non-ECRS (top row), mild/moderate ECRS (middle row) and severe ECRS (bottom row) were stained with hematoxylin and eosin (H&E) (left column) or immunostained using antibodies to the vascular endothelial cell marker CD34 (middle column) or to PNAd (right column). Signals on tissue sections in the middle and right columns were visualized with 3,3′-diaminobenzidine (DAB) (brown), and tissues were counterstained with hematoxylin. Representative cases are shown. Note that a greater number of eosinophils (left column, arrows) infiltrate and more PNAd-positive vessels (right column, arrowheads) are induced in severe ECRS than in mild/moderate- or non-ECRS. Bar = 50 μm. Negative control images using isotype-matched immunoglobulins are shown in Supplemental Figure 1.
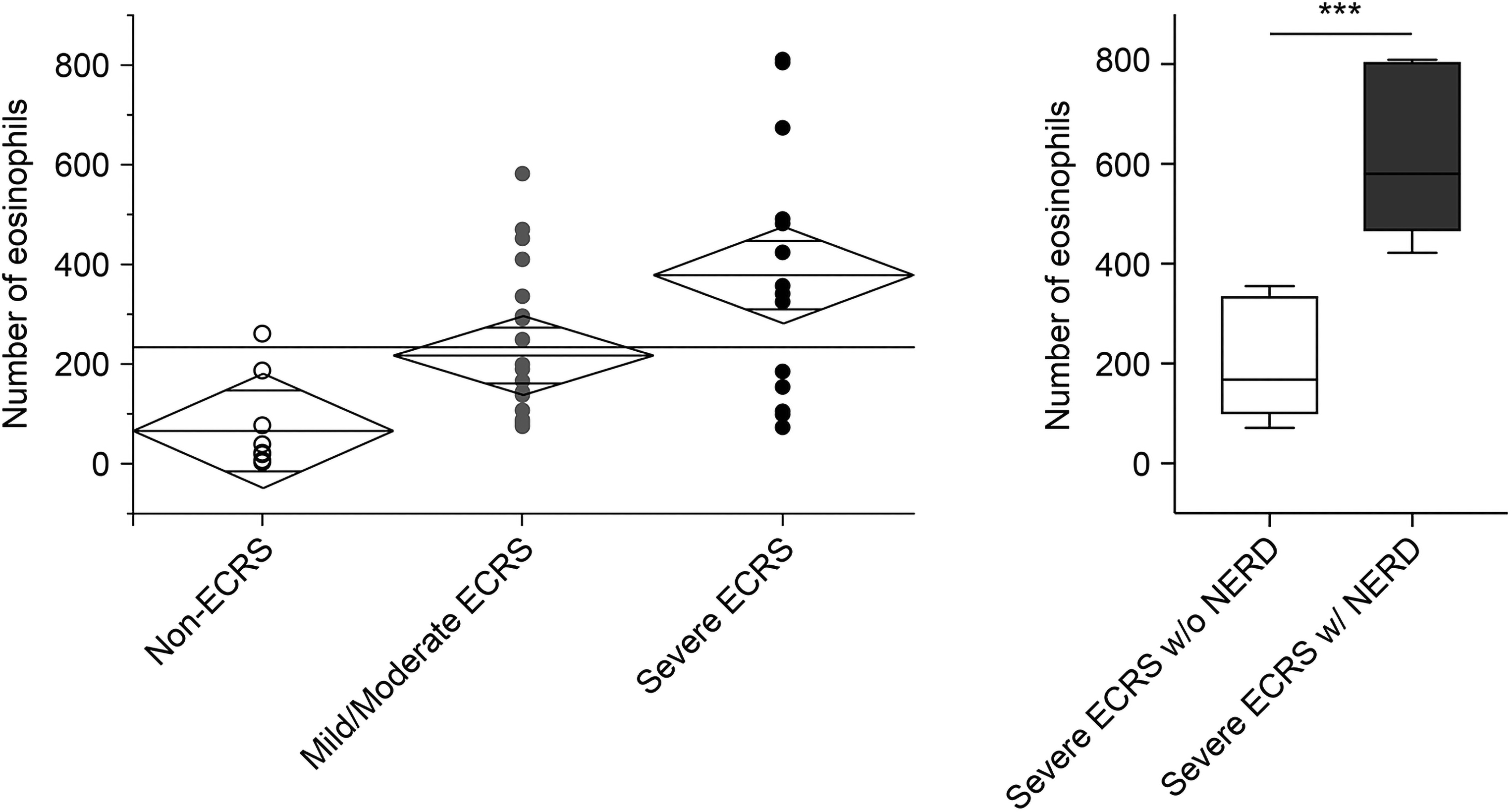
Correlation between the number of eosinophils infiltrating nasal polyps and ECRS severity. (Left) Scatter plot representing one-way ANOVA analysis of the number of eosinophils per HPF (y-axis) based on ECRS disease severity (x-axis). Eosinophil number was determined by counting eosinophilic granulocytes on H&E-stained tissues in all 3 severity groups (n = 10 for non-ECRS, n = 21 for mild/moderate ECRS and n = 14 for severe ECRS). The vertical span of each diamond represents the 95% confidence interval (CI) for each group. Center lines across each diamond correspond to group means. (Right) The number of eosinophils in severe ECRS without (w/o; open box) and with (w/; closed box) NERD. Data are presented in a box-and-whisker diagram. ***, p < .001.
