
Abstract
Objectives
While autoimmune diseases (ADs) are known for systemic inflammation, their specific association with upper airway inflammation (UAI) has not been extensively characterized. We aim to investigate the associations between various ADs and subsequent UAI development in a large, national cohort.
Methods
This retrospective cohort study utilized de-identified electronic health records from TriNetX, a national collaborative database. Adolescent and adult patients with a diagnosis of 1 or more ADs were identified. A 12 month washout period was implemented to exclude preexisting UAI. The primary outcome was the incidence of UAI (chronic rhinosinusitis, allergic rhinitis, nonallergic rhinitis, chronic laryngitis, obstructive sleep apnea) following AD diagnosis. Hazard ratios and relative risks (RRs) with 95% confidence intervals (CIs) were calculated.
Results
After propensity matching, 1 327 186 patients with ADs and 1 327 186 controls were included. Patients with ADs exhibited a significantly lower overall incidence of UAI compared to controls (9.11% vs 13.81%; RR 0.71, 95% CI 0.70-0.71). This reduced risk was notable for allergic rhinitis (RR 0.64, 95% CI 0.64-0.65) and chronic sinusitis (RR 0.88, 95% CI 0.87-0.89). Juvenile idiopathic arthritis and type 1 diabetes demonstrated the most pronounced reductions in UAI risk. However, granulomatosis with polyangiitis and eosinophilic granulomatosis with polyangiitis were associated with a significantly increased risk of UAI.
Conclusion
Most ADs were associated with a reduced overall risk of subsequent UAI. However, certain vasculitides significantly increased UAI risk, highlighting disease-specific pathophysiological mechanisms. These findings suggest a complex interplay between systemic autoimmunity and localized airway inflammation, warranting further investigation into underlying mechanisms and the impact of AD treatments.
Keywords
Introduction
Upper airway inflammation (UAI) is an intricate disease process manifesting in several conditions. Although acute episodes are often self-limiting, chronic or severe inflammation can persist for up to several months which can significantly hinder respiratory function and quality of life. 1 The underlying etiology driving UAI is multifaceted as it involves complex interactions between genetics, environmental irritants, dysregulated epithelial barriers, and inflammatory mediators, all which eventually result in regional inflammation. 2 Despite extensive research, the role of such inflammation in the context of preexisting autoimmune conditions has not been thoroughly investigated.
Autoimmune diseases (ADs) are characterized as excessive immune reactions to self-antigens, although they have been shown to contribute to systemic inflammation beyond their primary sites of involvement. Recently, population-based and observational studies in Asian and European nations have explored the potential association between select AD and UAI.3,4 This has been attributed to ADs modifying cellular transduction signaling pathways, influencing pathogenesis for specific conditions in the upper airway such as chronic rhinosinusitis (CRS) and nasal polyposis.5,6 However, this reveals a gap and motivates further investigation in large-scale research that examines the broader relationship between autoimmunity and UAI in the general population. Given the rising prevalence of ADs around the world, it becomes more feasible and ever so important to investigate these potential associations. 7 Furthermore, the coexistence of UAI may require increases or changes in medications that were already established for the baseline ADs. Indeed, this investigation can provide valuable insight into managing these conditions and developing targeted therapeutic strategies.
In this study, we aim to utilize the TriNetX network to characterize the associations between various ADs and UAI conditions in a large, real-world cohort of multinational populations. Leveraging this comprehensive healthcare data platform, we sought to determine the incidence of UAI following AD diagnosis, identify high-risk AD categories, and evaluate significant prognostic factors.
Methods
Study Design and Data Source
This retrospective cohort study utilized data from the TriNetX United States Collaborative Network, a federated health research platform providing access to de-identified electronic health records from 68 healthcare organizations. The dataset included demographic information, diagnoses, procedures, laboratory results, and medication records. This analysis was performed on March 31, 2025, and received exempt status from the Institutional Review Board as it exclusively involved de-identified data.
