
Abstract
Background
Adult and elderly patients with chronic rhinosinusitis (CRS) undergo similar therapeutic management. Few studies have undertaken sinonasal tissue-level comparisons of these groups. This study examines histopathological differences between adults (>18, <65 years) and the elderly (≥65 years) with CRS, with the goal of optimizing medical management.
Methods
In a retrospective cohort analysis, demographic factors, comorbidities, and a structured histopathological report of 13 variables were compared across adult and elderly patients with CRS who underwent functional endoscopic sinus surgery. These cohorts of adult and elderly patients included patients with and without nasal polyps (NP).
Results
Three hundred adult (158 aCRSsNP, 142 aCRSwNP) and 77 elderly (38 eCRSsNP, 39 eCRSwNP) patients were analyzed. Mean age of the adult cohort was 44.4 ± 12.4 years, while that of the elderly cohort was 71.9 ± 5.9 years (P < .001). Significantly more adults compared to elderly individuals demonstrated a positive atopic status (79.7% vs 64.0%, P = .004). Elderly patients exhibited higher rates of comorbid diabetes mellitus than adult patients (21.6% vs 10.3%, P = .009). Adults exhibited more tissue eosinophilia (43.4% vs 28.6%, P = .012) and presence of eosinophil aggregates (25.0% vs 14.3%, P = .029) compared to elderly patients, regardless of NP status. Conversely, the elderly demonstrated significantly more fungal elements (11.7% vs 3.0%, P = .004), and trended toward increased overall inflammation (63.6% vs 55.3%, P = .118) and tissue neutrophilia (35.1% vs 27.3%, P = .117), compared to adults.
Conclusion
Sinonasal tissue of adult and elderly patients with CRS demonstrates clear histopathological differences. Patient comorbidities, in addition to histopathological characterizations, may provide further context for management optimization.
Level of Evidence
2.
Short Summary
Sinonasal tissue samples from adult and elderly patients with CRS demonstrate clear histopathological differences. These patient populations also exhibit unique comorbidities. These distinctions have the potential to inform and optimize management of this condition.
Keywords
Introduction
While, chronic rhinosinusitis (CRS) is a common condition, impacting 5% to 12% of the population, 1 several studies have demonstrated that the elderly have a significantly higher incidence of CRS relative to adult patients, with 1 Korean group showing the prevalence of CRS in patients 60 years or older as almost twice that of younger patients. 2 Studies have demonstrated that older adults have increased CRS-associated comorbidities, including diabetes and reflux, as well as higher healthcare expenditure costs.3,4 Older individuals are also less likely to undergo surgery, and therefore are required to tolerate longer periods with higher CRS symptom burden. 3 Litvack et al 5 showed that age is significantly associated with increased risk for both hyposmia and anosmia. Furthermore, elderly individuals with CRS who opt for surgical intervention, report smaller improvements in disease-specific and general health quality of life outcomes following surgery. 6 Ageing has been shown to impact the paranasal sinuses specifically through declining ciliary motility, atrophy of supporting tissue in the nose, and increased nasal volume with decreased elasticity of the nasal mucosa.7,8 Current projections estimate that individuals aged 65 years or older will represent 20% of the US population by 2050. 9 Given this population shift, it is especially helpful to understand the effects of ageing on chronic diseases, specifically, the histopathological features of CRS in the elderly.
There is a paucity of literature on the histopathological features of CRS in the elderly population.10,11 One group of researchers suggested that relative to their younger counterparts, elderly patients with CRS demonstrate an endotype that features a more pro-inflammatory, neutrophilic immune response, with elevated mucus levels of interleukin1 β (IL-1β), IL-6, IL-8, and tumor necrosis factor α (TNF-α), irrespective of polyp status. 12 These increases in pro-inflammatory cytokines were associated with symptomatic bacterial infection and colonization in aged patients. Cho et al 13 found that levels of eosinophil cationic protein, an important marker of eosinophilic inflammation in CRS, in nonelderly patients were significantly higher compared with those in elderly patients, suggesting that eosinophilic inflammation appears to wane with age. The purpose of the current study is to identify characteristics distinct to aged patients with CRS, with the potential to change treatment approaches for this at-risk population.
Methods
Appropriate Institutional Review Board approval from Rush University Medical Center was obtained for this study.