The Percentage of PNAd-Positive Vessels Is Correlated with ECRS Severity
As noted in the Introduction, we hypothesized that the greater the ECRS severity, the greater the number of vessels that would express PNAd. To test this hypothesis, we immunostained nasal polyp tissue sections with antibodies to PNAd and the vascular endothelial cell marker CD34. We observed that all blood vessels in the tissue were immunolabeled for CD34 (Figure 2, middle column), whereas only some were PNAd-positive (Figure 2, right column). We note that the absolute number of PNAd-positive vessels cannot be simply compared between groups, as vascularity (the number of vessels per unit area) and polyp size (the area of tissue specimens) vary from sample to sample. Thus, we calculated the proportion of PNAd-positive vessels among all vessels (the PNAd + /CD34 + ratio), and compared that value among groups. Accordingly, as shown in Figure 4 (left panel), the mean PNAd + /CD34 + vessel ratio of severe ECRS was greater than that of mild/moderate ECRS or non-ECRS, and the PNAd + /CD34 + vessel ratio appeared to increase with increasing severity of ECRS. To test this possibility, we conducted a one-way ANOVA comparing the PNAd + /CD34 + vessel ratio across various severities of ECRS and found that the PNAd + /CD34 + vessel ratio was correlated with ECRS severity (F = 4.681, p = .015). However, in the analysis of severe ECRS, the PNAd + /CD34 + vessel ratio did not differ significantly between cases with or without NERD (Figure 4, right panel), a finding that was unanticipated.
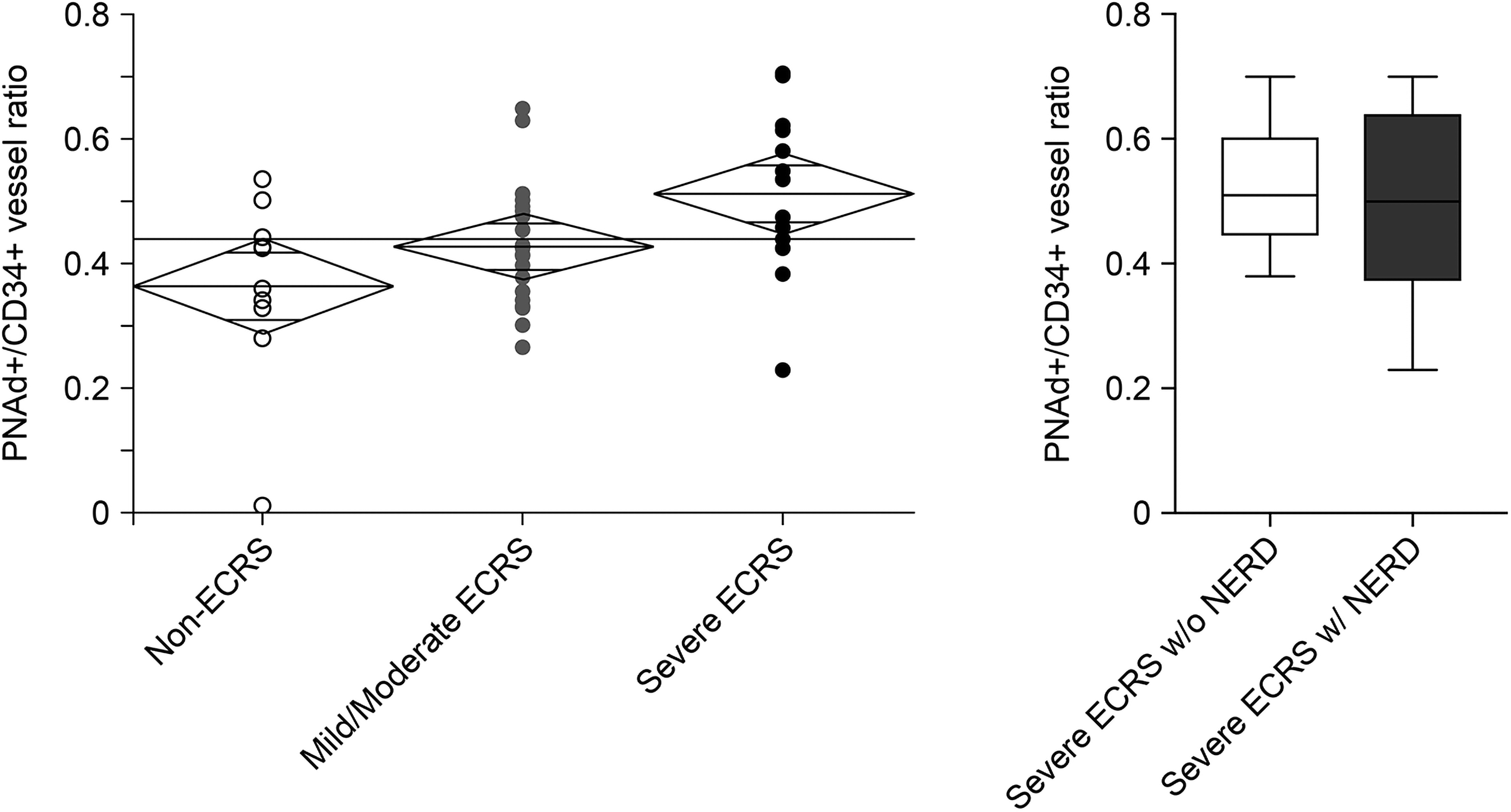