Patient Population
We identified patients with ADs using ICD-10-CM diagnostic codes (Supplemental Table 1). The index date was defined as the first recorded diagnosis of the autoimmune condition during the study period. Inclusion criteria consisted of age between 12 and 50 years at the time of diagnosis, confirmed diagnosis of at least 1 AD, had 2 or more encounters in the healthcare system (Z00-Z13). Patients with preexisting UAI conditions (CRS, allergic rhinitis, or chronic laryngitis) during the 12 month baseline period were excluded to focus on incident cases. A comparison cohort of patients without ADs was identified and matched to the autoimmune cohort based on propensity scores.
Exposure and Outcome Definitions
The primary exposure was the presence of an AD, categorized into 7 major groups: (1) rheumatologic (rheumatoid arthritis, systemic lupus erythematosus, Sjögren's syndrome, ankylosing spondylitis); (2) gastrointestinal (Crohn's disease, ulcerative colitis, celiac disease); (3) endocrine (type 1 diabetes mellitus, Hashimoto's thyroiditis, Graves’ disease); (4) dermatologic (psoriasis, vitiligo, pemphigus); (5) neurologic (multiple sclerosis, myasthenia gravis); (6) vasculitides (granulomatosis with polyangiitis (GPA), eosinophilic granulomatosis with polyangiitis (eGPA), giant cell arteritis); and (7) other ADs.
The primary outcome was the development of UAI conditions, identified using ICD-10-CM codes: CRS, allergic rhinitis, nonallergic rhinitis, chronic laryngitis, and obstructive sleep apnea (Supplemental Table S2).
Propensity Score Matching
To mitigate selection bias and control for potential confounding variables, we performed propensity score matching. Covariates included in the propensity score model were age, sex, race/ethnicity, socioeconomic determinants, body mass index, smoking status, and comorbidities including asthma, atopic dermatitis, anxiety, depression, chromosomal abnormalities, congenital abnormalities, immune deficiency disorders, socioeconomic disparities, and malnutrition. To address the potential impact of immunosuppressive therapy on outcomes, we performed additional analyses adjusting for exposure to systemic corticosteroids, conventional disease-modifying antirheumatic drugs, and biologic agents. Matching was conducted at a 1:1 ratio using a nearest-neighbor algorithm with a caliper width of 0.2 of the standard deviation of the logit of the propensity score. Balance between cohorts was assessed using standardized mean differences, with values <0.1 considered indicative of adequate balance.
Follow-up and Outcome Assessment
Follow-up began the day after the index date and continued until the first occurrence of an outcome event. The primary analysis assessed the time to first diagnosis of any UAI condition. Secondary analyses evaluated the risk of specific conditions (CRS, allergic rhinitis, and chronic laryngitis) independently.
Statistical Analysis
Baseline characteristics of the study cohorts before and after propensity score matching were described using counts and percentages for categorical variables and means with standard deviations or medians with interquartile ranges for continuous variables. Differences between groups were assessed using standardized mean differences before matching and appropriate statistical tests after matching. For time-to-event analyses, Kaplan–Meier survival curves were generated, and differences between groups were assessed using the log-rank test. Hazard ratios with 95% confidence intervals (CIs) were calculated using Cox proportional hazards models. For binary outcomes, risk differences and risk ratios with 95% CIs were calculated. Statistical significance was set at P < .05, and all tests were 2-sided. Statistical analyses were performed using the TriNetX platform's integrated analytics tools, with additional analyses conducted in R statistical software (version 4.2.0, R Foundation for Statistical Computing, Vienna, Austria).
Results
Study Population Characteristics
The initial TriNetX cohort included 128 695 089 patients across 71 healthcare organizations. After applying the inclusion and exclusion criteria, 1 349 146 patients with ADs and 6 573 535 controls were identified. Following 1:1 propensity score matching, 1 327 186 patients with ADs were matched to 1 327 186 controls, yielding a final study population of 2 654 372 patients. Baseline characteristics were well-balanced after matching, with all standardized mean differences below 0.1 (Table 1).
Baseline Characteristics Before and After Propensity Score Matching.
