
Abstract
Background
Caudal pneumatization of the pterygoid process may impact endonasal exposure of the lateral recess of sphenoid sinus (LRSS).
Objectives
This study aims to explore the implications of a pneumatized pterygoid process for an endonasal transpterygoid approach to the LRSS and to define strategies regarding the preservation or sacrifice of the vidian nerve.
Methods
Dissection of the LRSS (11 sides) was performed on 6 cadaveric specimens, preselected for the radiographic presence of an LRSS. In addition, the dimensions of the LRSS were measured on the deidentified CT images of 120 patients (240 sides). The sphenoid sinus was subdivided into 3 categories: Type 1 (no identifiable LRSS), Type 2 (lateral pneumatization of the greater wing above the vidian canal), and Type 3 (pneumatization of both the greater wing and the pterygoid process).
Results
On the cadaveric specimens, a Type 2 pneumatization often allowed access to the LRSS above the level of the vidian canal; thus, sparing the vidian neurovascular bundle. In Type 3 pneumatization, a frontal corridor through the pterygoid base could be created to reach the LRSS with preservation of the vidian nerve. Extreme Type 3 pneumatization, however, required the transposition or sacrifice of the vidian nerve to facilitate a full direct access to the superolateral LRSS. Measurements on CT images revealed that the extent of caudal pneumatization of the pterygoid process had no statistically significant correlation with the superolateral extension of the lateral recess in patients with Type 3 LRSS (P > .05).
Conclusion
Pneumatization of the LRSS toward a caudal or superolateral direction may develop independent from each other. Caudal pneumatization of the pterygoid process seems to variably impact the endonasal exposure of the LRSS.
Keywords
Introduction
Significant advancements in surgical techniques and instrumentation have advanced endoscopic endonasal skull base surgeries, leading to the preservation of facial esthetics, decreased length of hospital stay, and improved postoperative quality of life in properly selected patients.1–6 These techniques allow reaching deep-seated structures that previously require extensive open surgery.
As one of the most challenging skull base sites to access, the lateral recess of the sphenoid sinus (LRSS) was traditionally accessed through a craniofacial approach.7,8 However, during the past three decades, various less invasive approaches have been introduced to address lesions arising in the lateral recess of the sphenoid sinus.9–11 Bolger first introduced the transpterygoid approach to the lateral recess of the sphenoid sinus,10,12 and this endonasal approach has been widely adopted with some modifications. However, the feasibility of other techniques has been assessed on cadaveric dissections such as Alves-Belo et al, 13 who demonstrated a lateral orbital approach to access the lateral recess of the sphenoid sinus and Li et al 14 who suggested a prelacrimal approach. In Alves-Belo's study, 13 both the lateral recess and medial aspect of the middle cranial fossa were sufficiently exposed, while the vidian nerve and pterygopalatine ganglion were spared. 13 In a cadaveric study by Li et al, 14 a transnasal prelacrimal approach was adopted to access well-pneumatized lateral recess of the sphenoid sinus demonstrating the feasibility to preserve both the vidian nerve and pterygopalatine ganglion, while providing adequate exposure of the lateral recess of the sphenoid sinus and the middle cranial fossa. 14
As aforementioned, a transpterygoid approach addresses lesions arising from the lateral recess of the sphenoid sinus (eg, cerebral spinal fluid leak, meningocele, meningoencephalocele) and has emerged as one of the most commonly used techniques to access the lateral recess of the sphenoid sinus.15,16 Nonetheless, preservation of the vidian nerve and pterygopalatine ganglion and adequate exposure of highly pneumatized lateral recess of the sphenoid sinus (especially laterally) are still major considerations for an endonasal transpterygoid approach.12,17 Indeed, the current literature reveals variable rates of vidian nerve preservation.12,15,18 Gaining adequate exposure of an extensively pneumatized lateral recess of the sphenoid sinus is considered to be a leading factor triggering the sacrifice of the vidian nerve. 19
Other reports have focused on the extension of the pneumatization of the lateral recess of the sphenoid sinus in the superior and lateral directions; thus, invading the greater wing of sphenoid bone. 20 In patients with a lateral recess of the sphenoid sinus, its pneumatization often extends caudally into the pterygoid process; however, the extent is variable. A quantitative assessment of the caudal pneumatization of the pterygoid process (below the level of the vidian canal) and its implications for an endonasal transpterygoid approach to the lateral recess of the sphenoid sinus have not been sufficiently described.
