
Abstract
Background
Septoplasty is a common cause of nasal septal perforation (NSP), especially when bilateral apposing septal mucosal tears (BATs) occur intraoperatively. While prior studies have largely focused on NSP management once formed, there is limited evidence on how to prevent NSPs should BATs occur during septal surgery.
Objective
The purpose of this study was to assess the efficacy of intraseptal synthetic interposition graft (SIG) placement to prevent NSPs following BATs during septal surgery.
Methods
A single-institution retrospective cohort study was conducted with adult patients who underwent septoplasty or septorhinoplasty by 2 surgeons. Patients who had BATs intraoperatively had SIGs placed between the septal flaps (cadaveric acellular dermal or porcine collagen grafts). Patients were monitored endoscopically for NSP development at a minimum of 2 months postoperatively.
Results
Of 1132 operative patients between January 2016 and July 2024, 50 patients (4.4%) experienced BATs and had SIGs placed intraoperatively. Of the 50 patients, the median age was 52.7 years, 72.0% were males, and the median follow-up duration was 4.8 months (range: 2.0-85.4). Regarding the SIGs placed, 54.0% were porcine collagen and 46.0% were cadaveric dermis. While 46/50 patients experienced complete mucosalization of their BATs (92.0%), 4 developed NSPs postoperatively (8.0%). Two NSPs occurred within 2 months postoperatively, and 2 were delayed after complete mucosalization. All NSPs occurred following porcine collagen grafts.
Conclusion
Intraseptal synthetic IP graft placement demonstrated 92% success in preventing NSPs following BATs during septal surgery. Future studies should explore the efficacy of different SIGs at preventing NSPs following BATs during septal surgery.
Keywords
Introduction
Septoplasty is a highly effective surgical treatment for alleviating nasal obstruction caused by a deviated nasal septum. 1 Septoplasty is one of the most frequently performed otolaryngologic procedures in the United States, with ∼260 000 being performed annually.2,3 While a nasal septal perforation (NSP) is a relatively rare complication following septoplasty, occurring after about 1.6% to 6.7% of cases,4–6 septoplasty and septorhinoplasty are the most common causes of NSPs overall, representing ≥60% of all NSPs.7–9 NSPs generally occur after septoplasty due to the creation of bilateral apposing septal mucosal tears (BATs) removal of the intervening septal cartilage and bone. While NSPs are often asymptomatic, some patients develop debilitating symptoms like crusting, epistaxis, nasal whistling, and nasal obstruction, and large NSPs can lead to saddle nose deformities.10,11 Additionally, NSP repair following septal surgery is particularly challenging due to intraseptal fibrosis and potential thinning of the septal mucosal flaps.
Due to both the potential for patient morbidity from NSPs and the challenges inherent to NSP repair following septal surgery, it is imperative to prevent NSP formation during nasal septal surgery. First, surgeons aim to preserve the septal mucosal flaps during elevation and avoid apposing bilateral flap tears. This is best achieved through meticulous submucoperichondrial or submucoperiosteal flap elevation, as this preserves maximal flap thickness, blood supply, and biomechanical strength. 12 However, despite best surgical efforts at preventing BATs, they can still occur. When these arise, some surgeons have reported placing autologous tissue grafts to prevent NSP formation.13,14 However, sometimes nasal autologous grafts are not optimal for septal tear geometry, or they may not be available, so extranasal tissue like temporalis fascia may require harvesting. Synthetic collagen and cadaveric dermal grafts are often used to facilitate intranasal mucosal healing in both NSP and cerebrospinal fluid leak repair,15–17 but their use for NSP prevention after septal surgery has been incompletely studied. This study's main purpose was to assess the efficacy of intraseptal placement of synthetic interposition grafts (SIGs) to prevent NSPs following BATs during nasal septal surgery.