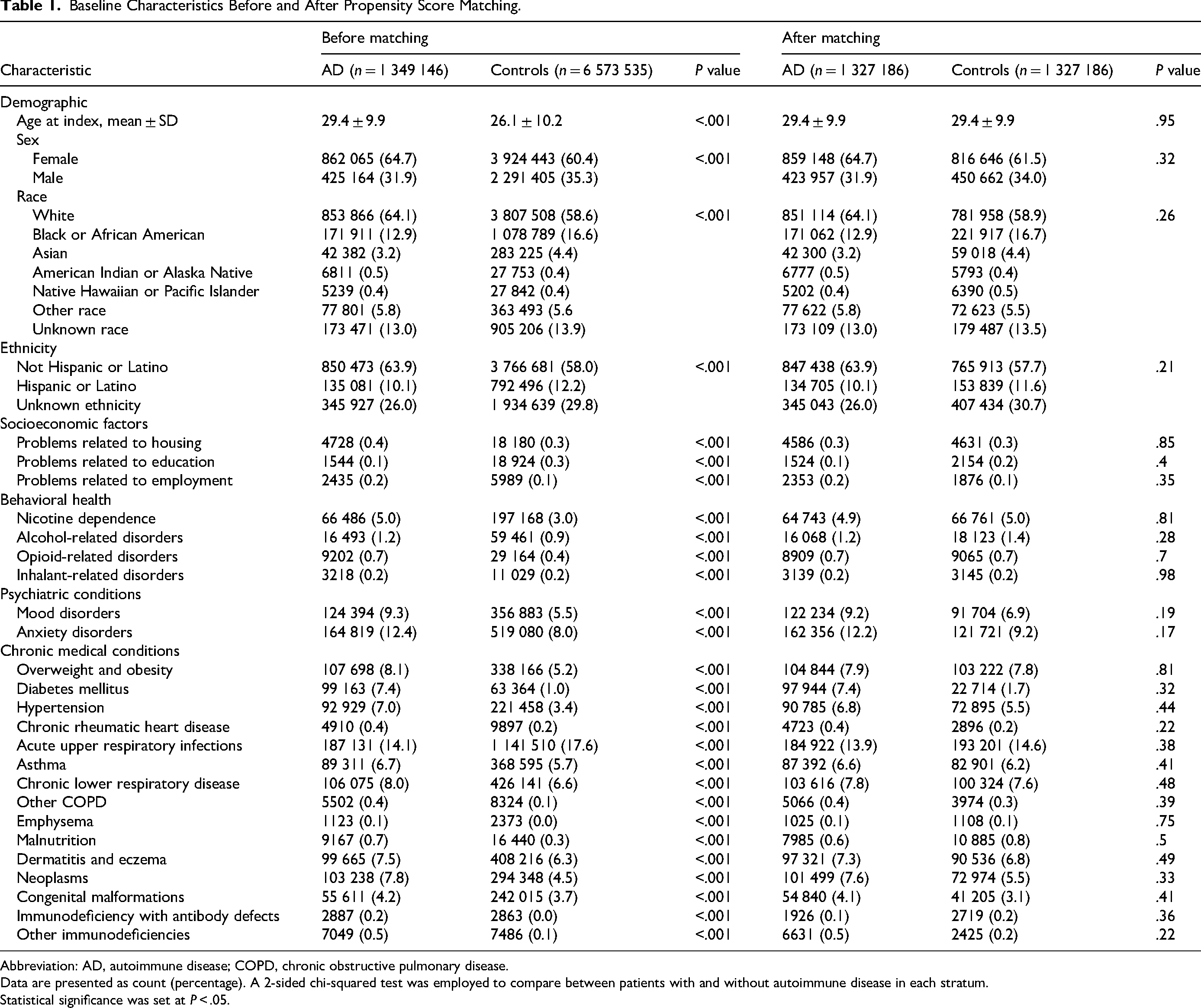
Abbreviation: AD, autoimmune disease; COPD, chronic obstructive pulmonary disease.
Data are presented as count (percentage). A 2-sided chi-squared test was employed to compare between patients with and without autoimmune disease in each stratum.
Statistical significance was set at P < .05.