Patients were eligible for the study if they had medically recalcitrant CRS, defined as 12 weeks of continuous sinonasal symptoms and positive findings on computed tomography and/or endoscopy based on clinical guidelines.1,14,15 Sinusitis cases associated with sinonasal malignancy, autoimmune disease, cystic fibrosis, or immunoglobin/immunological deficiencies were excluded. Furthermore, any patients subsequently found to have any of these conditions were excluded from the present analysis.
A retrospective chart review was performed to collect patient demographics, comorbid conditions, including asthma, gastroesophageal reflux disease (GERD), diabetes mellitus (DM), atopic status (ie, positive or negative percutaneous testing), and structured histopathology reports. Study population included adult (≥18 years) and elderly (≥65 years) patients with CRS without nasal polyps (CRSsNP) and CRS with nasal polyps (CRSwNP) who underwent functional endoscopic sinus surgery (FESS) at a tertiary care center between June 2014 and June 2020, was performed. FESS was defined as bilateral maxillary antrostomy, complete spheno-ethmoidectomy, and frontal sinusotomy. Diagnosis of asthma was obtained from manual review of the medical records of patients with CRS for diagnostic confirmation by a fellowship-trained pulmonologist based on clinical guidelines. 16 In accordance with the most recent clinical guidelines, diagnosis of atopy was based on positive evidence of sensitization to aeroallergens, including tree, grass, ragweed, mold, dustmite, animal (cat/dog), and cockroach, by skin prick test, and confirmed by a fellowship-trained allergist-immunologist. 17 A positive prick test indicated that the patient had IgE antibody specific for the allergen being tested on the skin's mast cells.
A structured histopathology report consisting of 13 variables (Table 1) was assessed in order to analyze differences in sinus tissue between groups. Each report was completed by 1 of the 2 dedicated head and neck pathologists. Histopathological variables assessed included: degree of inflammation (none/mild or moderate/severe), number of eosinophils per high power field (HPF) (<5/HPF or 5+/HPF), neutrophil infiltrate (absent or present), inflammatory predominance (lymphocytic, lymphoplasmacytic, eosinophilic, neutrophilic, or mixed), basement membrane thickening (absent or present), subepithelial