Methods
A single-center retrospective cohort study was conducted with adult patients who underwent at least a septoplasty for nasal obstruction by 2 surgeons (RHD and JRC) between January 2016 and July 2024. Institutional Review Board approval was obtained (IRB 10604). Medical charts were reviewed, and patients were included for analysis if they had SIGs placed between BATs that occurred during septoplasty or septorhinoplasty. Patients also had to have been monitored endoscopically for NSP development for a minimum of 2 months postoperatively.
For all patients, the following demographic and clinical data were collected: age, gender, tobacco use status, diabetes mellitus, and autoimmune history [specifically granulomatosis with polyangiitis (GPA) and systemic lupus erythematosus (SLE)]. Regarding surgical details, it was noted whether patients had prior nasal septal surgery, and whether they had concurrent rhinoplasties or inferior turbinate reductions (ITR). Preoperative and postoperative nasal obstruction and septoplasty effectiveness (NOSE, 0-20) scores were also recorded. 18 The primary outcome measures were intraoperative BAT and postoperative NSP development. It was also recorded if purulent septal infections or intranasal synechiae developed at SIG sites.
All surgeries were performed under general anesthesia. Hemitransfixion or Killian incisions were performed based on the location of septal deviation and surgeon preference. Septoplasties were then performed either endonasally or endoscopically, based on surgeon preference, via bilateral submucoperichondrial and submucoperiosteal flap elevation on both sides of the deviated septal cartilage and bone. After removing the deviated portions of septal cartilage and bone, the septal mucosal flaps were examined with a zero-degree rigid nasal endoscope. If BATs were identified, SIGs were placed between the mucosal flap tears, and appropriate SIG positioning was confirmed endoscopically (Figure 1). Based on surgeon preference, SIGs used were either 1.0 mm cadaveric dermal (Alloderm®, LifeCell Corporation, Branchburg, New Jersey) or porcine collagen (Biodesign® Duraplasty or Sinonasal Repair Grafts, Cook Medical, Bloomington, Indiana). Alloderm® grafts are acellular, nonimmunogenic connective tissue matrices with mature elastin, proteoglycans, and collagen bundles derived from allograft skin after epidermal removal. Biodesign® grafts are derived from porcine small intestinal submucosa while retaining the natural composition of extracellular matrix molecules, including collagen, glycosaminoglycans, and growth factors.
