
Abstract
Background
Previous research has reported inconsistent results when evaluating long-term revision rates of patients undergoing balloon sinus dilation (BSD) compared to primary endoscopic sinus surgery (ESS).
Objective
We aimed to compare outcomes and long-term rates of revision surgery in patients with chronic rhinosinusitis without nasal polyps (CRSsP) who underwent primary standalone BSD versus primary ESS. We also wanted to better understand the post-procedure utilization of major healthcare resources between these groups.
Methods
Retrospective cohort study using the TriNetX platform to identify patients with CRSsP undergoing standalone BSD versus primary ESS. 1:1 propensity score matching was performed to balance age and gender in each cohort. The primary outcome was revision ESS rates at 1 and 10 years. Secondary outcomes were rates of healthcare utilization and complications, including orbital, cerebrospinal fluid (CSF) leak, and epistaxis within 90 days.
Results
After matching, each cohort had 2112 patients. At 1 year, the revision ESS rate was 3.5% in the balloon cohort and 3.5% in the ESS cohort (OR = 0.97, 95% CI: 0.70–1.35). Extending follow-up to 10 years, revision rates were also not statistically different: 5.8% in the balloon cohort and 6.3% in the ESS cohort (OR = 0.92, 95% CI: 0.72–1.19). Patients in the balloon cohort had a lower 90-day risk of inpatient encounters (OR = 0.29, 95% CI: 0.23–0.38), CRS-related patient visits (OR = 0.63, 95% CI: 0.55–0.71), diagnostic nasal endoscopies (OR = 0.57, 95% CI: 0.50–0.65), antibiotic prescriptions (OR = 0.53, 95% CI: 0.43–0.66), and corticosteroid prescriptions (OR = 0.62, 95% CI: 0.53–0.71).
Conclusion
No significant difference was observed in revision ESS rates in CRSsP patients who underwent primary BSD versus ESS after 10 years in this large database study. Findings suggest that in appropriately selected patients, BSD offers a durable response and a favorable value proposition in the management of patients with CRSsP.
Keywords
Introduction
Chronic rhinosinusitis without nasal polyps (CRSsP) is a highly prevalent inflammatory condition of the paranasal sinuses, significantly impacting patient quality of life and healthcare expenditures.1,2 Endoscopic sinus surgery (ESS) is considered the gold standard for the management of CRSsP patients who fail appropriate medical therapy. 3 ESS is a highly beneficial treatment modality in enhancing patient symptoms and patient-reported quality of life by improving sinus drainage and enhancing the delivery of topical medications. 4
In 2005, the U.S. Food and Drug Administration (FDA) granted approval for balloon sinus dilation (BSD) as a therapeutic technique for managing conditions affecting the paranasal sinuses. BSD involves the use of a high-pressure balloon inflated to two atmospheres to widen the sinus outflow tract by creating small microfractures of the surrounding bone and compressing the mucosal lining. BSD enhances sinus ventilation and drainage and can be performed as a standalone procedure or used as a tool in conjunction with conventional ESS. However, disadvantages of the procedure include the high cost of the device and limited data on long-term efficacy. 5
Several studies have evaluated BSD and determined it to be a safe and effective treatment alternative in patients with uncomplicated CRSsP without the need for removal of diseased tissue, polyps or a fungal ball.4–7 However, there is still ongoing debate about the long-term effectiveness of primary standalone BSD in comparison to ESS, particularly in terms of the likelihood of requiring revision ESS at some point in the future. Critics of BSD have pointed to the lack of long-term outcomes as a one of the barriers to adoption, arguing that patient QOL and health care utilization may not be improved with BSD-only procedures to the extent it might with ESS, especially if the BSD patient ends up needing a traditional ESS down the road anyways.
Previous studies have reported an increase in revision rates or no difference in revision rates in BSD patients when compared to those who have conventional ESS. However, these analyses have been performed with small cohorts of patients with limited follow-up periods.7–12 This study aimed to evaluate long-term revision surgery rates in patients with CRSsP who initially underwent either primary standalone BSD or primary ESS using a large-population-based database. Additionally, we sought to assess the differences in major healthcare resource utilization post procedure and complication rates between these two treatment groups, to further interrogate the underlying “value proposition” for performing standalone balloon procedures.
