
Abstract
Background
The success rate of chronic rhinitis surgery varies depending on the patients’ factor and surgical method. While outcomes for nasal obstruction differ, the association between preoperative severity of other rhinitis symptoms, such as rhinorrhea, sneezing, and nasal itching, measured via the reflective total nasal symptom score (rTNSS) remains unevaluated.
Objective
To evaluate the association between the response rate to surgical treatment of chronic rhinitis and preoperative severity.
Methods
A retrospective cohort study was conducted among adult patients with chronic rhinitis symptoms refractory to medication and nasal spray for over 6 months and received radiofrequency ablation of inferior turbinates with posterior nasal nerve neurolysis. The primary endpoint was the change from baseline in 24-h rTNSS and nasal obstruction symptom evaluation (NOSE) scores. Postoperative surgery response rate, rTNSS score change, and score improvement ratios were also evaluated.
Results
A total of 183 patients (110 males, 60.1%) were included in this study. After 3-month follow-up, the preoperative rTNSS was 6.51 ± 2.74 change to 1.70 ± 1.43, and the NOSE score was 56.48 ± 19.90 change to 4.56 ± 7.74. Both scores and all sub-scores showed significant differences when comparing preoperative, 1-month, and 3-month results (P < 0.05-0.001). The response rate by rTNSS for whole cohort was 78.14 ± 41.44% and 93.99 ± 23.83% at 1- and 3-month follow-up. Subgroup analyses were performed according to individual rTNSS scores and 2 in 1 score groups (ie, 1-2, 3-4, etc) and their relationship to the surgery outcomes. Both preoperative individual score and score groups were significantly associated with all post-operation outcomes (P = 0.022 to <0.001) in linear regression analysis.
Conclusion
Patients with more severe preoperative rhinitis symptoms are associated with better response rate, post-operation symptom score changes, and score improvement ratio.
Introduction
Chronic rhinitis encompasses a range of symptoms caused by nasal mucosal inflammation, including nasal congestion, rhinorrhea, nasal itching, and sneezing. For treatment-resistant chronic rhinitis, various surgical approaches have been proposed, including inferior turbinate reduction (eg, partial and submucosal turbinectomy),1,2 radiofrequency (RF) ablation of the inferior turbinate (RFIT),3,4 vidian nerve resection, 5 and posterior nasal nerve resection or ablation.6–11 However, the surgery success rate varies with the different disease entities and surgical methods. Carrie et al 12 reported greater improvement in SNOT-22 scores was predicted by higher baseline symptom severity scores in septoplasty patient's cohort. Pedersen et al 13 reported that 81% of patients with severe nasal obstruction and 31% of those with mild nasal obstruction before surgery improved postoperatively. Only 56% of patients who received septoplasty reported that the results of the surgery were as they had expected. While the results of nasal obstruction vary, the associations of the preoperative severity of other rhinitis symptoms like rhinorrhea, sneezing, and nasal itching using rTNSS have not yet been evaluated.
In 2023, the American Academy of Otolaryngology endorsed posterior nasal nerve neurolysis (PNNN) as the standard treatment for treatment-resistant chronic rhinitis, including allergic and non-allergic forms of the condition. 14 PNNN can be performed with cryotherapy, RF ablation, and laser ablation. 15 Recently, a meta-analysis on various PNNN techniques reported improvements in the minimal clinically important difference in total nasal symptom scores (1.0 point) after 3 months of cryotherapy and RF therapy were 81.8% and 92.7%. 7 Although PNNN produced significant improvement with a lower complication rate and promising treatment effects, the response is not immediate (rTNSS improvement ≥ 30%) with the response rate at 3 months standing at 77.11% and varying up to 12 months of follow-up.6,9,11,16,17 To improve the early response rate, we combined PNNN with RFIT to obtain the joint result of the treatment of chronic rhinitis along with nasal obstruction relief immediately after the procedure.
To predict the outcome of chronic rhinitis surgery, a thorough preoperative evaluation to ascertain the diagnosis and perform the most suitable procedure is essential. By carefully selecting suitable cases, surgery success rates could be high; however, to the best of our knowledge, no study discussing the correlation between preoperative rhinorrhea, nasal itching, and sneezing has been conducted yet. Therefore, we hypothesized that the preoperative symptom score of rTNSS for chronic rhinitis was linearly correlated with the postoperative symptom score change and surgery outcome for patients who underwent chronic rhinitis surgery.
Methods
Study Design and Patient Population
This retrospective cohort study evaluated patients seeking treatment for chronic rhinitis between February and December of 2023. The study was approved by the Ethics Committee of the Chiayi Christian Hospital (No. CYCH2024022; April 12, 2024). Our inclusion criteria were as follows: age 18 to 65 years and chronic rhinitis symptoms refractory to previous nasal spray and/or oral antihistamine medical treatment for >6 months with poor response to adequate medical treatment, defined as new prescribed continuous use of steroid nasal spray with oral antihistamine, for 3 months. Our exclusion criteria were as follows: acute or chronic rhinosinusitis and the presence of anatomic obstructions that limit access to the posterior nasal passage. Data on patients’ age, sex, cigarette habits, obstructive sleep apnea history, patient combining other procedures (septoplasty), preoperative and each follow-up visit rTNSS, and NOSE scores, were collected. The use of medications such as steroid nasal sprays and antihistamines and the patient's habitual performance of nasal irrigation were not restricted before surgery. No nasal spray or oral antihistamine was prescribed during follow-up visits unless the patient suffers from moderate-to-severe rhinorrhea or congestion despite complete nasal surgical wound resolution.
Procedure
The procedures were performed by a single otolaryngology surgeon (CYH) under local anesthesia in the operation room or under general anesthesia if combined with septoplasty based on the patient's preference. All surgical procedures included turbinate reduction with RFIT and PNNN for chronic rhinitis symptom control. Septoplasty is not routinely performed and will only be combined with RFIT and PNNN when the deviated septum causes difficulty approaching the posterior nasal meatus to perform PNNN.