edema (absent or present [focal, perivascular, or distortion of mucosal structure]), hyperplastic/papillary changes (absent or present), mucosal ulceration (absent or present), squamous metaplasia (absent or present), fibrosis (absent or present), Charcot-Leyden crystals (absent or present), and eosinophil aggregates (absent or present). The features used for reporting subepithelial edema included the presence of loose stroma in the subepithelium with or without microcysts and inflammatory cells. Tissue eosinophilic aggregates were defined as groups of >20 eosinophils/HPF within the lamina propria of the sinonasal mucosa.
Structured Histopathology Report.
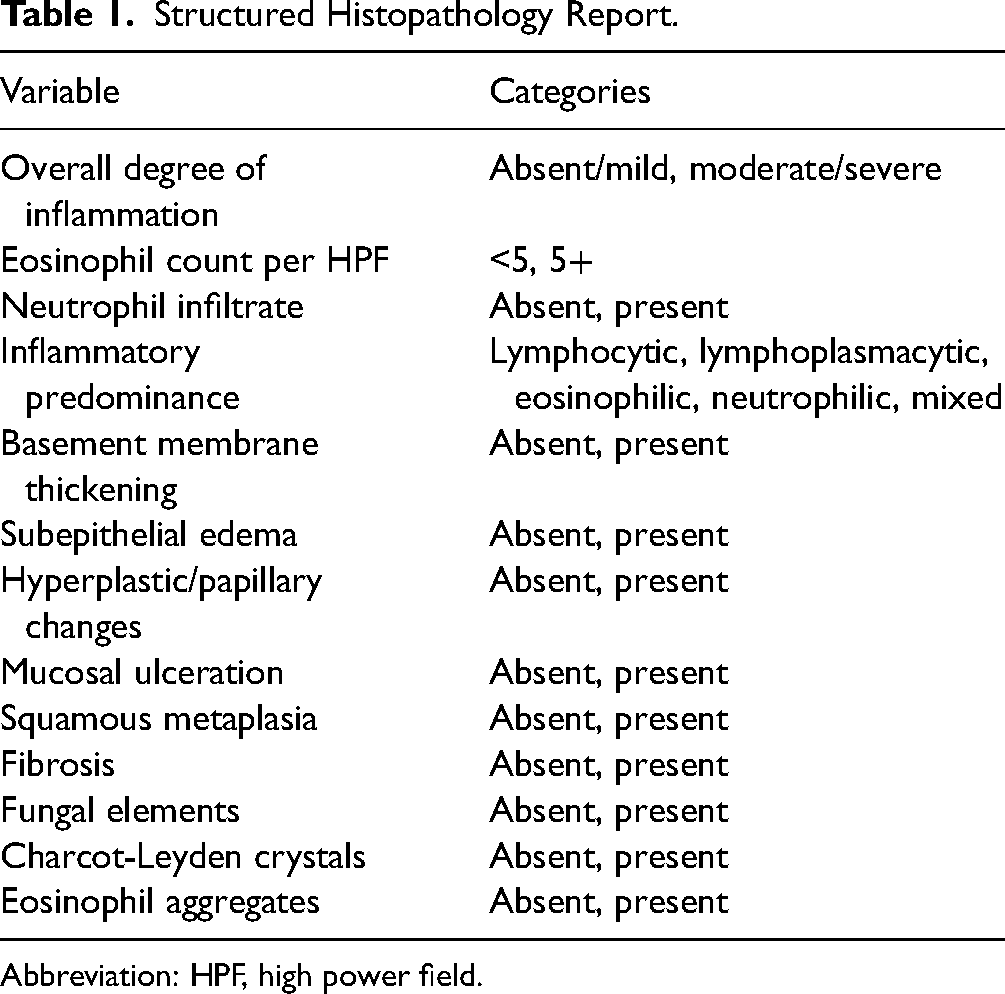
Abbreviation: HPF, high power field.
A 2-tailed Student t-test was used for comparison of parametric data. A one-way analysis of variance test was used to compare means between more than 2 independent groups. Nonparametric qualitative variables were compared using a χ2 test. All statistical analyses were performed using SPSS version 27.0 (IBM, Armonk, NY). A P-value ≤ .05 was considered significant for all statistical analyses.
Results
Seventy-seven elderly (38 CRSsNP and 39 CRSwNP) and 300 adult (158 CRSsNP and 142 CRSwNP) patients were analyzed. The mean age of the elderly CRS cohort was 71.9 years with a standard deviation of 5.9 years (age range: 65.3-89.1 years), while the mean age of the adult CRS cohort was 44.4 years with a standard deviation of 12.4 years (age range: 19.1-64.3 years). Of the elderly population, 36 were male and 41 were female. Of the adult population, 134 were male and 163 were female. Among the elderly cohort, 21.9% had DM, 35.1% had asthma, 64.0% had a positive atopic status (ie, tested positive on percutaneous allergy testing), and 33.8% had GERD, 50.6% had nasal polyps (NPs), and 18.2% had a history of revision sinus surgery. Of the adult cohort, 10.3% had DM, 37.7% had asthma, 79.7% had a positive atopic status, 26.5% had GERD, 52.1% had NPs, and 15.0% had a history of revision of sinus surgery. Significantly more elderly compared to nonelderly individuals had a comorbid DM diagnosis (21.9% vs 10.3%, P = .009). Significantly more nonelderly compared to elderly individuals had a positive atopic status (79.7% vs 64.0%, P = .004). Complete patient demographic data can be found in Table 2.
Demographics of Adult and Elderly Patients With CRS.