Therefore, the purpose of this study was to further explore the implications of variable degrees of pneumatized pterygoid process on an endonasal transpterygoid approach to expose the lateral recess of the sphenoid sinus and to define strategies that may help to preserve the vidian nerve.
Materials and Methods
Cadaveric Dissection
Cadaveric specimens were selected after reviewing previously acquired CT scans to ascertain the presence of a lateral recess of the sphenoid sinus. An endonasal transpterygoid approach to access the lateral recess of the sphenoid sinus was performed on six cadaveric specimens (11 sides). All studies were conducted at the Anatomy Laboratory Toward Visuospatial Surgical Innovations in Otolaryngology and Neurosurgery (ALT-VISION) at the Wexner Medical Center of The Ohio State University. Coauthors involved in the dissections had been previously certified by local regulatory agencies dealing with the use of human tissues and cadaveric studies. All specimens had been commercially prepared with intravascular injections of red (arterial) and blue (venous) latex and were preserved in 70% alcohol.
Rod-lens endoscopes with 0°, 45°, and 70° lenses (4-mm diameter, 18-cm length) were coupled to a high-definition camera and monitor (Karl Storz Endoscopy) to provide visualization during the dissections. Still photographs and videos were obtained to define and document the anatomic relationships of the endoscopic dissection. An AIDA system (Karl Storz Endoscopy) was used to record and save images (TIF format) and videos (MPEG format). A high-speed drill (Stryker Co.) with a straight handpiece and 3 to 4 mm hybrid burrs were used for the bony part of the dissections.
Radiologic Analysis
Deidentified CT images of the paranasal sinuses were obtained from 120 consecutive patients (240 sides) with ages ranging from 18 to 60 years, at Beijing Tongren Hospital, Capital Medical University in China, from July 1, 2019, to December 31, 2019. The study protocol was approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University (No. TRECKY2020-18), and proper informed consent for scientific studies was obtained from all patients upon registration for their CT scan. Patients with pansinusitis, sinonasal tumors, skull base trauma, invasive fungal sinusitis, and history of previous sinus surgery were excluded from the study. CT included axial, coronal, and sagittal images obtained in Digital Imaging and Communications in Medicine (DICOM) format. This was imported into Mimics 13.1 (Materialise) for measurements.
Traditionally, pneumatization of the sphenoid sinus had been classified into categories of conchal, pre-sellar, and sellar.
21
To properly assess the lateral recess of the sphenoid sinus and the significance of a pneumatized pterygoid process, however, the sphenoid sinus of 120 patients included in the present study was subdivided into three pneumatization types:
Type 1—Patients with no identifiable lateral recess of the sphenoid sinus (Figure 1A). Type 2—Patients with a superolateral pneumatization toward the greater wing of the sphenoid bone, with pneumatization that does not extend beyond the inferior edge of the vidian canal (Figure 1B). Type 3—Patients with a pneumatization of the greater wing as well as caudal pneumatization of the pterygoid process (Figure 1C).