Materials and Methods
The U.S. Collaborative Network within the TriNetX Analytics platform comprises deidentified electronic health record (EHR) data from over 100 million patients across 68 healthcare organizations. A qualified expert, as defined under Section §164.514(b)(1) of the HIPAA Privacy Rule, has determined that this data platform is exempt from review by the Western Institutional Review Board (IRB). This study utilized electronic health record data—including demographic details—alongside International Classification of Diseases Tenth Revision (ICD-10) codes, Anatomical Therapeutic Chemical (ATC) Classification, and Current Procedural Terminology (CPT) codes to define cohorts, matched variables, and study outcomes. All data queries were conducted on August 3, 2025.
Cohort Selection
The BSD cohort consisted of all patients within the TriNetX database from August 3, 2005, to August 3, 2025, with CRSsP who underwent primary standalone BSD without a prior history of ESS (a detailed description of the cohort, including identification codes, is reported in Supplemental Materials 1). The ESS cohort consisted of all patients within the TriNetX database from the same time range with CRSsP who underwent primary ESS without a prior history of BSD (a detailed description of the cohort, including identification codes, is reported in Supplemental Materials 1). It is important to note that we intentionally only included patients with CRSsP, given that there is a growing consensus that performing standalone balloon procedures in the setting of nasal polyps is generally considered inappropriate.
Outcome Variables
The primary outcome of this study was rates of revision surgery (in the form of traditional ESS or BSD) between the BSD and ESS cohorts, within 1-year and 10-year time intervals. The CPT codes utilized for determining ESS revision rates include the following: 31253, 31254, 31255, 31256, 31257, 31259, 31267, 31276, 31287, and 31288. For analyzing the rate of revision BSD performed after the index BSD or ESS procedures, CPT codes utilized included: 31295-31298.
In addition, we also assessed healthcare utilization and complication rates within 90 days of primary BSD and ESS to determine differences in usage between the cohorts. We evaluated various relevant post-procedure resource utilization categories, including emergency room (ER) visits (TriNetX Visit: Emergency or CPT 1013711), inpatient visits (TriNetX Visit: Inpatient Encounter or CPT 1013659), visits related to CRSsP (ICD-10-CM J32), diagnostic nasal endoscopies (CPT 31231), antibiotic prescriptions (ATC S01AA), and oral corticosteroid prescriptions (H02). We also evaluated complication rates within 30 days of primary BSD and ESS, including orbital complications (ICD-10-CM H53.2, H54.0, H54.7, H53, H54.61, H54.62, H54.10, H59.129, and H59.3), epistaxis (R04.0), and CSF leak (G96.0). A detailed overview of identification codes utilized for outcome variable selection is reported in Supplemental Materials 1. Patients in the BSD and ESS cohorts were matched using 1:1 Propensity Score Matching for age, sex, turbinate reduction (CPT 30140), septoplasty (CPT 30520), rhinoplasty (CPT 1005721), allergic rhinitis (ICD-10-CM J30), deviated nasal septum (ICD-10-CM J34.2), GERD (ICD-10-CM K21), asthma (ICD-10-CM J45), and OSA (ICD-10-CM G47.33).
Statistical Analysis
All statistical analyses were performed using the advanced analytics capabilities within the TriNetX platform to compare cohorts. Odds ratios (OR) with 95% confidence intervals (CI) were calculated to assess differences between the experimental and control groups. Baseline and matched patient characteristics were evaluated using chi-squared tests for categorical variables and independent sample t-tests for continuous variables. Propensity score matching was conducted at a 1:1 ratio between BSD and ESS cohorts using logistic regression. The platform utilizes nearest-neighbor matching with a tolerance level of 0.01, ensuring that the standardized mean difference (SMD) between covariates remains at or below 0.1.
Results
Overall, there were a total of 2113 patients in the standalone BSD cohort and 69,322 patients within the ESS cohort.