RFIT was performed using CelonLab ENT (Celon AG medical instruments, Teltow, Germany). A disposable stylus delivered bipolar RF energy at 15 W to the inferior turbinates. The RF was applied to 15 to 30 non-overlapping positions on the inferior turbinate to shrink the turbinate and ablate the intra-turbinate neurovascular structures at the posterior part of the inferior turbinate. The procedure took approximately 20 min for both sides.
PNNN was performed using a 2W continuous wave laser with the AcuPulse™ CO2 laser (Lumenis Ltd, Yokne’am Illit, Israel) that was transmitted via a nasal probe angulated at 20° and a straight-tip 90° mirror, with smoke evacuation. The posterior middle meatus and supero-posterior portion of the inferior turbinate were cauterized to target the region supplied by the posterior nasal nerve. This procedure took approximately 6 to 8 min/side.
After the procedure, the inferior turbinate was covered with a thin sealing hemostat. A compression tamponade or nasal irrigation was not required after the surgery. Post-operation medication included an antihistamine, antibiotic, and analgesic were prescribed for 3 days. Patient was followed up after 1 week, 4 weeks, and 3 months by clinic interviewing or telephone follow-up at 3 months.
Surveys
Patients were evaluated using a 24 h rTNSS and Nasal Obstruction Symptom Evaluation (NOSE) scale.18,19 The 24 h rTNSS is a 4-item questionnaire whose score ranges from 0 to 20. The questionnaire focuses on the patient's recent symptoms of nasal congestion, rhinorrhea, itching, and sneezing within 24 h. The NOSE scale is a nasal symptom-related quality of life questionnaire composed of 5 items scored between 0 and 100. It reflects the quality-of-life restrictions in patients with nasal problems. 19 Postoperative complications were recorded during each follow-up visit.
Outcome Evaluation
The primary endpoint was the interval change of the rTNSS and NOSE questionnaire score and the score of each item in the scoring systems (subclass score) during the follow-up visits. To evaluate the surgery efficacy, the responder rate, defined as the minimal clinically important difference of ≥30% improvement [decrease] in rTNSS compared with the baseline score, was presented. To evaluate magnitude of surgery outcomes, score improvement ratios were presented and defined as (preoperative score − postoperative score)/preoperative score for each questionnaire scoring and subscores. Complications such as epistaxis, dry eyes, and headaches were also documented.
Statistical Analyses
Continuous data are presented as mean values with standard deviations for normally distributed data and as median values with interquartile ranges for skewed data in the tables. Categorical data are presented as counts (frequencies) and percentages. Changes in the survey scores from baseline were analyzed using 2-tailed paired t-tests for normally distributed data. The Wilcoxon signed-rank test was used to analyze skewed data. The Kolmogorov-Smirnov test is used to test the null hypothesis that a set of data comes from a normal distribution. A linear regression model was estimated to examine the effect of preoperative chronic rhinitis severity and different post-operation outcomes. Statistical analyses were performed using PASW Statistics (version 18.0.0, SPSS Inc., Chicago, IL, USA).
Results
A total of 183 patients (115 males; 62.8%) underwent surgery for resistant chronic rhinitis. All the patients had completed 1- and 3-month follow-up plan. The mean age of these participants was 38.5 ± 9.97 years. Preoperative comorbidities were distributed as follows: 19 patients (10.4%) had rhinitis medicamentosa, 28 patients (15.3%) had obstructive sleep apnea, and 14 patients (7.7%) had a history of septum/turbinate surgery, all of whom experienced rhinitis symptom recurrence. Additionally, 32 patients (17.5%) had a smoking habit. Twenty-six patients (14.2%) underwent combined septoplasty with RFIT and PNNN to ensure adequate passage to the posterior nasal meatus for PNNN. Complications occurred in 16 patients (8.7%). These complications included epistaxis requiring emergency room visits, prolonged crusting, wound infection, and short-term dry eye symptoms, which were self-limiting. When patients were divided into 2 groups based on preoperative rTNSS (mild: <5 and moderate-to-severe: ≥5), no statistically significant differences were observed between the groups for any of the factors (Table 1).
Demographic Data of the Study Cohort.
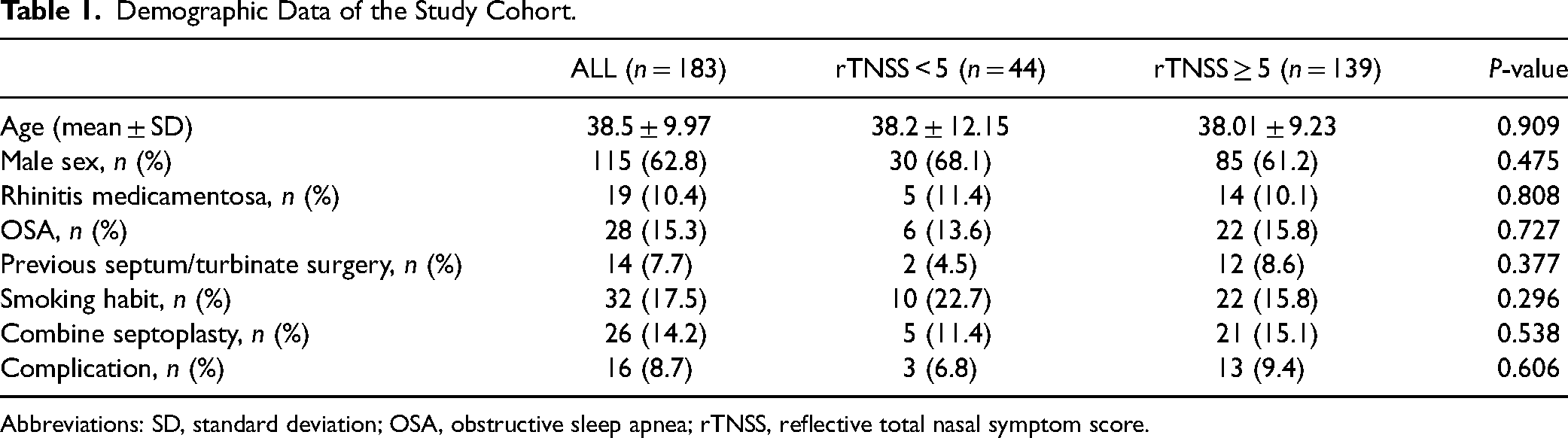
Abbreviations: SD, standard deviation; OSA, obstructive sleep apnea; rTNSS, reflective total nasal symptom score.