Correlation between percentage of PNAd-expressing vessels and ECRS severity. (Left) Scatter plot representing one-way ANOVA analysis of the PNAd + /CD34 + vessel ratio (y-axis) based on ECRS disease severity (x-axis). The vertical span of each diamond represents the 95% confidence interval (CI) for each group. Center lines across each diamond correspond to group means. (Right) The PNAd + /CD34 + vessel ratio in severe ECRS without (w/o; open box) and with (w/; closed box) NERD. Data are presented in a box-and-whisker diagram.
Eosinophil Number Positively Correlates with the PNAd + /CD34 + Vessel Ratio
Based on the above findings, we asked whether the number of eosinophils infiltrating nasal polyps is correlated with the PNAd + /CD34 + vessel ratio using linear regression analysis. As expected, a simple linear regression analysis revealed a positive correlation between the PNAd + /CD34 + vessel ratio and eosinophil number (Figure 5). This result indicates that the PNAd + /CD34 + vessel ratio could be used to estimate the number of infiltrating eosinophils.
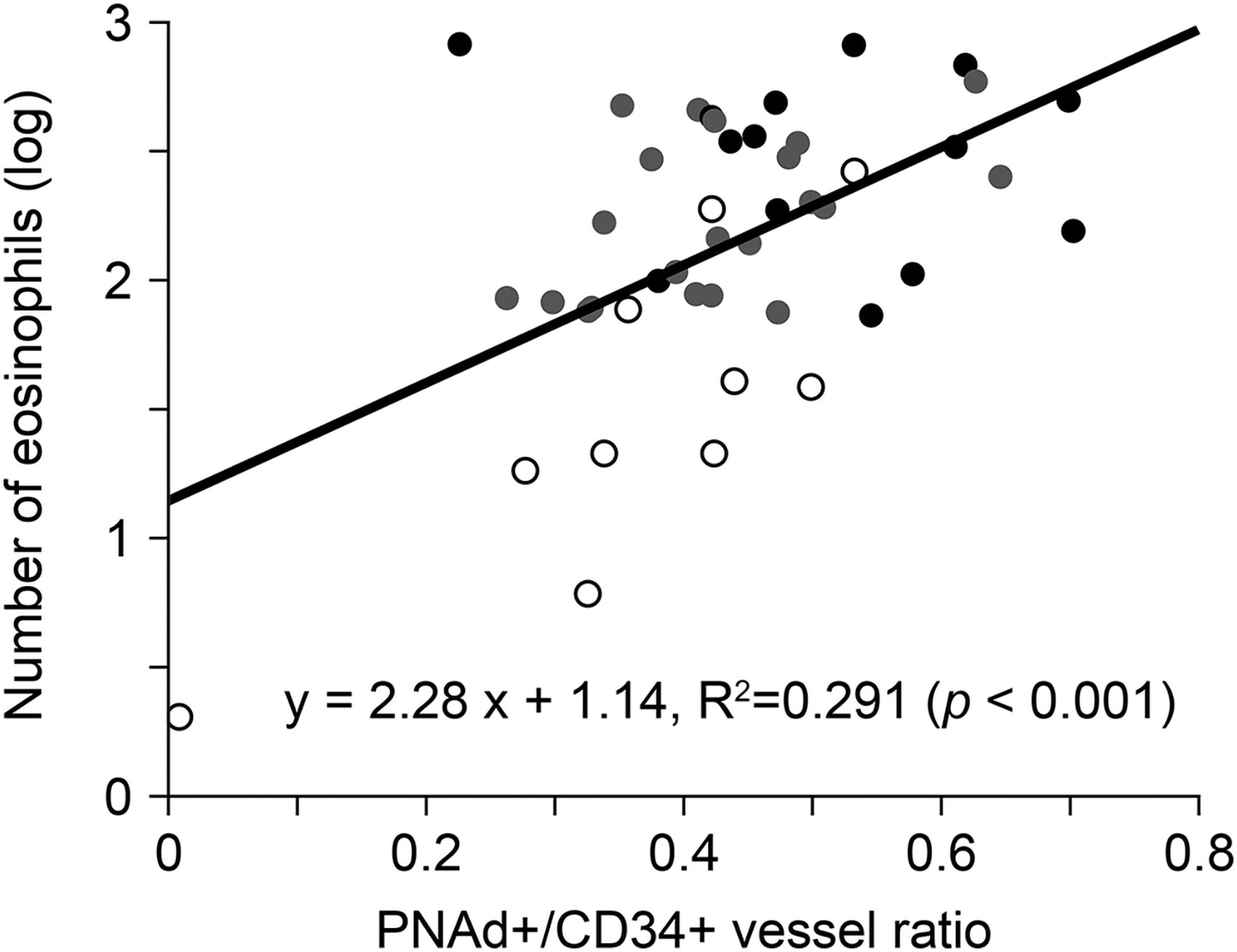
Linear regression analysis showing the correlation between PNAd + /CD34 + vessel ratio and the number of eosinophils infiltrating nasal polyps. Note that the y-axis showing the eosinophil number is drawn to log scale. White, gray, and black dots represent non-ECRS, mild/moderate ECRS and severe ECRS, respectively.
Discussion
Here, we demonstrated that the number of eosinophils infiltrating nasal polyps is correlated with ECRS severity. We also showed that the percentage of PNAd-expressing vessels, as indicated by the PNAd + /CD34 + vessel ratio, is correlated not only with ECRS severity but also with the number of eosinophils. Taken together, these findings suggest that PNAd may be at least partially responsible for eosinophil mobilization into nasal polyps formed in ECRS and for disease severity.