ESS Revision Rates Within 1-Year: Short-Term
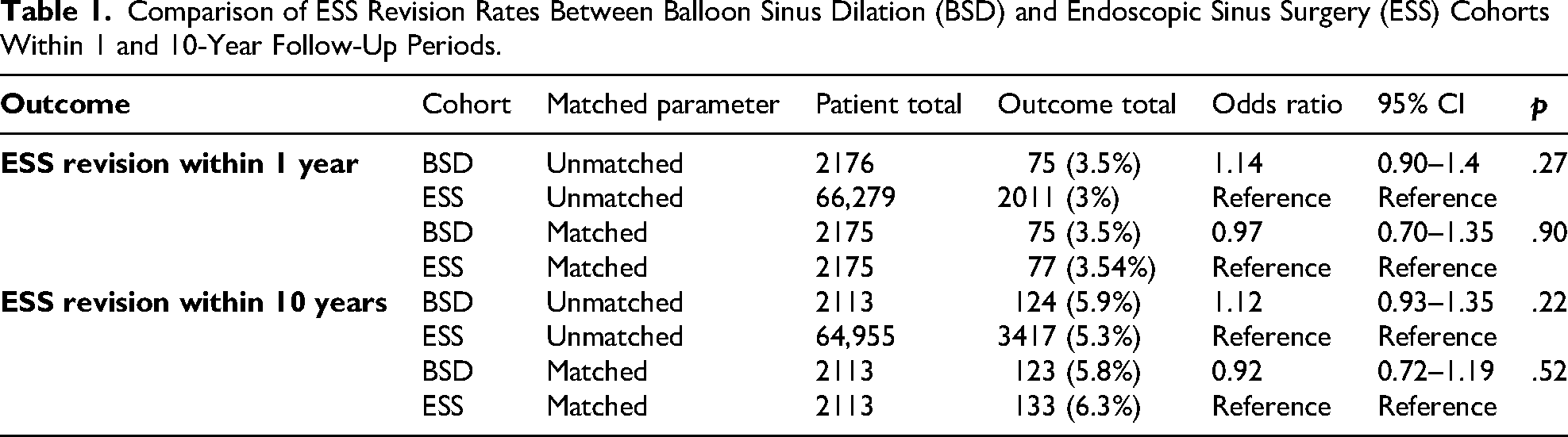
The median follow-up period was 365 days (IQR: 65) for the BSD cohort and 365 days (IQR: 81) for the ESS cohort when evaluating for revision rate outcomes up to 1 year. The overall revision rate was 3.5% for the BSD and 3% for the ESS cohorts. After 1:1 propensity score matching for age and female sex, there was no statistical difference in ESS revision rates within one year with an odds ratio (OR) of 0.97 (95% CI: 0.70–1.35, p = .27). Additional data for the unmatched and matched analyses are reported in Table 1.
Comparison of ESS Revision Rates Between Balloon Sinus Dilation (BSD) and Endoscopic Sinus Surgery (ESS) Cohorts Within 1 and 10-Year Follow-Up Periods.
ESS Revision Rates Within 10 Years: Long-Term
The median follow-up period was 1223 days (IQR: 2182) for the BSD cohort and 1161 days (IQR: 2111) for the ESS cohort when evaluating revision rate outcomes up to 10 years. The overall revision rates were 5.8% and 6.3% for the BSD and ESS cohorts, respectively. Extending the time interval for evaluating the ESS revision rate to 10 years continued to demonstrate no statistical difference in revision rates between the cohorts, with an OR of 0.92 (95% CI: 0.72–1.19) after 1:1 propensity score matching. Additional data for the unmatched and matched analyses are reported in Table 1.
Comparison of ESS Revision Rates Between Maxillary and Frontal BSD Versus ESS
In an attempt to account for disease severity, which cannot be assessed in the TriNetX database due to the lack of radiologic or symptomatic measures, we compared revision rates between frontal/maxillary BSD and ESS in patients with disease involving the same sinuses. After 1:1 propensity score matching, there was no difference in ESS revision rates between the BSD and ESS cohort at 1 year (OR: 0.88, 95% CI: 95%: 0.5–1.6) and 10 years (OR: 1, 95% CI: 0.66–1.5).
Balloon Sinus Dilation Revision Rates
We also evaluated the rate of revision balloon procedures following the index BSD. Revision BSD was uncommon, with only 2% of patients requiring repeat BSD at both 1 and 10-year follow-ups after 1:1 propensity score matching.