The mean follow-up duration was approximately 46 ± 46 months (3.8 years) in the AD cohort and 54 ± 45 months (4.5 years) in the control cohort. The median follow-up time was 32 months (2.7 years) in the AD cohort and 44 months (3.7 years) in the control cohort. Some patients were followed for up to 20 years.
Risk of Upper Airway Inflammatory Conditions
Patients with ADs exhibited a significantly lower incidence of UAI compared to matched controls (9.11% vs 13.81%; relative risk [RR] 0.71, 95% CI 0.70-0.71; P < .001). Among specific conditions, allergic rhinitis and chronic sinusitis were notably less frequent in the AD cohort (RR 0.64 and 0.88, respectively; P < .001 for both). Chronic laryngitis and obstructive sleep apnea also occurred less often among AD patients. No significant difference was observed for chronic rhinitis (RR 1.02, 95% CI 1.00-1.04; P = .06) (Table 2).
Risk of Upper Airway Inflammation in Autoimmune Diseases.
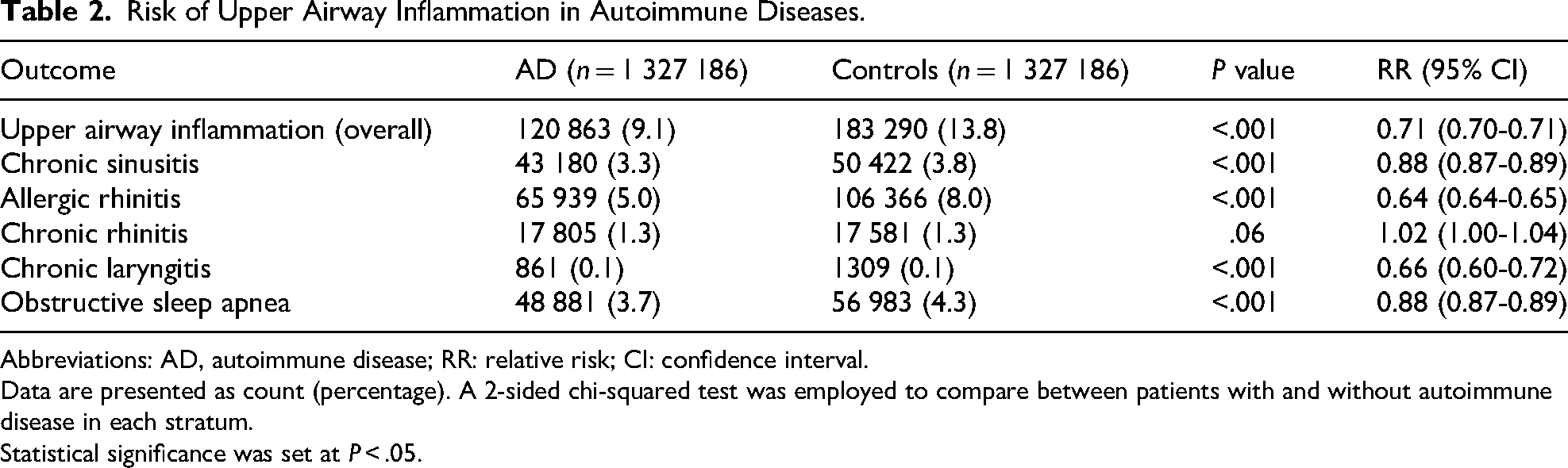
Abbreviations: AD, autoimmune disease; RR: relative risk; CI: confidence interval.
Data are presented as count (percentage). A 2-sided chi-squared test was employed to compare between patients with and without autoimmune disease in each stratum.
Statistical significance was set at P < .05.
Disease-Specific Risk Stratification
Across major AD categories, patients consistently exhibited a significantly reduced risk of UAI conditions compared to matched controls. This protective association was particularly prominent in endocrine, rheumatologic, gastrointestinal, dermatologic, and neurologic disorders. Among these, juvenile arthritis and type 1 diabetes showed the most pronounced reductions.
In contrast, vasculitis exhibited a divergent pattern: GPA and eGPA were associated with a significantly increased risk of UAI. Giant cell arteritis, however, did not show a statistically significant difference. Celiac disease and psoriasis, while still associated with lower UAI risk, showed relatively attenuated reductions compared to other autoimmune conditions (Table 3).