One might conclude that not only the PNAd + /CD34 + vessel ratio but also the absolute number of PNAd + and CD34 + vessels would correlate with eosinophil count. Results of linear regression analysis indicated that both the absolute number of PNAd + and CD34 + vessels indeed did correlate with eosinophil count, but the variance was too large to be practically useful to estimate eosinophil count (y = 0.012 x + 1.963, R2 = 0.024, F = 1.064, p < .001 for the former, and y = −0.009 x + 2.437, R2 = 0.060, F = 2.750, p < .001 for the latter). However, by dividing the number of PNAd + vessels by the number of CD34 + vessels, the variance converged and the resulting parameter was judged useful to estimate the infiltrating eosinophil count.
Clinically, it is noteworthy that we found that the postoperative recurrence rate of severe ECRS was significantly higher than that of less severe ECRS (see Table 2). Gion et al. recently compared characteristics of patients showing different ECRS severity, 21 and their observations were comparable to what we report here. For example, serum IgE levels, the proportion of eosinophils in peripheral blood, and comorbidity with asthma in severe ECRS were higher than those values seen in less severe ECRS. However, they did not compare postoperative recurrence rates among groups of differing ECRS severity. Although the histological criteria for ECRS proposed by the JESREC study group are useful in predicting ECRS recurrence risk per se regardless of the disease severity, it is important to note that patients with severe ECRS are at a particularly high risk of recurrence.