The mean preoperative rTNSS and NOSE scores were 6.51 ± 2.74 and 56.48 ± 19.90, respectively. One month postoperatively, the mean rTNSS was 2.55 ± 1.88, and the mean NOSE score was 11.39 ± 16.33. Three months postoperatively, the rTNSS was 1.70 ± 1.43, and the NOSE score was 4.56 ± 7.74. Both scores and all sub-scores showed significant differences when comparing preoperative, 1-month, and 3-month results (P < 0.001). Comparing rhinorrhea between 1 and 3 months showed a P-value of 0.008 and nasal itching between 1 and 3 months showed a P-value of 0.017 (Table 2). The response rate by rTNSS for whole cohort was 78.14 ± 41.44% and 93.99 ± 23.83% at 1- and 3-month follow-up, respectively. The symptom score improvement ratios were 70.5 ± 29.63% and 91.17 ± 16.28% at 3 months for rTNSS and NOSE, respectively (Figure 1).
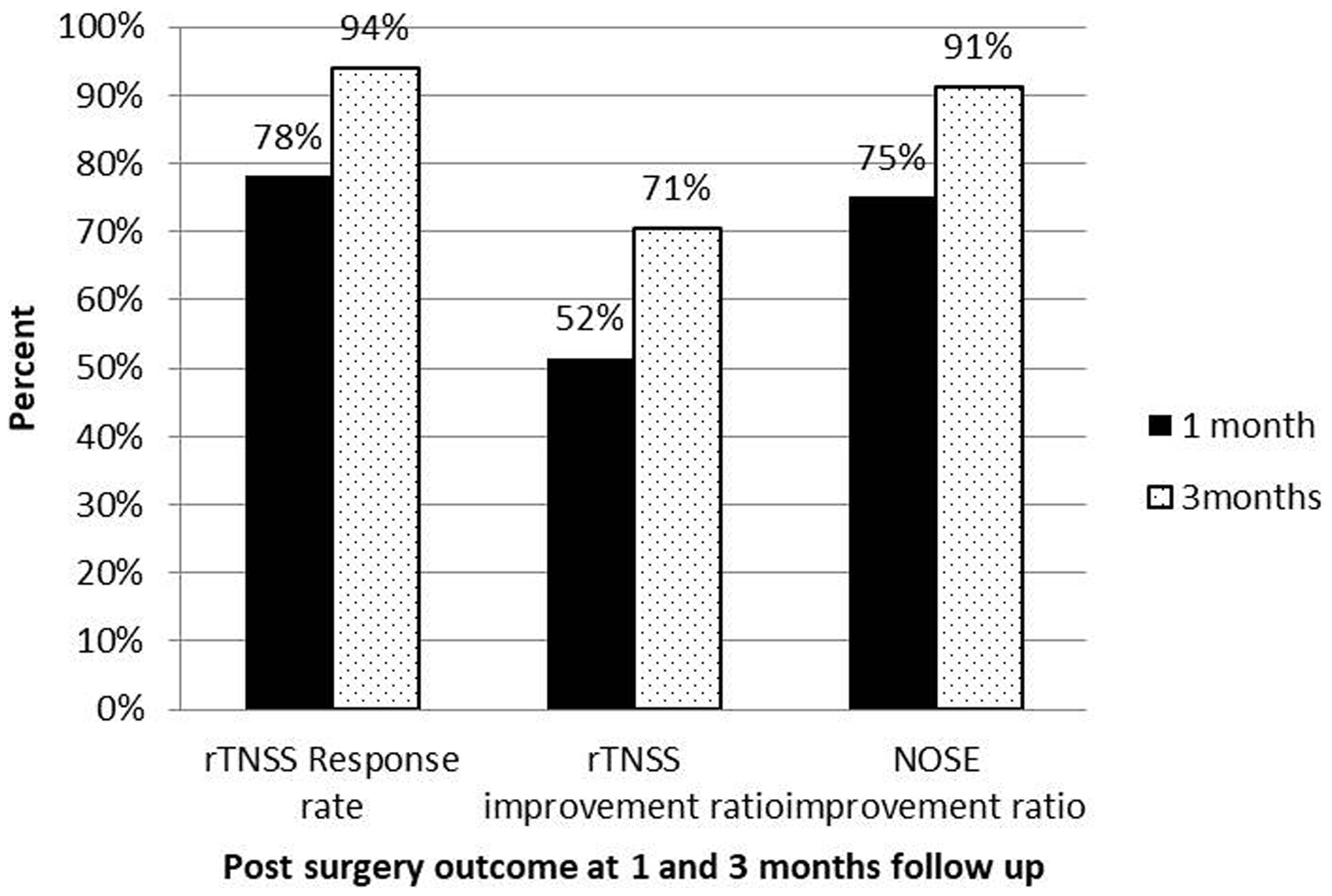
Post-surgery outcome including rTNSS responder rate and rTNSS and NOSE improvement ratio in 1 month and 3 months after RF ablation of the bilateral inferior turbinate with posterior nasal nerve neurolysis.
Follow-up Questionnaire Scorings After Chronic Rhinitis Surgery.