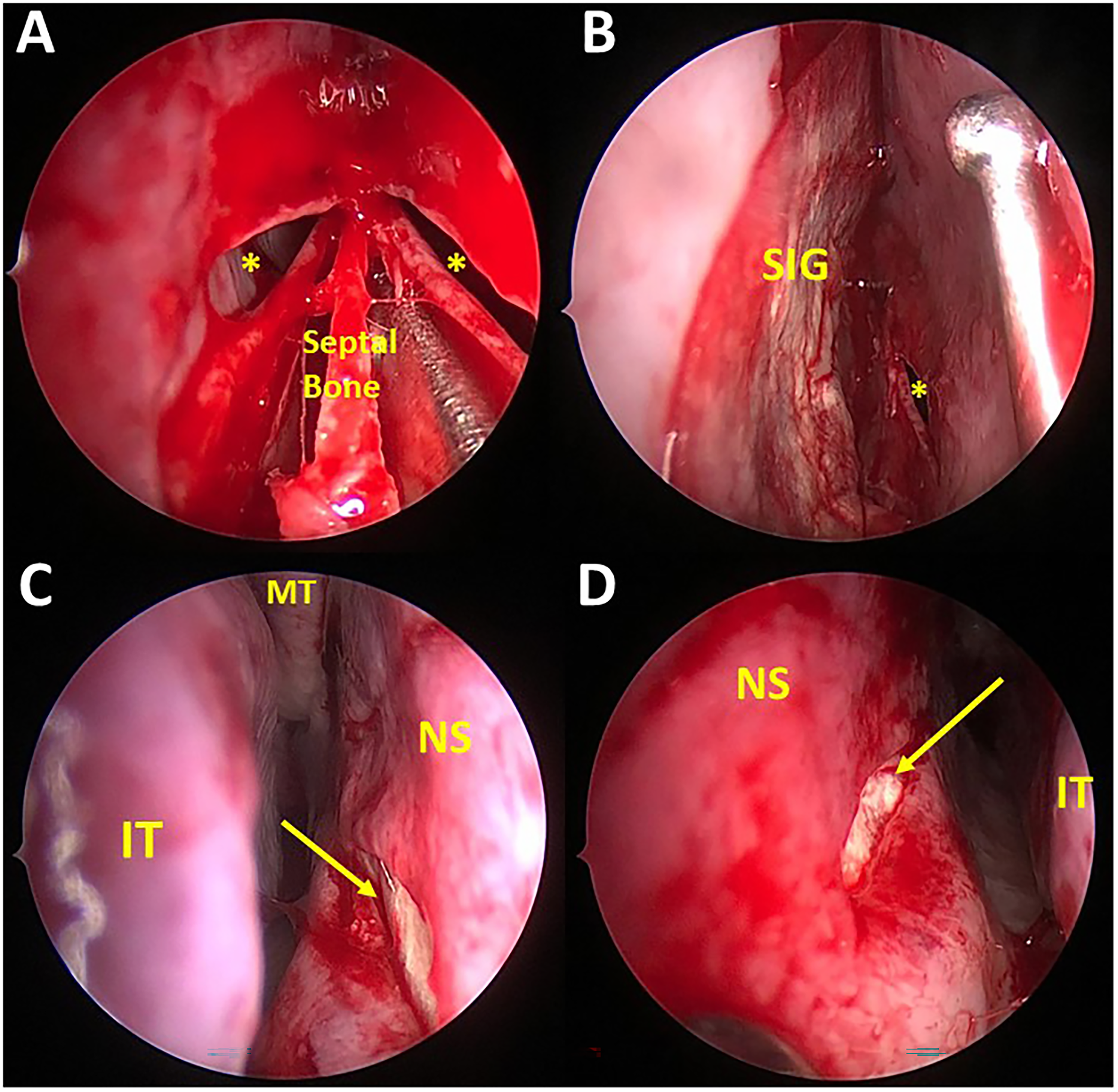
Intraoperative Views of a Representative Case of Bilateral Linear Apposing Septal Mucosal Tears During Septoplasty. (A) Bilateral Mucosal Tears (Yellow Asterisks) Occurred After Removal of Severely Deviated Portions of the Septal Bone. (B) Synthetic Interposition Graft (SIG) Placed Between Right and Left (Yellow Asterisk) Mucosal Tears. (C) SIG Seen Deep to the Right Nasal Septal Tear Defect (Yellow Arrow). (D) SIG Seen Deep to the Left Nasal Septal Tear Defect (Yellow Arrow). Abbreviations: MT, Middle Turbinate; IT, Inferior Turbinate; NS, Nasal Septum.
Initial septal incisions were closed with absorbable sutures. Mucosal flaps above and below the BATs were always pressed and apposed to the underlying SIG on each side. No attempts were made to suture septal mucosal tears or SIGs. Next, Doyle splints were placed bilaterally and secured to the anterior septum with nonabsorbable suture, and were removed about 7 days postoperatively. Patients were administered one dose of intravenous prophylactic antibiotics preoperatively (cefazolin or clindamycin if penicillin-allergic), and prophylactic oral antibiotics after surgery until Doyle splints were removed around one week postoperatively (cephalexin or doxycycline if penicillin-allergic). At each postoperative visit, 0˚ or 30˚ endoscopes were used to visualize the septum in its entirety to evaluate for NSP formation. If BATs were not completely mucosalized at 2 to 3 months postoperatively, patients were always seen again around 6 months postoperatively. If BATs were completely mucosalized at 2 to 3 months, patients were offered another postoperative visit around 6 months, or they could return as needed in the future if they experienced bothersome symptoms. If NSPs developed during follow-up, NSP sizes and locations were recorded. The NSP location was considered anterior if the entirety of the NSP was located anterior to the anterior head of the middle turbinate.