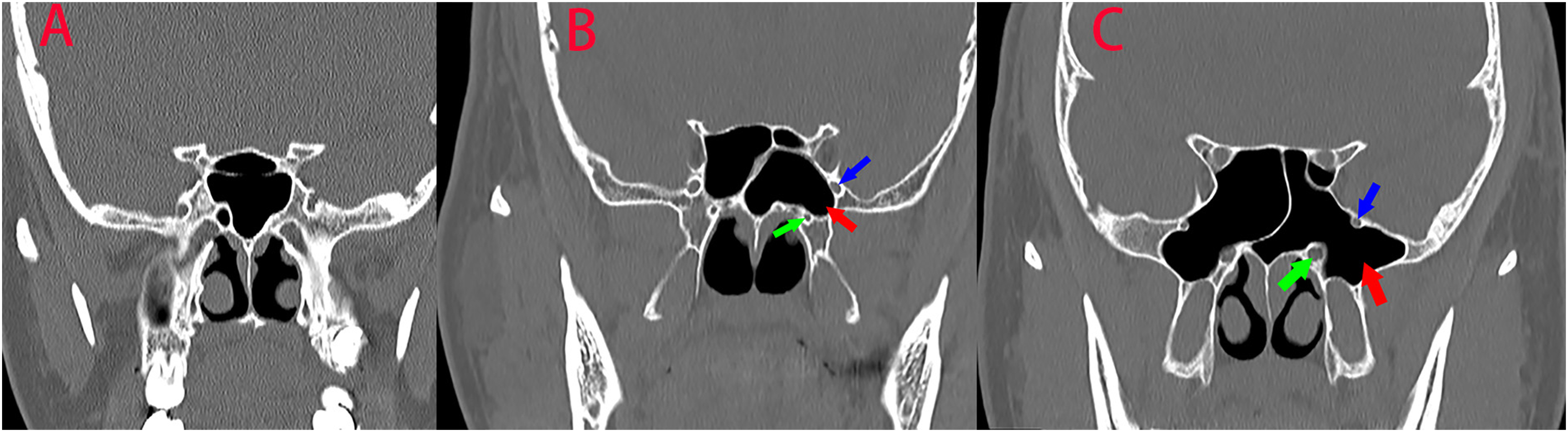
(A) No occurrence of lateral recess of the sphenoid sinus (LRSS); (B) The LRSS (red arrow) mainly extended into the greater wing of sphenoid bone; (C) Pneumatization of both the greater wing and the pterygoid process (red arrow). Green and blue arrows in B and C represent vidian canal and represent maxillary nerve canal, respectively.
Indices measured in a Type 3 variant include height of the vidian (D1) and maxillary nerve canals (D2), lateral extension (D3, horizontal distance from the vidian nerve to the lateral border), and superior extension (D4, vertical distance from the roof of the lateral recess of the sphenoid sinus to the horizontal line crossing the vidian canal) of the lateral recess of the sphenoid sinus (Figure 2). In patients with a Type 2 variant, only the lateral (D3) and superior extensions (D4) of the lateral recess of the sphenoid sinus were measured.
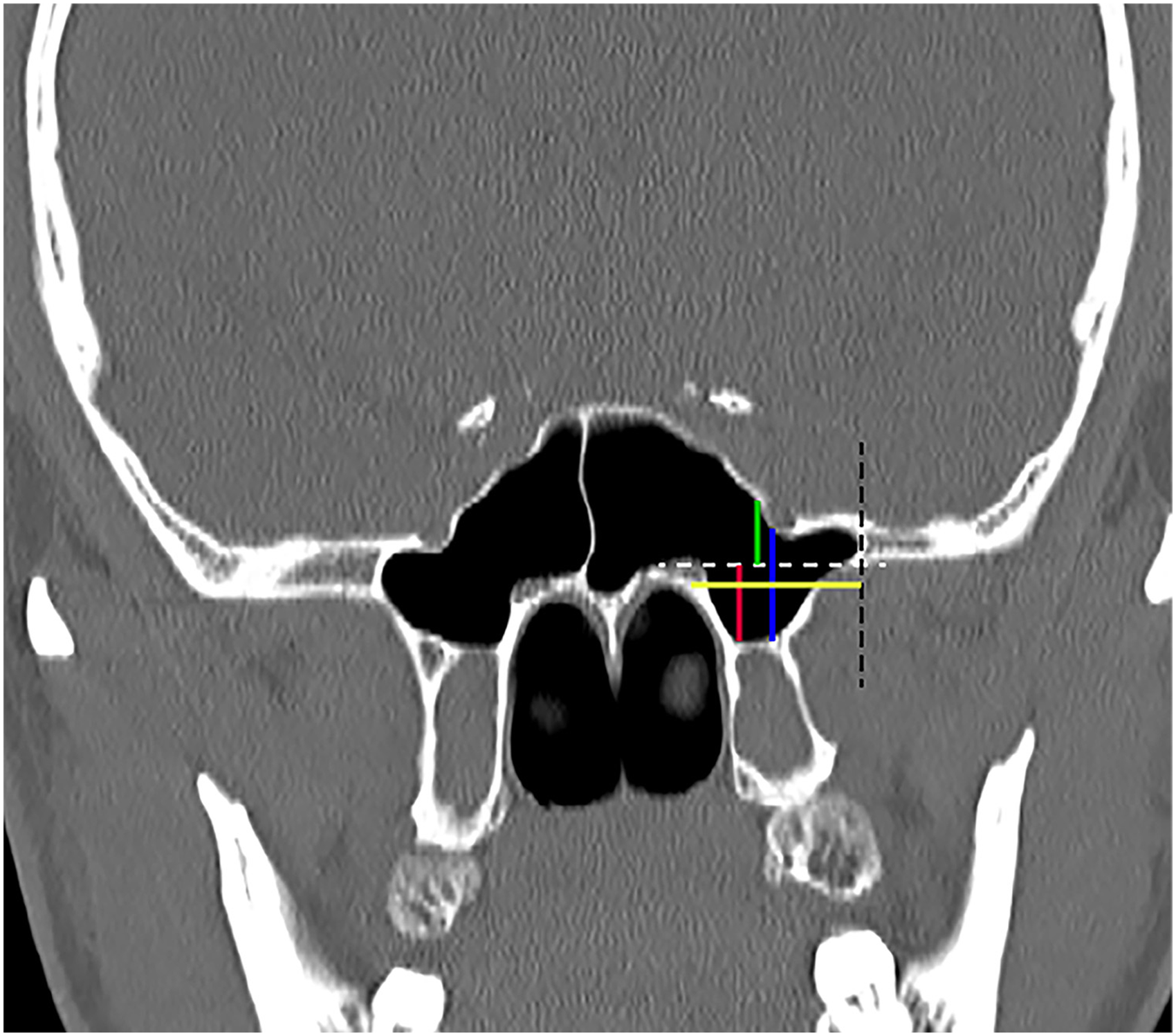
In Type 3 variant, the dot horizontal (white) and vertical lines (black) represent the line crossing the vidian nerve and the lateral borderline of the recess. Schematic description of D1 (red line), D2 (blue line), D3 (yellow line), and D4 (green line) was demonstrated.
Statistical Analysis
In patients with Type 3 variant, the correlation between the caudal extension (D1, D2) with the lateral (D3) and superior extensions (D4) was subject to linear regression analysis. The value was expressed as mean ± standard deviation (SD), and a probability value of P < .05 was considered to be statistically significant. Statistical analysis was performed using Statistica 16.0 (StatSoft, Inc.).
Results
Cadaveric Dissection