Risk of Upper Airway Inflammation Stratified by Specific Autoimmune Diseases.
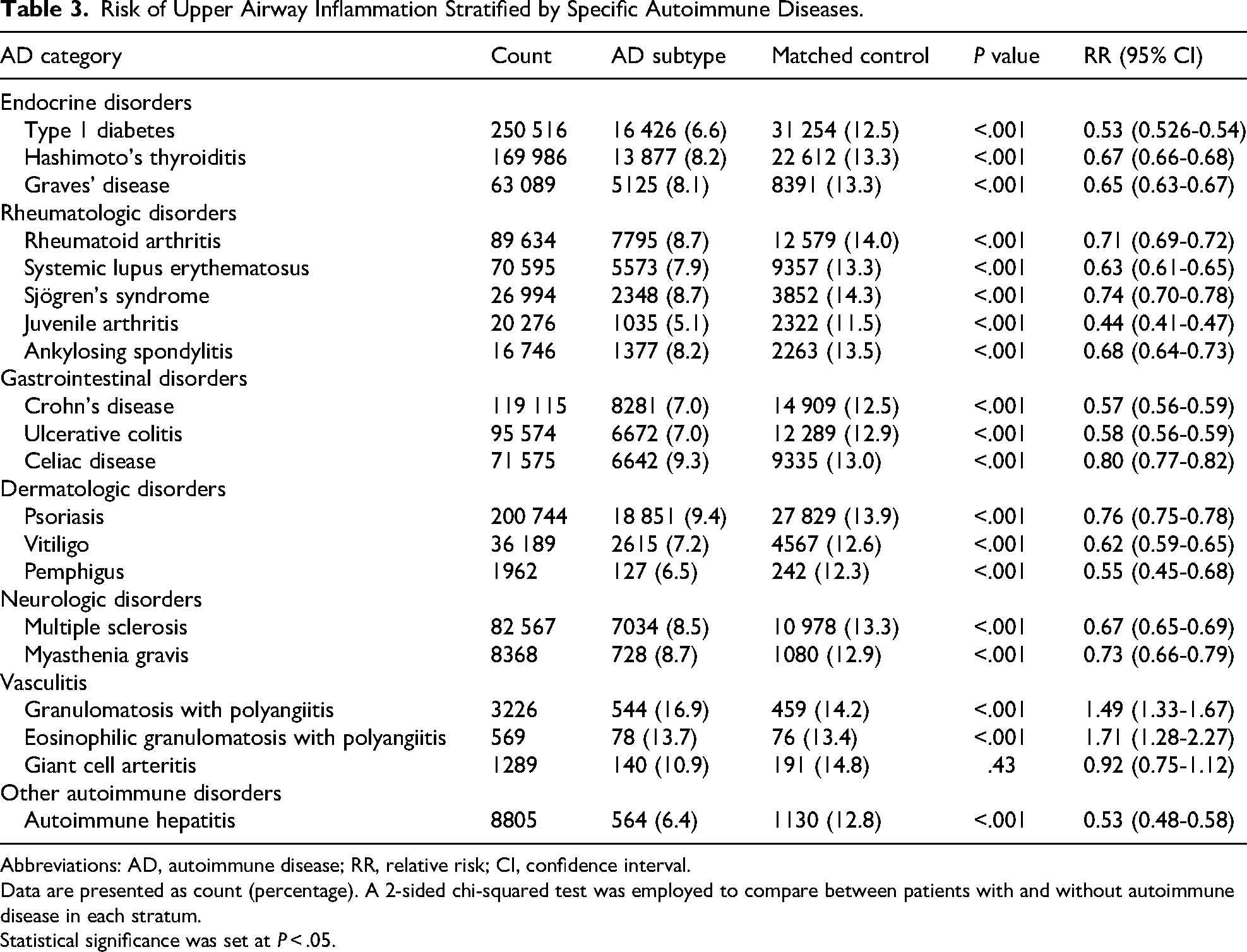
Abbreviations: AD, autoimmune disease; RR, relative risk; CI, confidence interval.