SAS/STAT v9.3 (Cary, NC, USA) was used for statistical analysis. Numerical variables were summarized as medians with interquartile ranges (IQRs), with medians compared via Wilcoxon rank-sum tests. Categorical variables were summarized via frequencies and column percentages and compared via chi-squared tests of independence, except in the presence of sparse data, where Fisher's exact tests were used. NOSE score differences were also calculated from preoperative to the last postoperative visits. All demographic and clinical variables were then compared between patients who did versus did not develop NSPs postoperatively using the Wilcoxon rank-sum tests.
Results
Table 1 shows demographic and clinical data. Of 1132 patients who had at least septoplasties, 50 developed BATs requiring intraseptal SIG placement (4.4%). Of the 50 patients with SIG placement, the median age was 52.7 years, and 72% were male. Additionally, 16% were current smokers, 26% were former smokers, 10% had diabetes mellitus, and no patients had GPA or SLE. Only 2 patients had undergone a prior septal surgery. Regarding concurrent surgical interventions, 94% had ITRs, and 20% had septorhinoplasties (all via a closed approach by one surgeon, RHD). Of the 50 SIGs, 27 (54%) were porcine collagen xenografts (22 duraplasty and 5 sinonasal grafts), and 23 (46%) were cadaveric acellular dermal grafts. Patients were followed postoperatively for a median of 4.8 months (IQR = 2.5-13.7; range = 2.0-85.4), with 23/50 (46%) having been followed for ≥ 6 months, and 14/50 (28%) for ≥ 12 months.
Demographic and Clinical Data of Patients Who Had Synthetic Interposition Grafts Placed for Bilateral Apposing Septal Mucosal Tears During Septal Surgery.
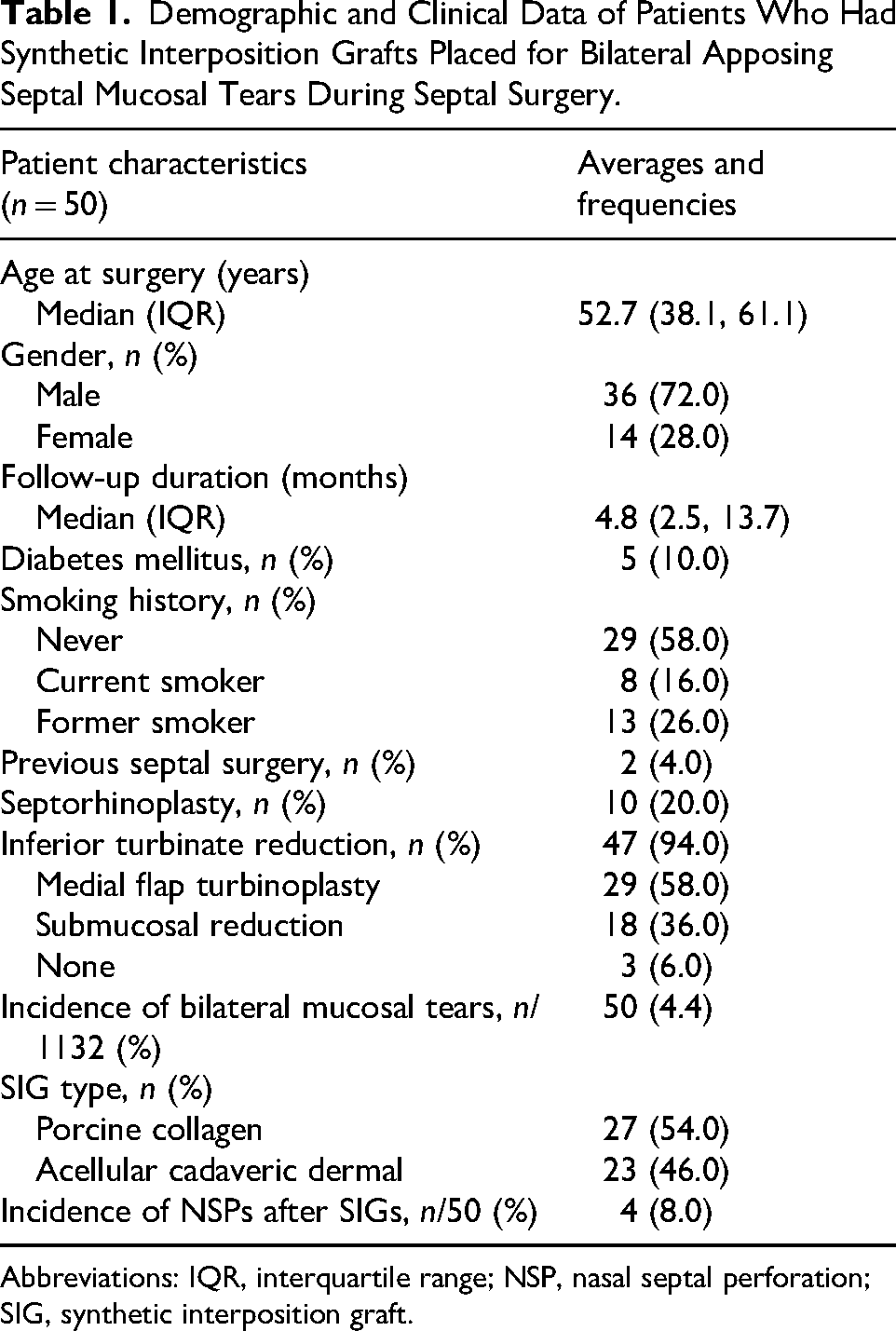
Abbreviations: IQR, interquartile range; NSP, nasal septal perforation; SIG, synthetic interposition graft.