As these specimens were preselected, a lateral recess of the sphenoid sinus was present in 11/12 sides (one side did not have a pneumatized lateral recess). Type 2 pneumatization, extending toward the greater wing of sphenoid bone and above the level of vidian canal, was identified in 6/11 sides (54.55%). Caudal pneumatization of the pterygoid process combined with lateral pneumatization into the greater wing of the sphenoid bone (Type 3) was observed in the remaining 5/11 sides (45.45%).
Technical nuances of an endonasal transpterygoid approach have been previously described.22,23 However, the following observations are relevant:
To access a Type 2 lateral recess of the sphenoid sinus above the level of the vidian canal (6/11 sides), the external orifice of the vidian canal and the foramen rotundum was identified along with the pterygoid base (Figure 3A). Access into the lateral recess of the sphenoid sinus was obtained by extending the sphenoidotomy laterally above the vidian canal; thus, preserving of the vidian and palatovaginal neurovascular bundles in all 6 sides (Figure 3B). To get a full direct access to the roof and lateral wall of the lateral recess, however, sacrifice of the lateral nasal wall was required in 2/6 sides (33.33%). When accessing a Type 3 lateral recess (5/11 sides), the soft tissue contents of the pterygopalatine fossa are anterior to the recess; thus, requiring their mobilization laterally and inferiorly to obtain wide and direct access. In turn, this requires transecting the palatovaginal artery and nerve (Figure 4A). The bony wedge inferolateral to the vidian orifice was drilled to enter the lateral recess of the sphenoid sinus (Figure 4B).