Healthcare Utilization Within 90 Days of Index Event
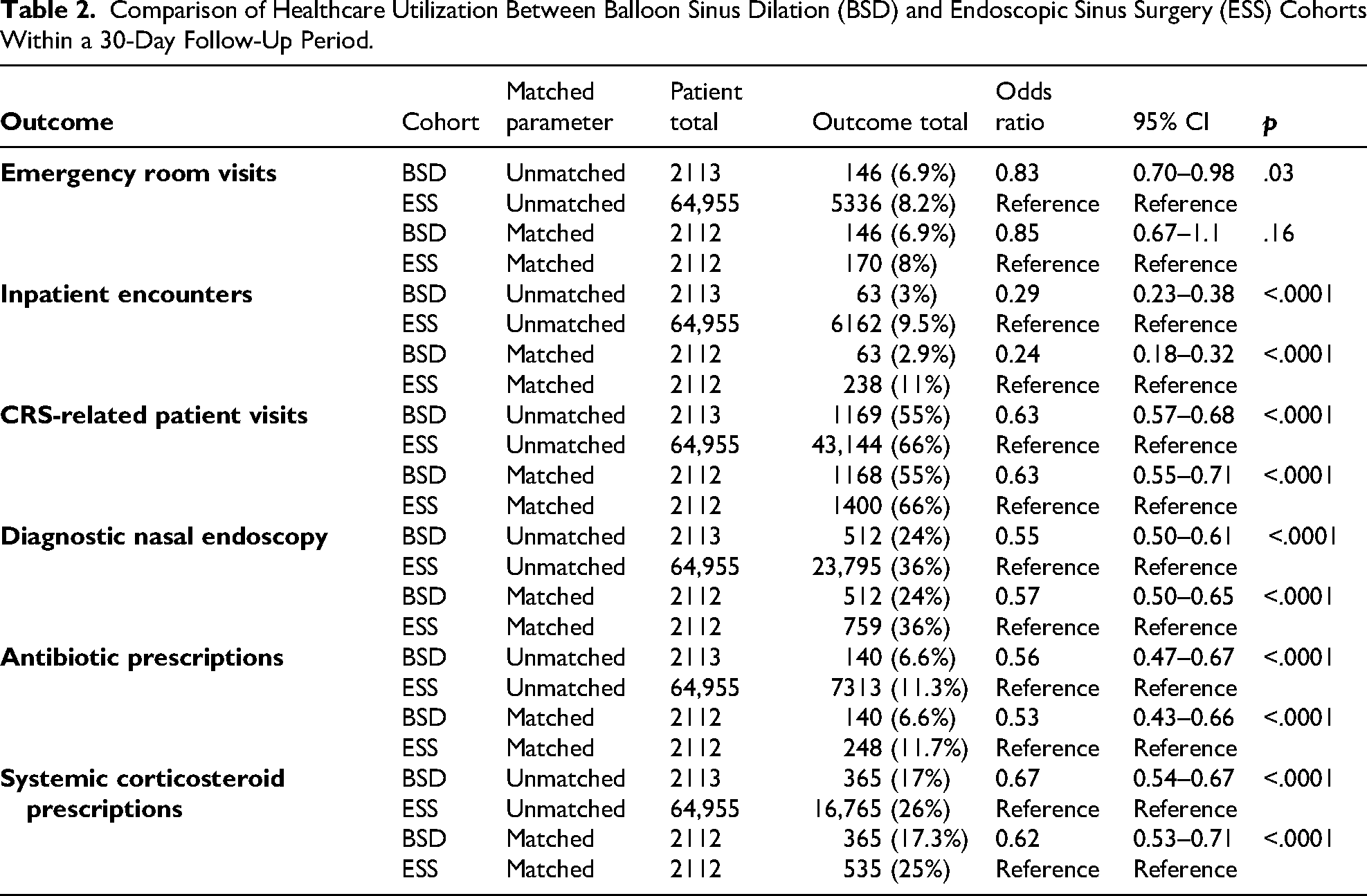
There was a statistically significant reduction in rates of inpatient encounters (OR = 0.24, 95% CI: 0.18–0.32), CRS-related patient visits (OR = 0.63, 95% CI: 0.56–0.71), diagnostic nasal endoscopies (OR = 0.57, 95% CI: 0.50–0.65), antibiotic prescriptions (OR = 0.53, 95% CI: 0.43–0.69), and corticosteroid prescriptions (OR = 0.62, 95% CI: 0.53–0.72) in the BSD cohort compared to the ESS cohort. Further data on the number of patients with each outcome and unmatched analysis are reported in Table 2.