Regarding outcomes, 4/50 patients (8%) developed NSPs despite intraseptal SIG placement for tears. Figure 2 shows a representative example of successful postoperative healing in the case from Figure 1, as occurred in 92% of cases. None of the patients had purulent septal infections at the SIG sites, and no synechiae formed between the SIG sites and surrounding intranasal structures. Table 2 shows the clinical features compared between those who did versus did not develop NSPs postoperatively. None of the variables were significantly different between groups. Overall, patients achieved a significant median 9-point NOSE score reduction following functional nasal surgery (P ≤ .0001), having decreased from a median NOSE score of 15.0 preoperatively to 3.0 postoperatively. While NSP patients achieved a 14-point NOSE score reduction compared to a 9-point reduction in those without an NSP, these NOSE score reductions were not significantly different (P = .137).

Postoperative Endonasal Views Over Time in the Case From Figure 1. (A and B) Right and Left Nasal Endoscopic Views at 1 Week Postoperatively, Showing That the Bilateral Tears Had Not Mucosalized Yet (Yellow Arrows). On the Left Side (B), a Blood Clot Was Overlying the Synthetic Interposition Graft. (C and D) Right and Left Nasal Endoscopic Views at 3 Months Postoperatively, Showing That Both Tears Had Mucosalized Completely Without Nasal Septal Perforation Development (Yellow Arrows). On the left (D), There Was a Linear Depression Where the Defect Closed Over the Interposition Graft. Abbreviations: IT, Inferior Turbinate; NS, Nasal Septum.
Comparison of Demographic and Clinical Data Between Patients Who Did Versus Did Not Develop NSPs. There Were No Significant Differences Between the Groups for any of the Variables.