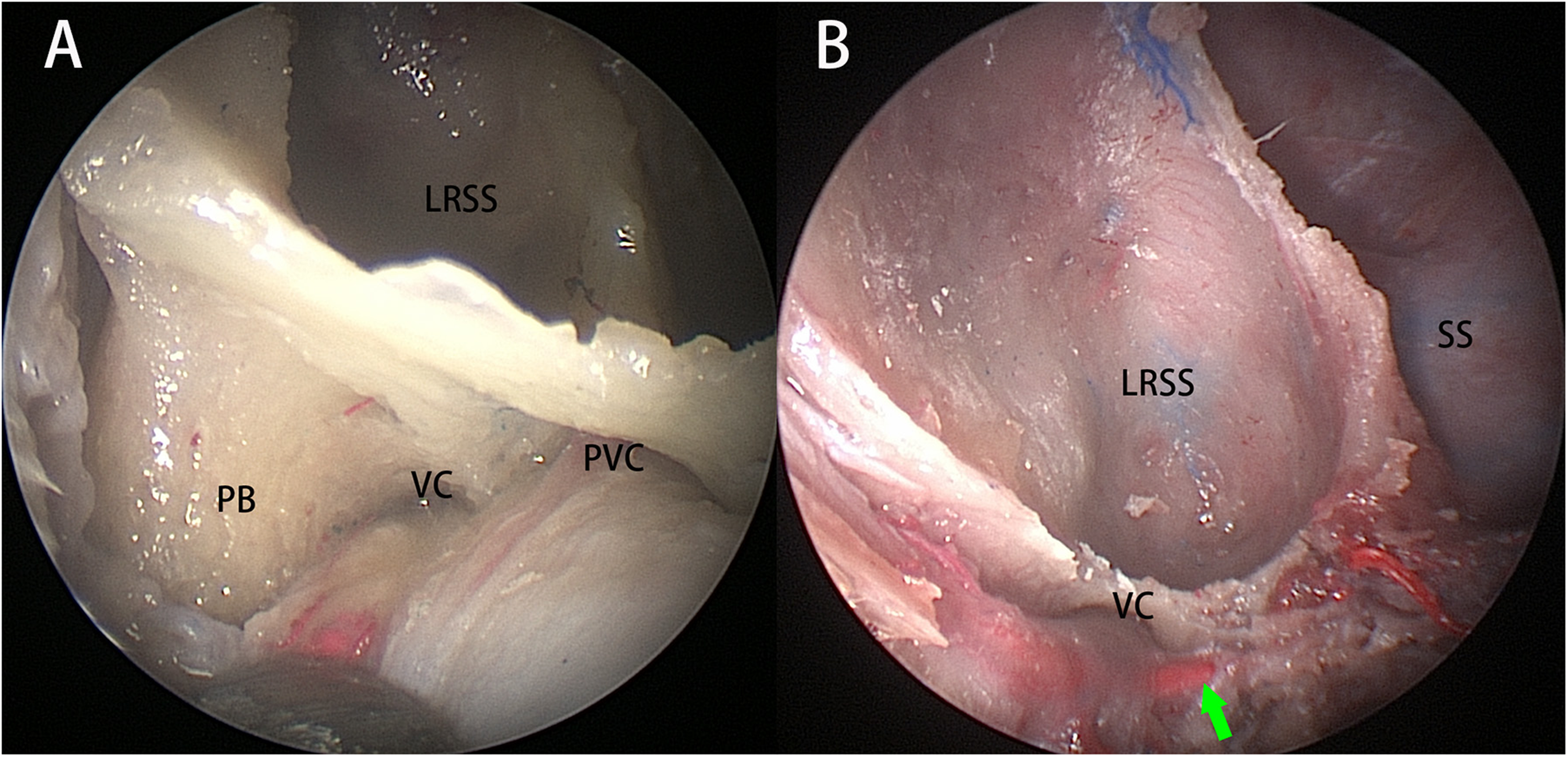
Exposure of Type 2 lateral recess of the sphenoid sinus (LRSS) on right side. (A) The external orifices of the palatovaginal canal (PVC) and vidian canal (VC) were identified along the pterygoid base (PB); (B) The entire lateral recess was exposed above the level of VC after removal of the anterior wall of the LRSS, blue arrow: palatovaginal artery.