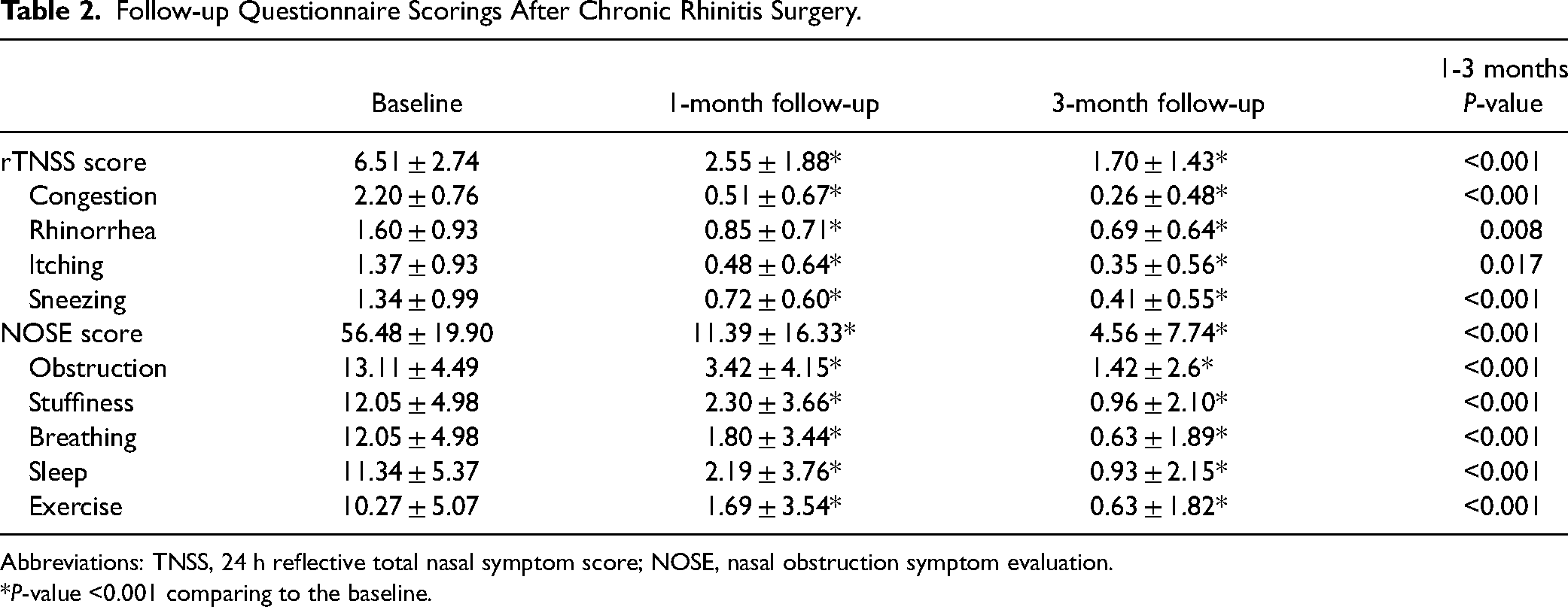
Abbreviations: TNSS, 24 h reflective total nasal symptom score; NOSE, nasal obstruction symptom evaluation.
P-value <0.001 comparing to the baseline.
To evaluate relationship between preoperative severity and surgery outcome, subgroup analyses were performed according to individual rTNSS scores and 2 in 1 score groups (ie, 1-2, 3-4, 5-6, 7-8, 9-10, and 11-12). The responder rate, change of rTNSS scores, and score improvement ratio during 1- and 3-month follow-up are summarized in Table 3. The distribution of 12 individual rTNSS score and 6 score groups were from a normal distribution by Kolmogorov-Smirnov test with P = 0.2 in both tests. Relationships with post-operation outcomes with preoperative severity by individual rTNSS scores and score groups are illustrated in Figures 2 and 3. Response rates were 50% and 75% with rTNSS score = 1 and increased to 100% after score = 8 and 7 in 1 month and 3 months, respectively. The postoperative rTNSS changes were 0.25 ± 1.5 and −0.75 ± 0.5 when rTNSS = 1 and gradually increased to −9.56 ± 1.67 and −10.11 ± 1.05 till score = 12 for 1 month and 3 months, respectively. The rTNSS score improvement ratio was −25% and 75% with rTNSS score = 1 and increased to 54% and 72% when score = 5% and 80% and 84% at score = 12 for 1 month and 3 months, respectively. Outcome results for rTNSS score groups were also presented in Table 3 with similar but more straightforward trends. Linear regression model was estimated to examine the effect of preoperative chronic rhinitis severity according to individual rTNSS score and score groups and different post-operation outcomes were presented in Table 4. Both preoperative individual score and score groups were significantly associated with all post-operation outcomes (P = 0.022 to <0.001). The model had best prediction for the postoperative rTNSS changes with preoperative rTNSS severity with R2 = 0.979-0.993 and P < 0.001 for individual score and score groups in both 1-month and 3-month outcomes. Linear regression analysis showed the preoperative rTNSS score group had better R2 of all outcomes compared to model with preoperative rTNSS score, indicating proposed 2 to 1 score group model had better prediction than individual preoperative rTNSS score.