Comparison of Healthcare Utilization Between Balloon Sinus Dilation (BSD) and Endoscopic Sinus Surgery (ESS) Cohorts Within a 30-Day Follow-Up Period.
Post-Operative Complication Rates Within 90 Days of Index Procedure
No statistically significant difference in the rates of epistaxis and CSF leak was found between the cohorts. Although extremely rare in both groups, there was a statistically significant reduced risk of orbital complications (OR = 0.34, 95% CI: 0.20–0.56) in the BSD cohort compared to the ESS cohort.
1:1 Propensity Score Matching
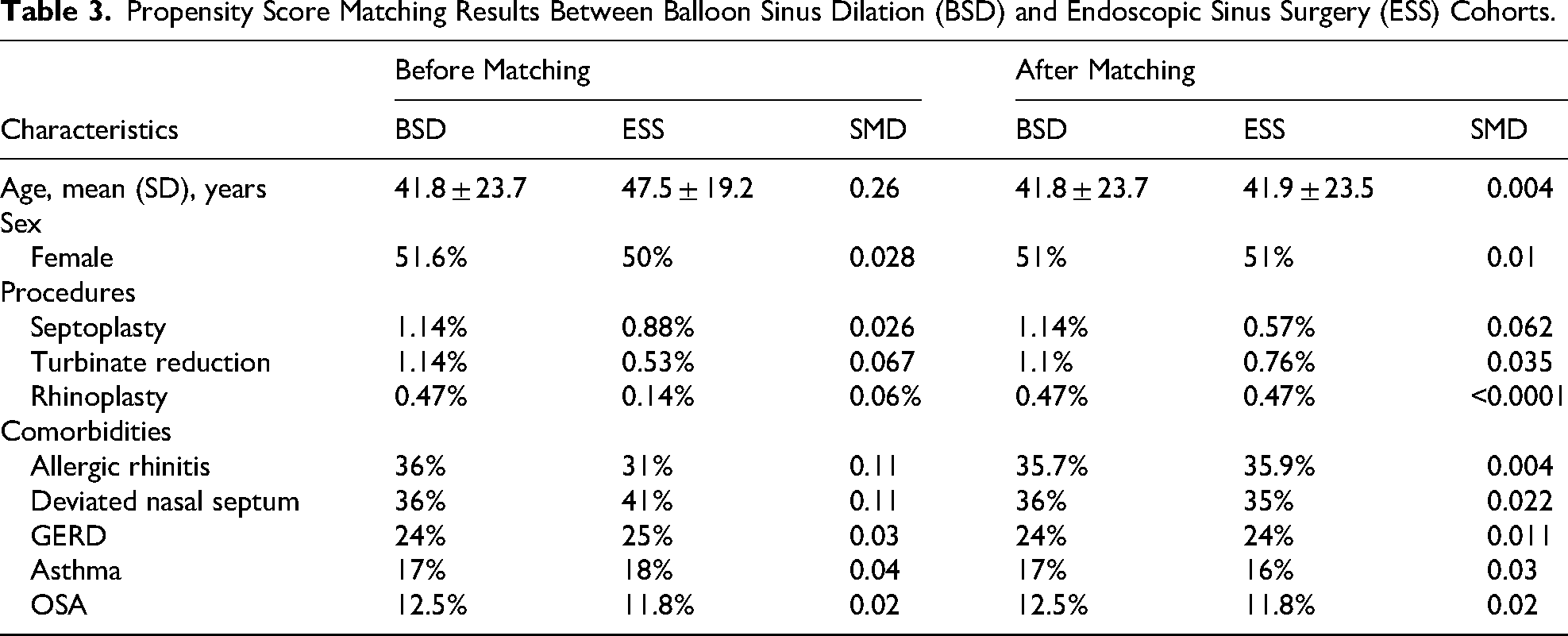
The results of the covariates used in the 1:1 propensity score matching are reported for the BSD and ESS in Table 3.