Exposure of a Type 3 LRSS on left side. (A) The palatovaginal artery and nerve (green arrow) were transected to facilitate the exposure of the pterygoid base (PB) and vidian canal (VC); (B) The bony wedge inferolateral to the vidian nerve at the PB was drilled allowing entry into the lateral recess of the sphenoid sinus (LRSS); (C) The posterolateral wall (PLW) and bottom wall (BW) of the lateral recess were directly exposed; (D) The superior wall (SW) and lateral wall (LW) were sufficiently exposed under angled view.
Both the floor and posterior wall of the lateral recess of the sphenoid sinus could be adequately exposed in all five Type 3 sides (Figure 4C). Angled-lens scopes (45° or 70°) can help to approach and visualize its roof (middle cranial fossa) and lateral wall even in the 2/5 sides that were pneumatized into the greater wing of the sphenoid (Figure 4D). In these two sides, ease of instrumentation with full and direct access to the roof and lateral wall of the lateral recess required the resection of the lateral nasal wall, and the circumferential drilling of the vidian canal to allow the transposition or sacrifice of the nerve.
Radiological Analysis
Based on the classification of sphenoid sinus pneumatization proposed in the present study, the absence of a lateral recess of the sphenoid sinus (Type 1) was observed (CT scan images) in 111 sides (46.25%). In the remaining 129 sides with a lateral recess of the sphenoid sinus, Type 2 and 3 variants accounted for 51 sides (21.25%) and 78 sides (32.5%), respectively.
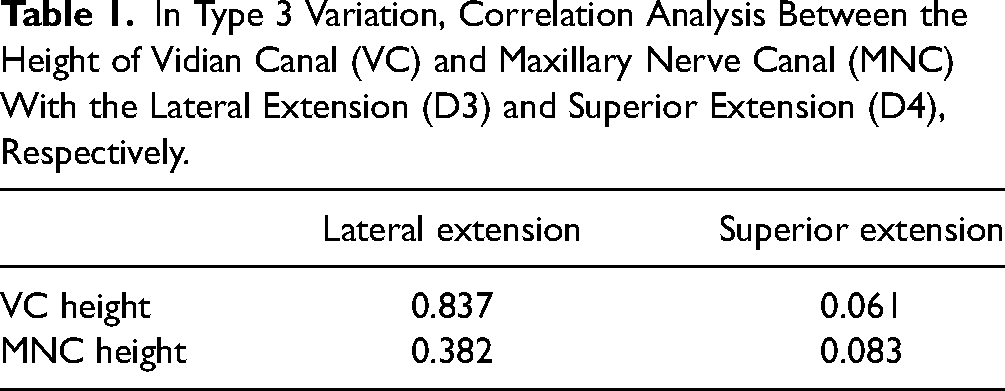
In patients with Type 3 lateral recess, the average height of the vidian canal (D1) and maxillary nerve canal (D2) was 0.81 ± 0.22 cm and 1.30 ± 0.30 cm, respectively (Table 1). There was no significant correlation between caudal pneumatization of the pterygoid process (D1, D2) and the lateral and superior extension (D3, D4; all P > .05, Table 1).
In Type 3 Variation, Correlation Analysis Between the Height of Vidian Canal (VC) and Maxillary Nerve Canal (MNC) With the Lateral Extension (D3) and Superior Extension (D4), Respectively.