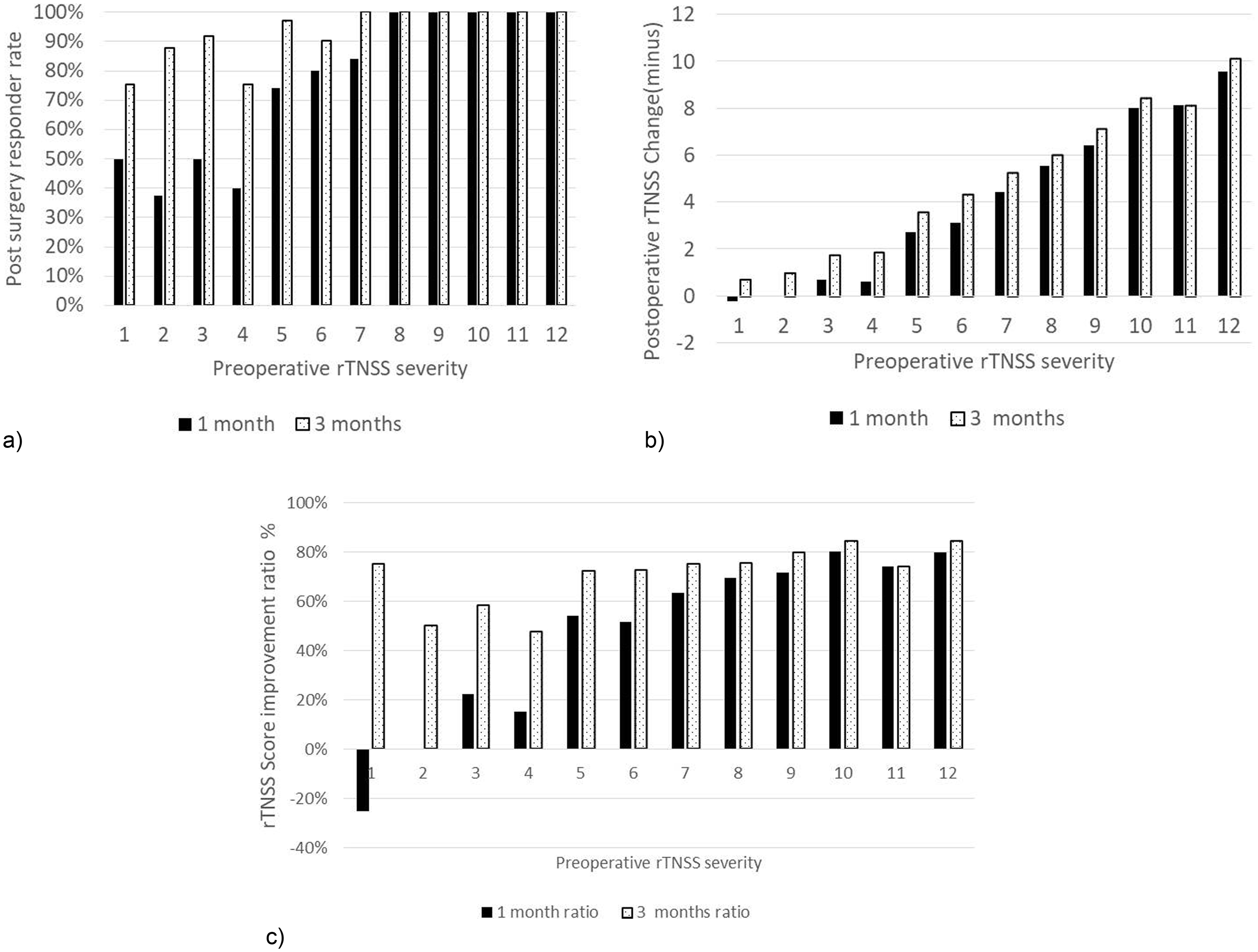
Post-surgery outcomes according to preoperative rTNSS severity by individual rTNSS score. (a) Response rate, β = 0.916 and 0.774 with P < 0.001 and 0.003 for 1- and 3-month outcomes, respectively. (b) Postoperative rTNSS change − β = 0.989 and 0.991 with both P < 0.001 for 1- and 3-month outcomes, respectively. (c) rTNSS score improvement ratio, β = 0.928 and 0.695 with P < 0.001 and 0.012 for 1- and 3-month outcomes, respectively.
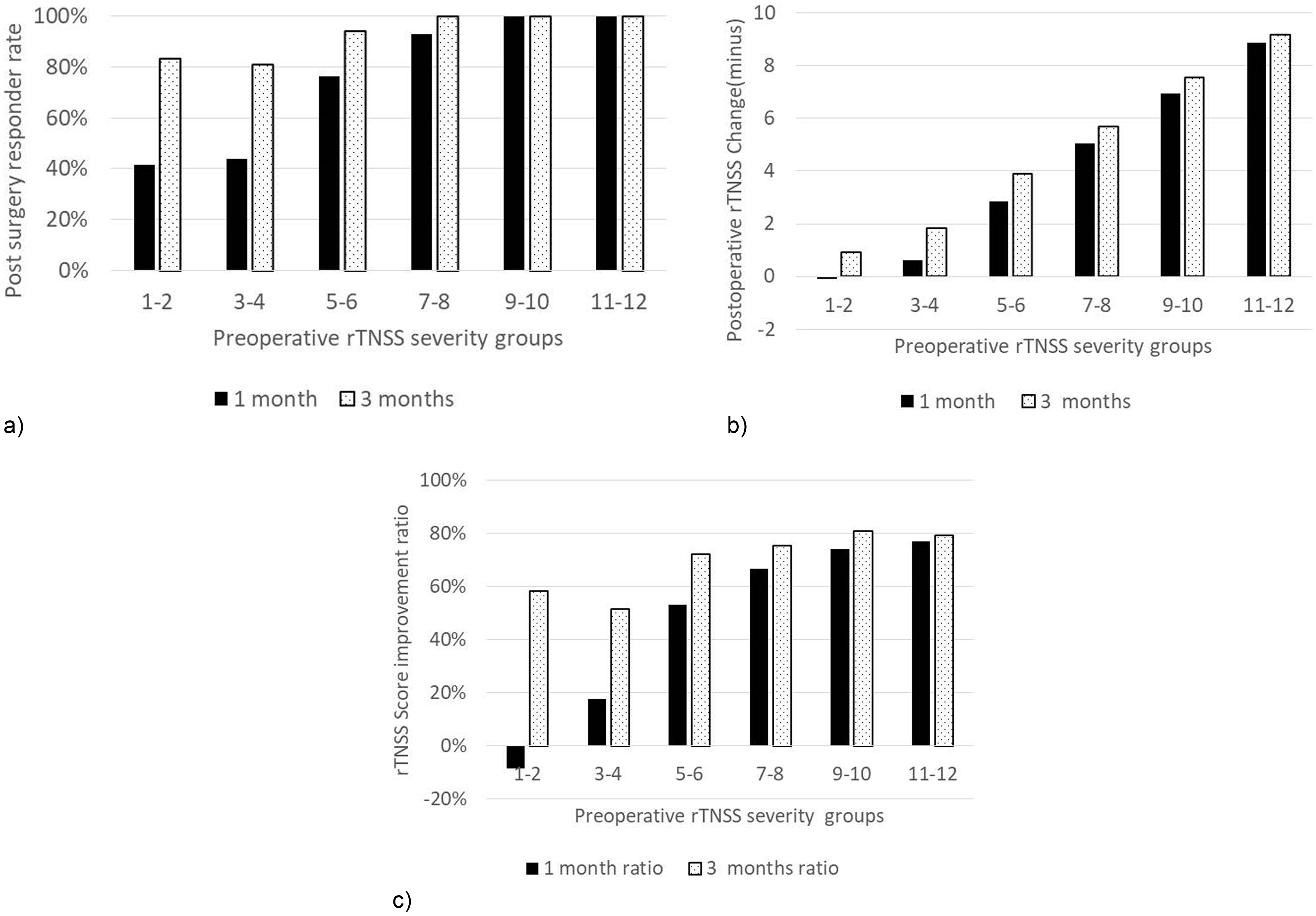