Propensity Score Matching Results Between Balloon Sinus Dilation (BSD) and Endoscopic Sinus Surgery (ESS) Cohorts.
Discussion
To our knowledge, this is the largest study with one of the longest follow-ups evaluating surgical revision rates and outcome differences between primary standalone BSD and primary ESS in the literature. The primary objective of this analysis was to evaluate the surgical revision rates between these two modalities over the long term and to establish whether or not upfront standalone BSD was associated with a higher risk of revision surgery, including formal ESS, even years post procedure. When assessing revision ESS rates over a 10-year period, the overall revision surgery rate was 5.8% in the BSD cohort and 6.3% in the ESS cohort, indicating comparable long-term revision rates between the two management approaches. In addition, there was also no statistical difference in revision surgery performed by balloon dilation between the BSD and ESS cohorts at 1 and 10 years. It is noteworthy that very few patients ended up having revision BSD performed over short term and long term periods.
When limiting the analysis to cases involving only the maxillary and frontal sinuses to control for disease, results for revision ESS in the BSD and ESS cohorts remained similar. We selected these specific sinuses as they are the most common sinuses to be treated with BSD. While these patients likely also underwent ethmoidectomy, it does appear that revision ESS remains similar between groups when controlling for the extent of surgery.
When viewed in conjunction with other published literature reporting patient QOL improvements following BSD, this finding suggests durable improvements when standalone BSD is performed in appropriately selected patients. 12 This finding is very significant because it helps to establish that patients who have BSD do not go on to require revision ESS at any greater rate than those who have their CRS treated with primary ESS. Meaning, that all things being equal, BSD appears to provide similar lasting improvements for an appropriately selected patient as does primary ESS when considering the need for revision surgery over the short and long term. The key here is, of course, in appropriately selecting those patients with CRSsP who would be good candidates for BSD.
Previous studies have compared revision rates between BSD and ESS albeit only over the short-term. In a combined study of a randomized controlled trial and meta-analysis by Chandra et al, there was no statistically significant difference in the mean change of Sino-Nasal Outcome Test (SNOT-20) scores or revision rates between the REMODEL FESS group and the combined six standalone balloon dilation studies at 1 year. 8 Similarly, several randomized control trials found no difference in the revision rates between the BSD and ESS cohorts at 3- and 6-month follow-up periods.7,9–12
As far as long-term outcomes, one study by Koskinen et al. of 77 BSD patients and 82 ESS patients found that the revision surgery rate following BSD was 22%, whereas it was significantly lower at 7% after ESS with a mean follow-up period of 5.3 years in the BSD group and 9.8 years in the ESS group. This study included a very small sample size, however. In contrast, our study, utilizing a large database and extensive sample size, contradicts this finding, as we observed no significant difference in revision rates between BSD and ESS out 10 years postoperatively. For added context, a previous study of over 4000 revision ESS surgeries demonstrated that the mean time until revision surgery was approximately 1.5 years. 13 Our findings are further supported by a meta-analysis encompassing five randomized controlled trials and four cohort studies with varying follow-up durations, which demonstrated similar revision rates between these two approaches.9,10,14–19 As a result, we believe that primary BSD is likely not associated with an increased risk of revision ESS in appropriately selected patients, as reported in the Clinical Consensus Statement: Balloon Dilation of Sinuses by Piccirillo et al. 12
Our study also demonstrated that primary BSD was associated with a significant reduction in healthcare resource utilization. When compared to the ESS cohort, primary BSD patients had a statistically significant reduction in rates of inpatient encounters, CRS-related outpatient visits, diagnostic nasal endoscopies, and antibiotic and corticosteroid prescriptions post-procedure. Similarly, the REMODEL study found a significant reduction in work/school days missed, antibiotic prescriptions, physician/nurse visits, and acute infections in the BSD only cohort. 8 Thus, a growing body of evidence is establishing that BSD is appears to be associated with a significant reduction in healthcare utilization when performed on appropriately selected CRSsP patients, likely attributable to its minimally invasive nature.