Discussion
The emergence of an endonasal transpterygoid approach has reduced or even eliminated many barriers to surgically manage lesions at the lateral recess of the sphenoid sinus.10,23 Some have suggested that the vidian nerve and the pterygopalatine ganglion may be preserved in the majority of cases. 12 However, lateral extension of the pneumatization, into the greater wing of the sphenoid bone seems to be a significant restricting factor for direct exposure and instrument access to the posterolateral wall of the lateral recess. 24 This study suggests that when there is no caudal pneumatization of the pterygoid process (Type 2), the corridor accessing the lateral recess may be established above the level of vidian canal; therefore, preserving the vidian neurovascular bundle. However, it also indicates that the lateral nasal wall is a significant obstacle to expose of the most lateral aspect of lateral recess of the sphenoid sinus that extends into the sphenoid wing. Therefore, its partial or total removal may be warranted to achieve a full direct access. Alternatively, a transnasal prelacrimal or a translateral orbital approach may be used to provide adequate exposure while allowing the preservation of the lateral nasal wall.13,14
Bolger advocated using a direct corridor through the pterygoid base, inferolateral to the vidian canal, for patients with pterygoid process pneumatization extending below the level of the vidian canal (Type 3 variant). 12 However, others have indicated the occasional unavoidable need to transect the palatovaginal neurovascular bundle to facilitate the lateral displacement of contents of the pterygopalatine fossa and reported that the sacrifice had no discernible clinical consequence. 25 This study seems to confirm that the geometry and dimensions of the surgical window through the pterygoid base may present additional challenges, restricting the concomitant insertion and maneuverability of an endoscope and one or two surgical instruments 14 ; therefore, expanding the pterygoid window is indicated according to the need for a superolateral exposure. Similarly, the study findings agree with other previous studies suggesting that in patients with a narrow pterygoid window or an extremely superolateral extension of the lateral recess, a transposition or sacrifice of the vidian neurovascular bundle is required to facilitate further exposure.17,26
Correlation between caudal pneumatization of the pterygoid process and superolateral pneumatization into the greater wing of the sphenoid bone in patients with Type 3 pneumatization reveals that the extent of caudal pneumatization had no statistically significant correlation with the extent of lateral and superior pneumatization of the lateral recess (Table 1). This implies that pneumatization of the sphenoid bone toward a caudal and a superolateral direction may develop independently with each other; therefore, the role of caudal pneumatization into the pterygoid process on endonasal surgical exposure of the lateral recess of the sphenoid sinus can vary depending on the actual pneumatization status.
Based on this cadaveric dissection and our previous experience, pneumatization of the pterygoid process may impact the required endonasal access to the lateral recess of the sphenoid sinus by:
In patients with a Type 2 pneumatization, a superior and lateral extension of the lateral recess above the vidian canal is encountered. In this setting, the lateral nasal wall becomes the most significant obstacle; thus, requiring an extended maxillectomy to enhance the lateral exposure. In Type 3 patients with an extensive caudal pneumatization of the pterygoid process but limited superolateral extension toward the greater wing of the sphenoid bone, the established corridor inferolateral to the vidian canal on the pterygoid base can provide adequate exposure of all aspects of the lateral recess. Preservation of the vidian nerve and lateral nasal wall is likely possible. Type 3 expansive pneumatization in the greater wing of the sphenoid bone accompanying the caudal pneumatization of the pterygoid process presents a surgical challenge to provide a direct full access to the superolateral wall of the lateral recess of the sphenoid sinus through an endonasal corridor. Although angled scopes and instruments can facilitate exposure, complex lesions arising from the roof or lateral wall of the lateral recess often require a full direct access and free instrument maneuverability.17,27 Therefore, sacrifice of the vidian nerve or circumferential drilling of the vidian canal to allow its transposition and the partial or complete removal of the lateral nasal wall may be required.
28
This study comprises significant limitations, as it is a preclinical cadaveric and radiological study, and the application of the described principles requires clinical validation. Nonetheless, the suggestions regarding the preservation or sacrifice of the vidian nerve and lateral nasal wall are based on anatomical findings. In 2/5 sides of specimens (40%) with a Type 3 variant, the transposition or sacrifice of the vidian nerve was required to provide adequate exposure and facilitate a full direct access with currently available instrumentation. In the clinical setting, however, the exposure of the roof and superolateral aspect may be impacted by additional factors, including the location and pathological character of the lesion, the strategy for management of the lesions, the availability of instrumentation, as well as surgical experience and expertise. Therefore, defining a critical measurement (ie, D3, D4) that could help decide when the sacrifice of the vidian nerve or lateral nasal wall still needs to be defined by clinical study.
Conclusion
Pneumatization of the lateral recess of the sphenoid sinus toward a caudal or superolateral direction may develop independently from each other. Impact of a caudal pneumatization of the pterygoid process on endonasal exposure of the lateral recess of the sphenoid sinus seems to be variable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N. London holds stock in Navigen Pharmaceuticals, was a consultant for Cooltech Inc., and receives research funding from Merck, Inc., none of which are relevant to this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Lifeng Li received funding support from the National Key R&D Program of China (2019YFC0119301) during his stay at the Ohio State University.