Post-surgery outcomes according to preoperative rTNSS severity by rTNSS score groups. (a) Response rate, β = 0.942 and 0.892 with P = 0.005 and 0.017 for 1- and 3-month outcomes, respectively. (b) Postoperative rTNSS change − β = 0.994 and 0.997 with both P < 0.001 for 1- and 3-month outcomes, respectively. (c) rTNSS score improvement ratio, β = 0.942 and 0.876 with P = 0.005 and 0.022 for 1- and 3-month outcomes, respectively.
Post-Chronic Rhinitis Surgery Outcome According to the Preoperative Individual rTNSS Score and Score Groups.
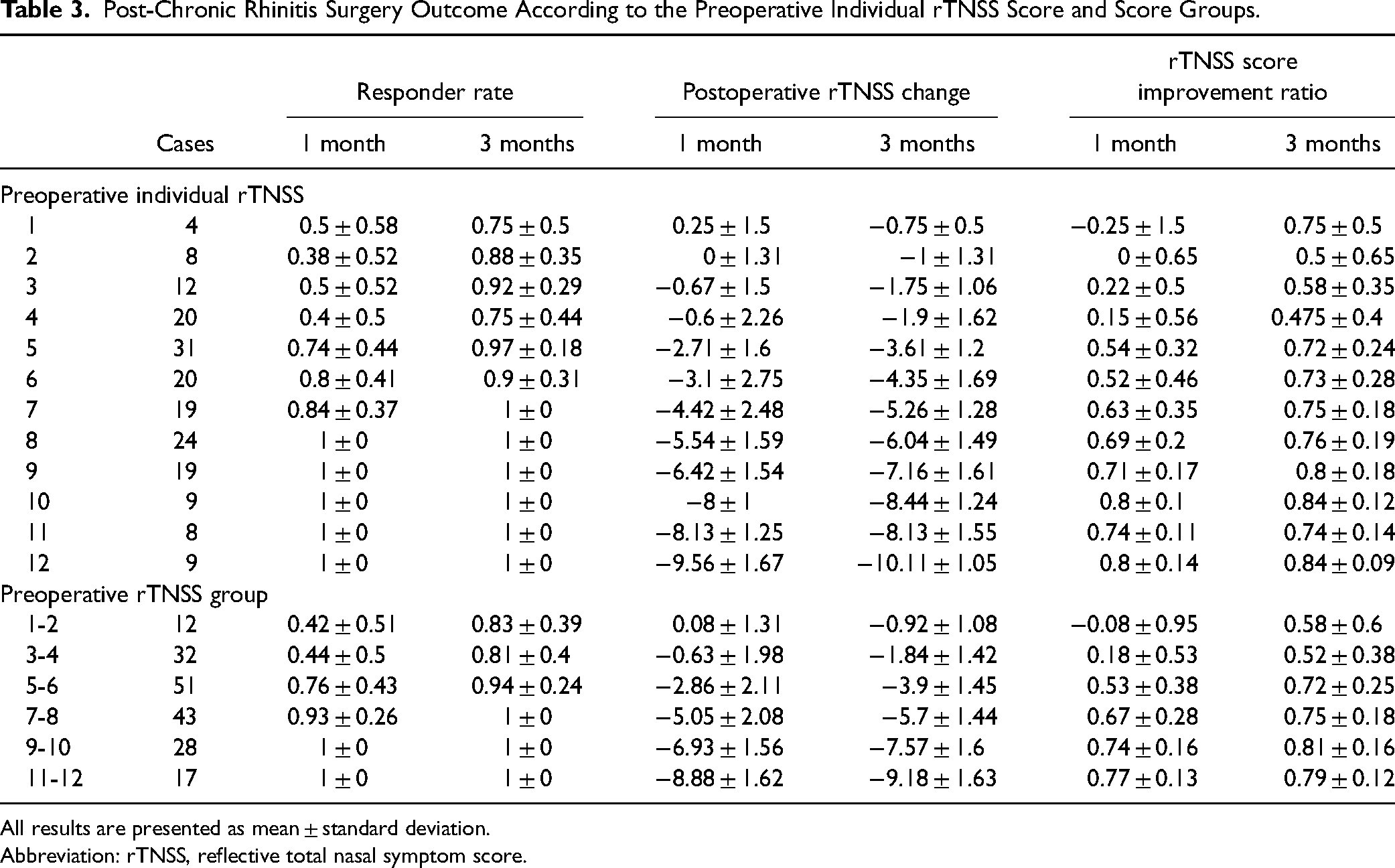
All results are presented as mean ± standard deviation.