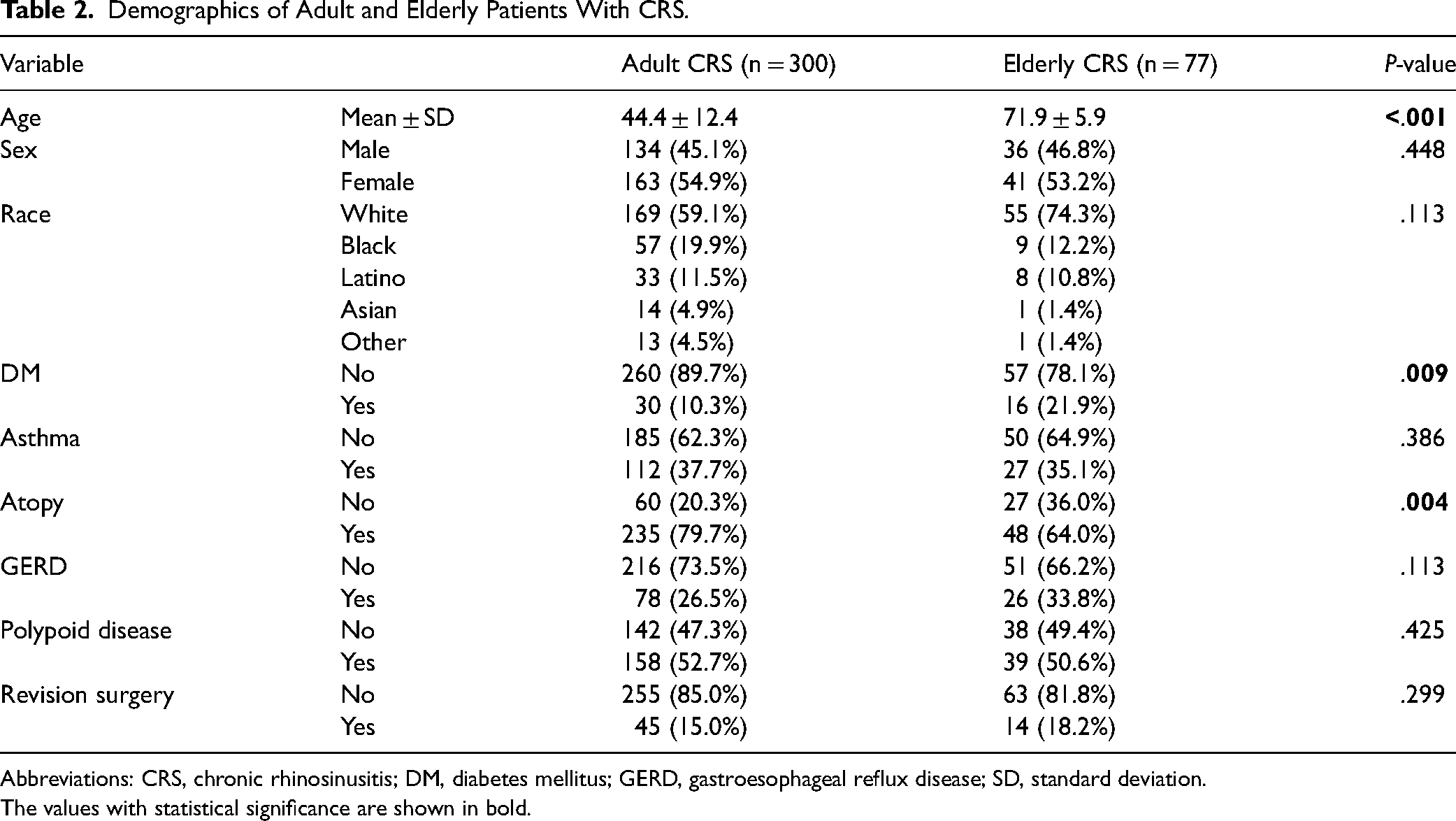
Abbreviations: CRS, chronic rhinosinusitis; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; SD, standard deviation.
The values with statistical significance are shown in bold.
Regarding histopathological characterization, adults with CRS exhibited significantly more tissue eosinophilia (28.9% vs 12.0%, P = .006) and eosinophil aggregates (70.3% vs 44.0%, P < .001). Elderly individuals exhibited increased fungal elements (11.7% vs 3.0%, P = .004) and trended toward increased tissue neutrophilia (35.1% vs 27.3%, P = .117) and overall inflammation (63.6% vs 55.3%, P = .118), relative to nonelderly patients. Complete structured histopathological data can be found in Table 3.
Comparison of Structured Histopathological Variables Between Adult and Elderly Patients With CRS.