Thus far, two molecular interactions have been implicated in the “rolling” step of eosinophil recruitment to inflammatory sites: one is the interaction between L-selectin expressed on eosinophils and PNAd on vascular endothelial cells,5–8 and the other is that between sLex on eosinophils and E and/or P-selectin expressed on vascular endothelial cells.22–26 Here, we focused on the former in terms of ECRS development, but it remains unclear to what extent each mechanism contributes to ECRS pathogenesis. We recently developed a monoclonal antibody against E-selectin, designated U12-12, that can be used on FFPE tissue sections. 27 We then used this antibody to immunostain tissue sections from nasal polyps formed in ECRS to assess the potential expression of E-selectin on mucosal vessels in these polyps. However, only a small number of vessels in nasal polyps formed in ECRS were stained by this antibody (data not shown). This result suggests that E-selectin is minimally involved in eosinophil infiltration, at least in ECRS, although further studies are needed to define the extent to which P-selectin functions in ECRS pathogenesis.
An intriguing finding reported here is that while the number of eosinophils in severe ECRS with NERD was significantly greater than that seen in those without NERD, the percentage of PNAd-positive vessels did not differ between these two groups. This finding is consistent with the results of Ebbens et al., who found that the number of eosinophils in asthma patients with nasal polyps and exhibiting acetylsalicylic acid intolerance was significantly greater than that seen in patients with nasal polyps without these complications, although they observed no statistically significant difference in the percentage of PNAd-positive vessels. 7 One explanation for this outcome is that the presence of NERD facilitates one or more of the three steps that occur after the “rolling” step: namely, (i) chemokine-dependent eosinophil activation, (ii) firm attachment of eosinophils to endothelial cells, or (iii) eosinophil extravasation. Further studies are needed to investigate which step(s) may be more efficiently triggered and by what mechanism.
Fujieda et al. recently reported that dupilumab, a biologic that inhibits the IL-4 and IL-13 pathways, significantly improves symptoms in severe CRSwNP, regardless of ECRS status. 28 This result suggests that factors that correlate with ECRS status, such as blood eosinophil count, do not necessarily correlate with the efficacy of dupilumab in CRSwNP. Although none of the cases examined in the present study used dupilumab, it would be of interest to examine whether the percentage of PNAd-expressing vessels affects the efficacy of this biologic in CRSwNP.
There are some limitations to the present study. Since the number of cases analyzed was relatively small, the conclusions drawn should be supported by an analysis of a larger number of cases, and a multicenter study is needed for this purpose. In addition, even if their preoperative JESREC score was ≥11, cases that did not meet the JESREC's histological criteria (namely, a mucosal eosinophil count ≥70/HPF) were excluded from analysis, which may have resulted in selection bias. We note that discrepancies between preoperative clinical findings and postoperative histological findings are likely due to preoperative steroid administration. 29 However, an accurate assessment of the effects of this type of preoperative therapy would be helpful in understanding the natural history of ECRS.
Conclusions
The percentage of PNAd-expressing vessels is correlated not only with the number of eosinophils infiltrating nasal polyps but also with ECRS severity. Thus, PNAd is responsible at least partially for mobilizing eosinophils to nasal polyps and, consequently, for the severity of ECRS.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924221129903 - Supplemental material for The Percentage of PNAd-Expressing Vessels is Correlated with Disease Severity in Eosinophilic Chronic Rhinosinusitis
Supplemental material, sj-docx-1-ajr-10.1177_19458924221129903 for The Percentage of PNAd-Expressing Vessels is Correlated with Disease Severity in Eosinophilic Chronic Rhinosinusitis by Eiichi Kato, Toshiki Tsutsumiuchi, Akifumi Muramoto, Takahiro Tokunaga, Shigeharu Fujieda and Motohiro Kobayashi in American Journal of Rhinology & Allergy
Supplemental Material
sj-docx-2-ajr-10.1177_19458924221129903 - Supplemental material for The Percentage of PNAd-Expressing Vessels is Correlated with Disease Severity in Eosinophilic Chronic Rhinosinusitis
Supplemental material, sj-docx-2-ajr-10.1177_19458924221129903 for The Percentage of PNAd-Expressing Vessels is Correlated with Disease Severity in Eosinophilic Chronic Rhinosinusitis by Eiichi Kato, Toshiki Tsutsumiuchi, Akifumi Muramoto, Takahiro Tokunaga, Shigeharu Fujieda and Motohiro Kobayashi in American Journal of Rhinology & Allergy
Footnotes
Acknowledgments
We thank Hisataka Kato and Maiko Yamanaka for technical assistance, and Ryan Sullenberger and Elise Lamar for critical reading of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Japan Society for the Promotion of Science (grant numbers 19K18726 and 21H02702).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.