Abbreviation: rTNSS, reflective total nasal symptom score.
Linear Regression Analysis Results for Each Postoperative Outcome.
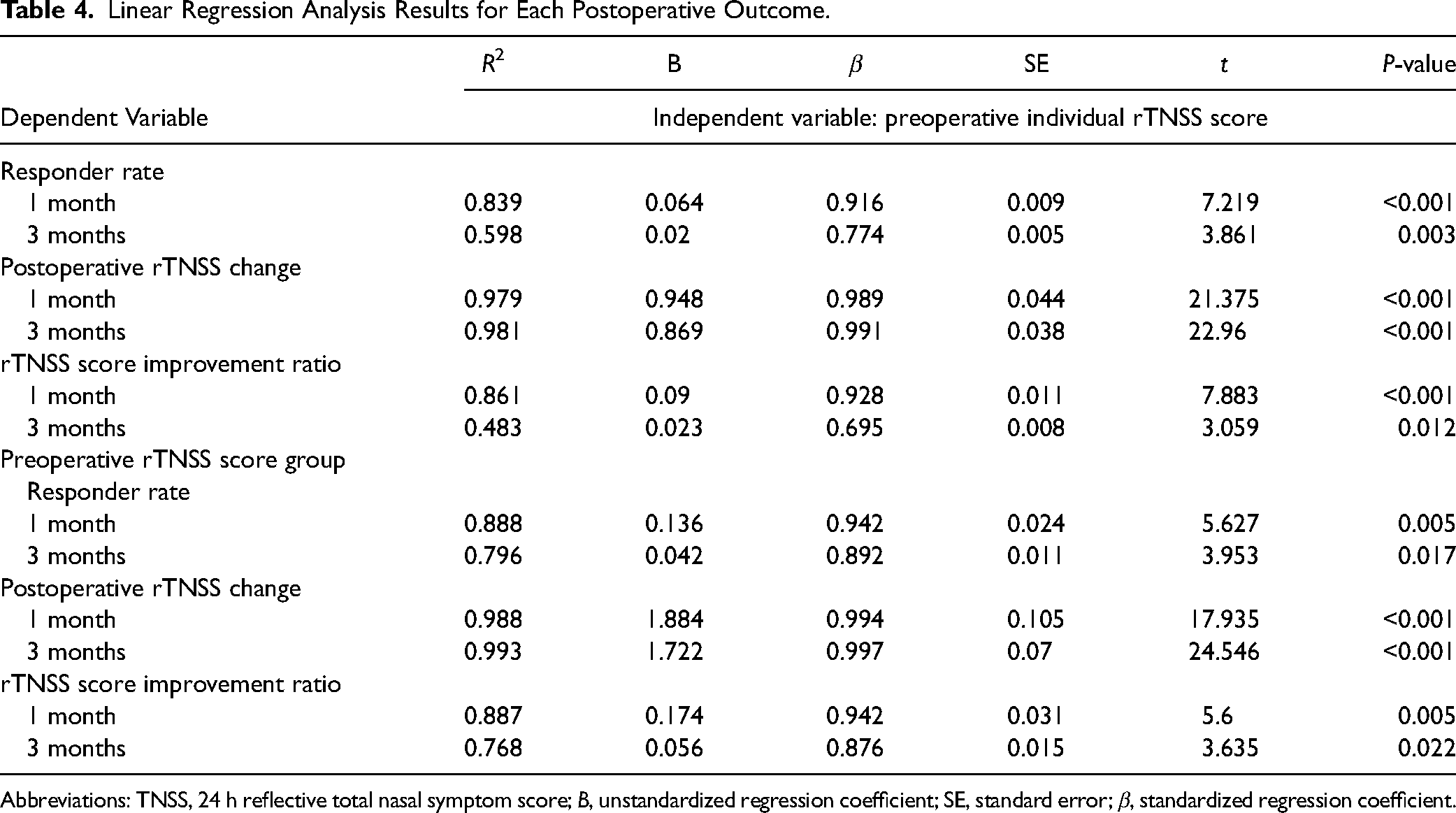
Abbreviations: TNSS, 24 h reflective total nasal symptom score; B, unstandardized regression coefficient; SE, standard error; β, standardized regression coefficient.
Postoperative complications including epistaxis, which required a visit to the emergency room, occurred in 4 patients. All the patients were examined by an otorhinolaryngologist. No serious posterior nasal bleeding was observed, and the short-term tamponade or surgical packing was removed within 3 days without any recurrent bleeding. Two patients complained of short-term dry eyes, which spontaneously resolved within 3 weeks without any further sequelae. Mild foul-smelling purulent discharge from the surgical bed might develop 2 to 3 weeks after the procedure. The symptoms can be resolved by removing all the crusting during the follow-up visit. No headache, ear discomfort, or severe nose pain was documented.
Discussion
Our study demonstrated a significant improvement in chronic rhinitis symptoms in patients receiving combined RF ablation of the inferior turbinates and PNNN surgery. Furthermore, we found that the response rate was significantly correlated with preoperative rTNSS scores, indicating that more severe disease predicts greater improvement in chronic rhinitis symptoms. To the best of our knowledge, this is the first study to explore the relationship between preoperative rTNSS scores and response rates in chronic rhinitis surgery.