We also evaluated complication rates between the BSD and ESS cohorts and found a statistically significant difference in the rate of orbital complications, with a lower risk for the BSD cohort. However, there was no difference in the rate of postoperative epistaxis and CSF leak noted. A recent meta-analysis of several studies comparing ESS to BSD found no difference in the rate of major complications between the studies evaluated. 20 It should be underscored that BSD is certainly associated with a similar complication profile to ESS, and the potential for these complications should be openly and honestly discussed with patients during the informed consent process.
As far as the value proposition for the use of the BSD as a standalone procedure, the central issue here lies in the ability to select patients appropriately. Critics of balloon-only procedures have raised concerns over the potential increased risk of the need for revision procedures, including having to perform traditional ESS after the potential failure of BSD. 21 In this scenario, any value-proposition which may have saved a trip to the OR and other attendant costs related to upfront conventional ESS may appear to have been saved initially, but in fact, if a revision ESS is later needed anyways after the BSD, then the costs to the healthcare system would have been unnecessarily inflated. The long-term revision surgery rates in the present study help to allay some of these concerns, and the data presented on the healthcare utilization support the existing literature which suggests that indeed there are financial advantages to successfully treating CRSsP with a BSD-only procedure where appropriate.
There are several limitations of this study. Given the retrospective design of this study, we cannot establish causality but can only identify associations based on our findings. Additionally, the TriNetX platform does not include data on symptom severity or patient-reported outcomes limiting our ability to assess subjective treatment response between BSD and ESS cohorts. Furthermore, we are unable to view endoscopic examinations or imaging studies of patients in the TriNetX platform to assess for ourselves the severity of objective findings seen in CRSsP. It is also valid that the extent of disease may be less in the BSD group. While limited by our database-methodology, we attempted to explore this through our subset comparison of maxillary and frontal sinus procedures only. It is also true that ESS addresses the ethmoid sinus whereas BSD does not which also needs to be called out in a study comparing the two approaches. Additionally, administrative databases are entirely reliant on the data (ICD-9, CPT codes, etc.) that is entered, with no ability to scrutinize or corroborate them. Nonetheless, our study provides valuable insights on revision surgery rates, and healthcare utilization between standalone BSD and ESS in a large cohort of patients over a long period of time. Based on the results of our study and the available literature, we would conclude that the value proposition for the use of standalone balloon procedures, in appropriately selected CRSsP patients, is actually quite favorable and not overinflated.
Conclusion
In this large database study, no significant difference in revision ESS rates was found between CRSsP patients who underwent primary BSD versus ESS at 1- and 10-year time intervals. Patients undergoing BSD also had significantly less healthcare utilization postoperatively. These findings suggest that when carefully selected, CRSsP patients can achieve durable improvement with BSD, and there appears to be a strong value proposition in performing standalone balloon procedures.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924251377259 - Supplemental material for Comparison of Long-Term Revision Rates and Health Care Utilization Between Standalone Balloon Sinus Dilation and Endoscopic Sinus Surgery in Chronic Rhinosinusitis Patients Without Nasal Polyps: Is the Balloon Value Proposition Overinflated?
Supplemental material, sj-docx-1-ajr-10.1177_19458924251377259 for Comparison of Long-Term Revision Rates and Health Care Utilization Between Standalone Balloon Sinus Dilation and Endoscopic Sinus Surgery in Chronic Rhinosinusitis Patients Without Nasal Polyps: Is the Balloon Value Proposition Overinflated? by David Hoying, Matthew J Kabalan, David C Kaelber and Raj Sindwani in American Journal of Rhinology & Allergy
Footnotes
Ethical Approval and Informed Consent Statements
Ethical approval was not required. A qualified expert, as defined under Section §164.514(b)(1) of the HIPAA Privacy Rule, has determined that this data platform is exempt from review by the CWRU Institutional Review Board (IRB). Consent for participation and publication is not applicable for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the Clinical and Translational Science Collaborative of Cleveland, which is funded by the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Science Award grant, UL1TR002548. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
Dr. Sindwani is a consultant for 3D Matrix, Stryker, and Optinose. He also receives honoraria from Elsevier (textbooks) and Sage (Editor-and-Chief). None of these are relevant to this publication. All other authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available within the TriNetX platform.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.