Data are presented as count (percentage). A 2-sided chi-squared test was employed to compare between patients with and without autoimmune disease in each stratum.
Statistical significance was set at P
Discussion
In this real-world cohort study of over 2.6 million patient records worldwide, we found that individuals with ADs were overall less likely to develop at least 1 episode of UAI compared to matched controls. The protective association was strongest for allergic rhinitis (RR 0.64), chronic laryngitis (RR 0.66), and chronic sinusitis (RR 0.88), while the incidence of chronic rhinitis was similar between groups.
Inflammatory processes occurring in the upper airway have substantial societal and clinical relevance. Considering the high prevalence of such diseases in the United States alone, the diagnosis and treatment toward UAI can reach up to $13bn per annum depending on the specific illness, with much more costs related to UAI-related losses in work attendance and productivity.8,9 The symptoms of UAI alone can be bothersome to patients and impair quality of life.10,11 Leaving UAI untreated can gradually involve adjacent tracts and precipitate further medical conditions, such as airway obstruction or bronchial hyperresponsiveness in the lower airway.12,13 With environmental factors being common triggers for patients with autoimmune disadvantage, it is imperative to assess UAI in this susceptible population.14,15
Interestingly, stratified analysis revealed consistent risk reductions of UAI across most autoimmune categories, including endocrine, rheumatologic, gastrointestinal, dermatologic, and neurologic disorders. Notable protective effects were observed in type 1 diabetes mellitus (RR 0.53), a condition affecting almost 9 million individuals worldwide which is the largest population affected out of all diseases studied. 16 Belmonte et al studied the role of insulin treatment in mediating inflammation in the airway which may explain the reduced risk in the disease. 17 Although the exact mechanism is unclear, this may involve controlled glucose levels in preventing the formation of advanced glycation products which are known to induce inflammation and endothelial dysfunction. 18 Regardless, this finding accentuates the additional adverse effects of hyperglycemia and importance of adhering to insulin therapy.
Prior studies echo our findings regarding this protective effect. Sekigawa et al found that there was a significantly lower incidence of atopic disease and UAI in patients with systemic lupus erythematosus than in patients without it, despite a very small cohort size. 19 While celiac disease and psoriasis also exhibited reduced risks of UAI, the magnitude of these associations was limited. This could suggest an underlying genetic overlap or shared inflammatory pathways with allergic diseases, as has been noted in previous studies.20,21 Interestingly, there are also some deviations. Dhamija et al reported that patients with inflammatory bowel disease, including Crohn's disease and ulcerative colitis, were at least 4 times more likely of having CRS than patients without inflammatory bowel disease. 22 Shih et al performed a population-based control study in Taiwan and found that CRS was strongly associated with premorbid ADs. 3 Overall, these deviations may reflect regional variation in allergen exposure or differences in healthcare utilization thresholds that should be investigated further.
Several physiological mechanisms may explain the inverse relationship observed between these ADs and UAI. One explanation involves the Th1/Th2 paradigm, suggesting how the dominance of Th1 helper T cells in ADs can attenuate the response of Th2 helper T cells which mediate inflammatory pathways to environmental triggers.23–25 Furthermore, the chronic immune activation in ADs can gradually lead to immune cell exhaustion which can reduce the responsiveness to inhaled pathogens, a phenomenon more characterized by viral infections but can occur in other contexts as well.26,27 Overall, the observed reductions of UAI, especially allergic rhinitis and chronic sinusitis, suggest immune system alterations that may confer protection against mucosal inflammation.