Septoplasty was the mainstay of nasal obstruction surgery worldwide. In the United States alone, approximately 250 000 septoplasties are performed each year. The United Kingdom reports about 22 000 septoplasties annually.12,20 However, most septoplasty requires operation room and cost much more staff than office-based procedures. Thus, minimally invasive turbinate procedures including microdebridor turbinoplasty, coblation turbinoplasty, ultrasound turbinoplasty, RFIT, and PNNN have been developed for convenience with various levels of efficacy. 21 Lin et al 22 reported RFIT alone can effectively control symptoms of allergic rhinitis, including nasal obstruction, rhinorrhea, sneezing, and itchy nose and eyes, for up to 1 year postoperatively in the 51.3% to 63.9% range. 3 While the RF procedure was safe and easy to perform, the control of rhinorrhea and itching nose was not profound. A series of studies using temperature-controlled RF neurolysis demonstrated a 57.6% to 62.8% improvement in rTNSS scores in 3 months to 1 year.9,11,23 Cryotherapy PNNN has demonstrated the most significant improvement in symptoms such as rhinorrhea and congestion. 7 Krespi et al reported an overall improvement of 55% in the rTNSS and an improvement of 60% in symptom-specific scores (rhinorrhea and congestion) after PNNN with a diode laser. 15 To combine the advantage of early response and long-term control of rhinorrhea and sneezing, we combined the RFIT and PNNN, which showed satisfying early response rates with safety profiles.
The surgical outcome of chronic rhinitis varies according to different procedures and patient characteristics. Pedersen et al 24 reported that septoplasty + turbinoplasty yielded a 67% reduction, septoplasty alone a 62% reduction, and turbinoplasty a 45% reduction in the nasal obstruction VAS 0 to 100 scale score. In contrast to Pedersen's study, the results of our study were mainly that RFIT with PNNN showed highly effective results with NOSE scores that improved by 92% in 3 months per the 0 to 100 NOSE questionnaire.
Laser ablation of the posterior nasal nerve offers several advantages over other methods. The nasal probe, featuring a 20° angulation and a straight-tip 90° mirror with a smoke evacuation system, allows for a wide range of angles. This flexibility enables the ablation of nearly all mucosal areas innervated by the posterior nasal nerve without leaving any untreated spaces. The CO2 laser used in this procedure ensures shallow ablation, avoiding deeper tissue penetration. Consequently, it is safe, minimizes bleeding, and generates sufficient power to induce nerve injury.25,26 The CO2 laser is widely available in most otorhinolaryngology hospitals and operating rooms, which makes this procedure more accessible. CO2 laser ablation of the posterior nasal area was associated with complications such as intraoperative bleeding. The bleeding was controlled by packing the nasal cavity with cotton strips soaked in lidocaine/epinephrine. Further packing was achieved with Surgicel® if required.
Preoperative severity had a significant impact on the postoperative outcome and satisfaction. Pedersen et al 13 reported that 81% with severe nasal obstruction and 31% with mild nasal obstruction before surgery had improved. Only 56% reported that the results of the surgical operation were as they had expected. In another publication by Pedersen et al, 24 it was reported that almost 70% of patients with moderate nasal obstruction improved to mild obstruction. In the severe group, 90% of patients improved to either mild or moderate. Our study had presented detailed preoperative severity to post-chronic rhinitis surgery outcome data, which support the hypothesis that the preoperative rTNSS score was linearly correlated with the postoperative symptom score change and surgery outcome.
The response rate at 3 months was 77.11% and varied up to 12 months of follow-up in PNNN only cohort.6,9,11,16,17 Our study demonstrated by combining RFIT and PNNN, responder rate could be 94% as early as in 3 months. The magnitude of the improvement was also significant with 52% improvement within 1 month and 71% within 3 months in rTNSS scores. The NOSE score demonstrated a 75% improvement in 1 month and 91% improvement in the 3 months. Our results support the use of combining the 2 methods, we anticipated an early and promising treatment effect.
The current study has some limitations. First, the retrospective design could lead to selection bias, confounding the result. Second, we did not control for concurrent medication use and the questionnaire for nasal obstruction evaluation was subjective and varies to the environment and concomitant use of other medication. However, since the preoperative rTNSS and NOSE score were documented after medication failed to control the symptom and before surgery, these preoperative scores had already considered the effect of medical treatment since all patients had been tried adequate medical treatment before surgery. Thus, medical treatment was not restricted after the surgery to keep same background and examine individual differences. Third, the surgical procedure could be operator dependent in treatment extent. Meanwhile, the variation in surgery skills could be minimized by only enrolling single surgeon's (CYH) surgery outcome. Other limitations including lack of external validity of current single institute cohort and its relatively short follow-up period of only 3 months. However, considering the findings of previous RF and PNNN studies,3,9,11,23 changes beyond 3 months are limited. Nevertheless, we anticipate the sustained effectiveness of the results over longer periods. The promising study outcomes highlight the need for larger multicenter studies to externally validate our findings.
Conclusion
Patients with more severe preoperative chronic rhinitis symptoms, evaluated with rTNSS score, are associated with better response rate, post-operation symptom score changes, and score improvement ratio. The combination of PNNN to RFIT surgery significantly improved the chronic rhinitis symptoms in 1 month and 3 months. The 2 in 1 preoperation severity rTNSS score groups had better linear association with surgery outcomes and individual rTNSS preoperative scores.
Footnotes
Acknowledgments
We express our gratitude to Hsin-Yi Yang at the Chiayi Christian Hospital Clinical Data Center for her valuable statistical consultation and to Teng-Han Lo at the Chiayi Christian Hospital Otolaryngology Department for his assistance with data entry and organization.
Authors’ Contributions
CYH, JWH, BHK, and YSL designed and coordinated the study. CYH and JYL collected the clinical data and documented most cases. CYH contributed to writing the manuscript and drafting the manuscript. CYH and JWH critically reviewed the manuscript for important intellectual content. All authors read and approved the final manuscript.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of Chiayi Christian Hospital (No. CYCH2024022; April 12, 2024).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Ditmanson Medical Foundation Chia-Yi Christian Hospital Research Program(R113-056).