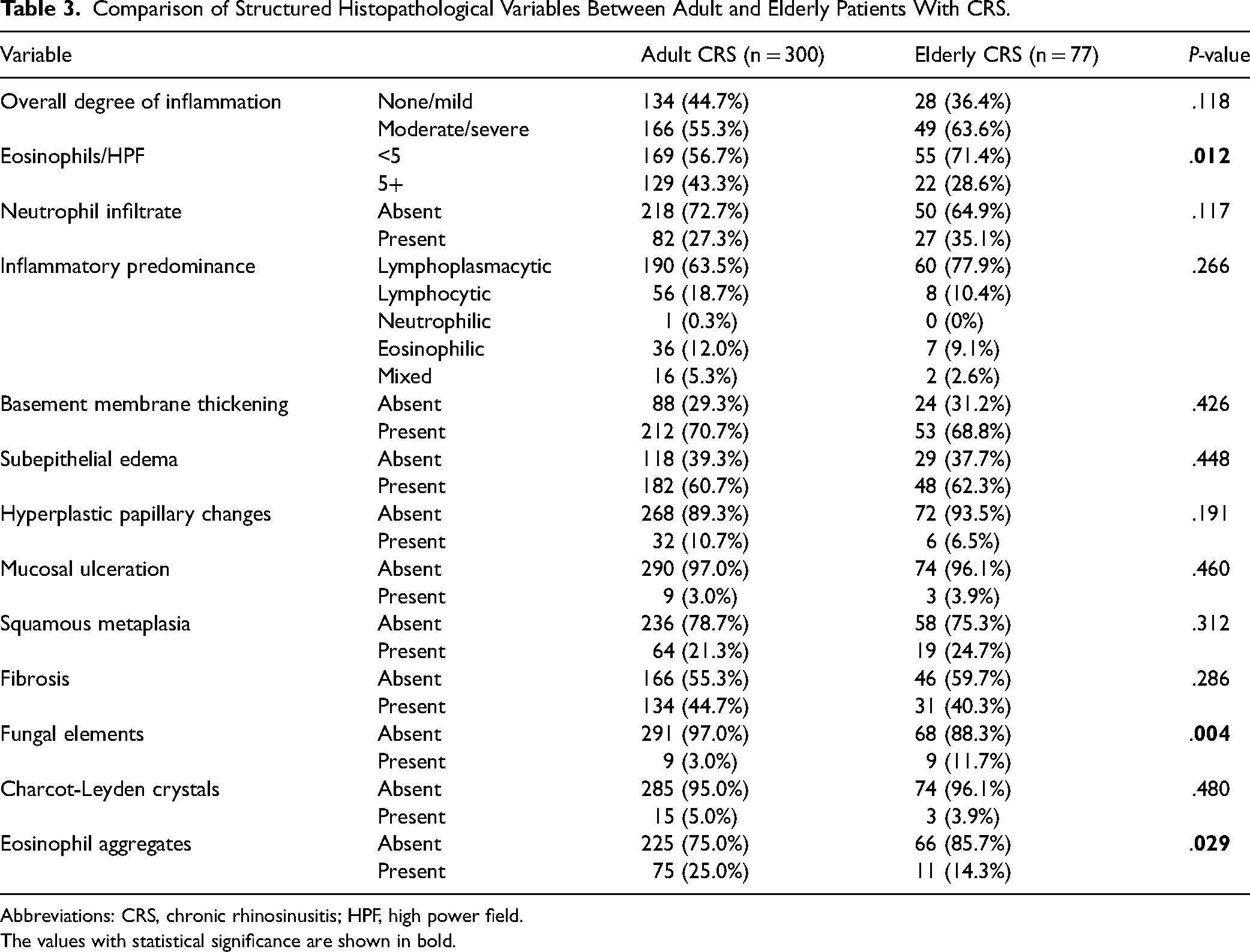
Abbreviations: CRS, chronic rhinosinusitis; HPF, high power field.
The values with statistical significance are shown in bold.
Discussion
The role of ageing in CRS remains largely undefined despite the increasing elderly population and associated healthcare resource utilization. Our findings suggest that elderly and adult patients with CRS have unique histopathological profiles. This claim is consistent with that which is already known about immunity and ageing, in particular, the idea that as we age, the makeup of our innate immune system changes.18,19 Immunosenescence, or the gradual deterioration of immune function with age, has been shown to affect the pathophysiology of airway inflammatory diseases, including CRS. 20 The decline of numerous immune cell functions with ageing is well documented.
Age-based changes in eosinophil quantity and quality have previously been noted. 21 Mathur et al examined the counts and behavior of eosinophils extracted from the peripheral blood of adult and elderly patients with asthma. They reported an age-related change in eosinophil functional activity, specifically a decrease in IL-5-stimulated eosinophil derived neurotoxin degranulation. 21 Interestingly, though Cho et al 13 did not show a difference in number of infiltrating tissue eosinophils in patients with CRSwNP aged 60 years and older relative to nonelderly patients, they did find that eosinophilic cationic protein, a marker of eosinophilic inflammation, extracted from nasal lavages, was significantly reduced in older versus younger patients. These findings imply that though eosinophils infiltrate NP tissue in elderly patients, they are less functional. Our data advance this body of literature by suggesting that elderly patients with CRS, across both CRSsNP and CRSwNP subgroups, exhibit decreased tissue eosinophilia.