Corticosteroid use to mediate symptoms from ADs can also prevent severe cases of UAI, although this is not likely the case in this study given that we adjusted for the exposure to systemic corticosteroids during our data analysis. However, AD patients in this study had significantly more sinonasal interventions and intranasal corticosteroid prescriptions when compared to controls. This suggests that if UAI occurs in these patients, it may be corticosteroid-resistant, more severe, or possibly due to atypical inflammatory mechanisms or altered mucosal healing. Unfortunately, we were unable to assess or adjust for biologic medications such as tumor necrosis factor (TNF)-α inhibitors which are used in more advanced cases of ADs and may possibly contribute to new-onset or exacerbated UAI.28,29 This is especially important in the context of CRS as patients taking TNF-α inhibitors may switch from type 1 to type 2 inflammation, the latter being associated with nasal polyps.6,30 Interestingly, it has been shown that the percentage of patients taking such biologics and subsequently seeking care from specialists for UAI is very low, raising the question of if this class of medications will cause UAI to a significantly high extent. 31 Nevertheless, clinicians should evaluate autoimmune context when evaluating UAI symptoms and considering the need to adjust medications to address UAI in addition to the baseline AD symptoms.
Notably, vasculitis disorders such as GPA and eGPA varied from the protective trend and were associated with significantly increased UAI risk. This aligns with known disease presentations as these forms of vasculitis often involve the upper and lower respiratory tracts, causing persistent inflammation and tissue damage.32,33 In contrast, giant cell arteritis did not demonstrate a significant difference which may be due to the limited involvement of the airway mucosa. 34
Recent understanding has revealed patients with immunoglobulin G (IgG4)-related disease (IgG4-RD), a systemic AD due to IgG4-positive plasma cells infiltrating various tissues causing a characteristic fibrosis, to be vulnerable to certain UAI. The discrepancies in the diagnostic criteria of IgG4-RD make the disease difficult to diagnose which precluded us from performing an accurate analysis of this specific AD and including it in the present study.35,36 Previous studies have shown prevalences of allergic rhinitis and CRS ranging from 32% to 54%, with this wide range presumed to be a result of differing diagnostic and inclusion criteria between studies.37–40 However, other studies report low rates of sinusitis in this disease due to limited involvement of the sinuses, though it is being increasingly detected.41,42 Although it is unclear why, UAI in patients with disease tends has shown to be more severe than those without the disease, motivating scientists to consider the presence of IgG4-RD when there is refractory UAI. 43 We recommend a standardized diagnostic approach to detect the presence of IgG4-RD which can facilitate accurate studies on the prevalence, pathophysiology, and management options of UAI in this very unique disease.
Despite these compelling findings, we must acknowledge the study's limitations. First, as a retrospective study using real-world data, diagnostic misclassification and underreporting are possible. Second, medication data and compliance, such as the use of specific disease-modifying drugs or biologic agents, were not analyzed even though they may impact UAI. Third, electronic health record-based research may underdetect mild or subclinical UAI presentations, especially if they are managed in outpatient settings or with over-the-counter therapies.
Conclusions
To our knowledge, this study represents the largest known real-world analysis of UAI outcomes in patients with ADs. Such an investigation is important for evaluating patients with these chronic diseases, optimizing both their patient care and healthcare economics and utilization as a whole. We recommend longitudinal cohort studies to explore the temporal relationship between autoimmune activity, therapy exposure, and UAI occurrence. Mechanistic investigations, such as tissue immunophenotyping and transcriptomic profiling, should also be performed to clarify shared and divergent immune pathways in ADs and UAI.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924251386200 - Supplemental material for Divergent Risk Patterns of Upper Airway Inflammation in Autoimmune Diseases: A Nationwide Retrospective Analysis
Supplemental material, sj-docx-1-ajr-10.1177_19458924251386200 for Divergent Risk Patterns of Upper Airway Inflammation in Autoimmune Diseases: A Nationwide Retrospective Analysis by Jessan A. Jishu, Cameron Galic, Abdelrahman Shata, Gabriel J. Montclare, Hunter Leggett, Reyna Halalsheh, Manal S. Fawzy and Eman A. Toraih in American Journal of Rhinology & Allergy
Footnotes
Acknowledgments
We acknowledge the TriNetX database for providing us with the privilege to access patients’ electronic health records data and promote research to optimize patient care.
Ethical Approval and Informed Consent Statements
Ethical approval was not sought for the present study because all information was collected from a publicly available database which holds de-identified patient information.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Northern Border University, Saudi Arabia, through project number (NBU-CRP-2025-1442).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.