The question remains whether elderly individuals with CRS exhibit an inefficient Th2 response or favor a Th1 response. Ageing has been associated with reductions in sinonasal ciliary beat frequency and mucociliary clearance, 20 which in turn may result in reduced phagocytosis and pathogenic bacteria and impaired innate defense mechanisms. 22 Morse et al 12 suggest that elderly individuals with CRS favor a Th1 response by showing that aged patients with CRS have elevated levels of select pro-inflammatory cytokines, including IL-1β, IL-6, IL-8, and TNF-α. This analysis also correlated the levels of these pro-inflammatory cytokines with increased bacterial colonization and/or infection. In sum, these data support a neutrophil-driven mechanism of chronic inflammation in aged patients with CRS, irrespective of polyp status, which may be associated with an inability to clear pathogenic bacteria from the sinonasal cavity.
It has been posited that the waning eosinophilic inflammation seen in elderly patients with CRS correlates with a reduction in the expression of S100A8/9, 13 which are epithelial barrier-associated proteins with antimicrobial activity. 23 Accordingly, our data show that elderly patients with CRS not only display significantly lower levels of tissue eosinophilia, but also that they show increased overall inflammation and tissue neutrophilia relative to their younger counterparts, though these differences did not reach statistical significance.
It is possible that epithelial barrier breakdown associated with loss of eosinophils creates an environment within which tissue neutrophils can infiltrate and become a key inflammatory cell. Interestingly, this is born out in our date set. Interesting, elderly and nonelderly patients with CRSsNP demonstrated a more prominent difference in tissue neutrophilia, relative to their CRSwNP counterparts. Among patients with lower levels of tissue eosinophilia (ie, patients with CRSsNP), tissue neutrophils may more easily be able to infiltrate the tissue. Accordingly, based on the data presented, we posit that an inefficient Th2 response and a favored Th1 response are not mutually exclusive and that these disease processes may in fact be occurring in concert within the elderly patients with CRS.
In addition to histopathological characterization of elderly CRS, clinical identifiers of elderly CRS may prove beneficial for providers. Of all patients with CRS in this cohort, nonelderly patients were significantly more likely to demonstrate positive atopic status. Hwang et al 2 have previously showed that the association between CRS and allergic rhinitis, though it exists, is significantly weaker in elderly compared to nonelderly patients with CRS. Unlike adult patients with CRS, where atopic status is commonly interrogated, this approach may not exhibit the same diagnostic or therapeutic efficacy in elderly patients with CRS.
On the other hand, co-diagnosis of DM is significantly more common in elderly relative to adult patients with CRS. Unsurprisingly, elderly patients with CRS demonstrated significantly more fungal elements on structured histopathology than younger patients with CRS. These data are consistent with the known and close association between DM and presence of fungal elements on sinonasal structured histopathology.
There are several limitations of the present study. First, as a retrospective cohort analysis, there is potential for selection bias. Second, the study is limited by the lack of normal adult and elderly control groups. Importantly, though histopathological characterization of elderly and adult CRS has the potential to be massively useful in terms of optimizing treatment, we would be remiss not to address the utility of endotyping in both adult and elderly patients with CRS to better understand the inflammatory profile of CRS. Endotypic and histopathological characterizations complement one another in the pursuit of maximizing therapeutic options for patients.
Conclusion
This study is the largest of its kind to explore the histopathological differences between elderly and adult CRS. There are marked differences in the inflammatory response of both groups, perhaps suggesting different pathophysiological pathways of disease in these populations. Elderly patients with CRS, regardless of NP status, demonstrate decreased tissue eosinophilia and presence of eosinophil aggregates as well as a trend toward increased tissue neutrophilia and overall inflammation, relative to nonelderly patients with CRS. Patients with this age-dependent, pro-inflammatory immune profile may be less likely to respond to glucocorticoids and may ultimately benefit from alternative treatment approaches. The elderly CRS population not only appears to have distinct pathophysiology, but also unique clinical presentations from adults with CRS. Specifically, elderly patients are significantly less likely to have a comorbid positive atopic status and significantly more likely to have a co-diagnosis of DM. These clinical feature findings may also have implications for disease management, for example, patients with DM may suffer adverse events and have a relative or absolute contraindication to systemic steroid use.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study protocol was approved by the Institutional Review Board at Rush University Medical Center.