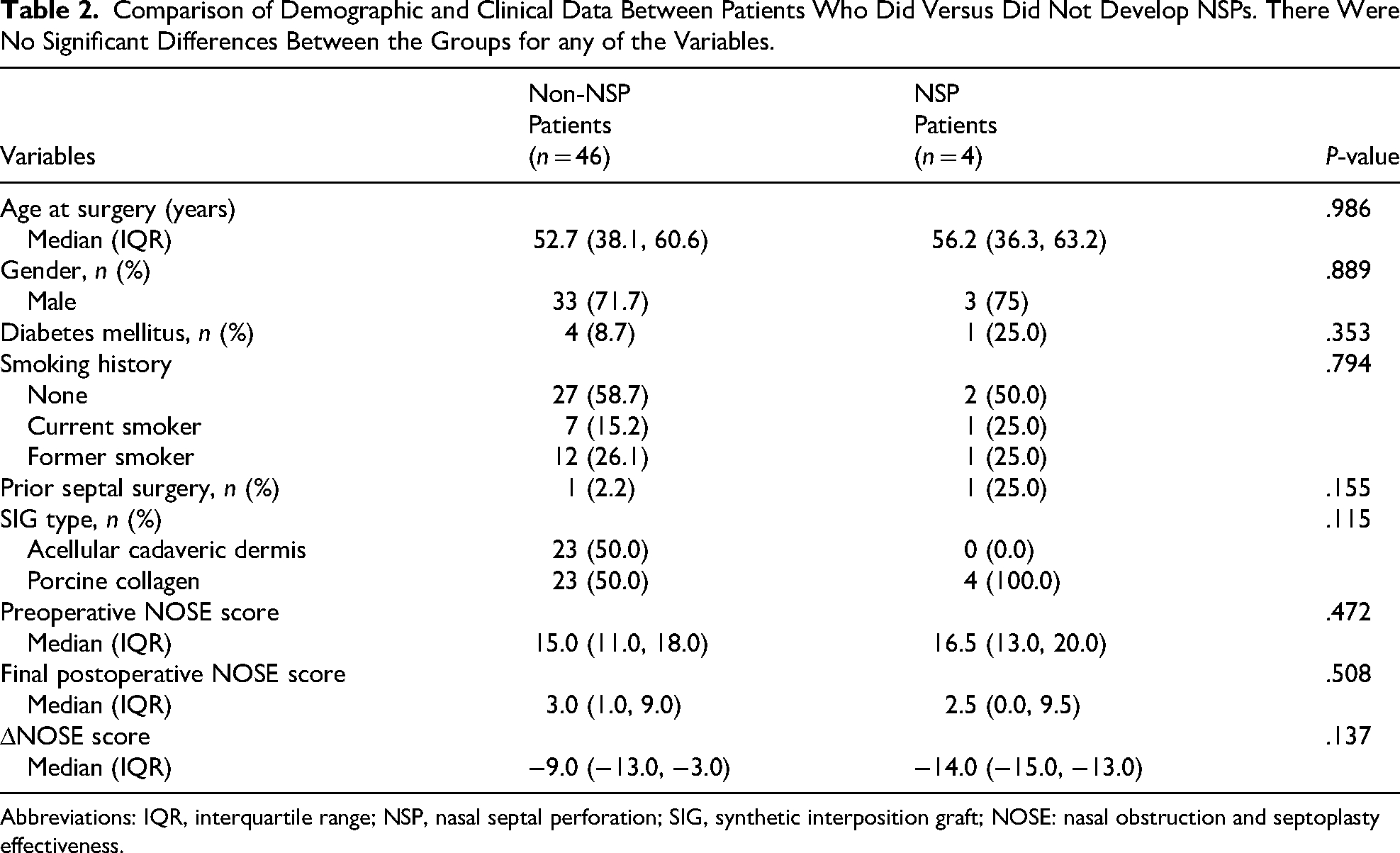
Abbreviations: IQR, interquartile range; NSP, nasal septal perforation; SIG, synthetic interposition graft; NOSE: nasal obstruction and septoplasty effectiveness.
Table 3 demonstrates the clinical features in the 4 patients who developed NSPs postoperatively. All 4 patients had porcine collagen xenografts placed. Patients 1 and 4 had Biodesign® Duraplasty grafts, and patients 2 to 3 had Biodesign® Sinonasal grafts. Only patient 4 had diabetes mellitus. Note that patients 1 and 2 developed early NSPs within the first 2 months of surgery, while patients 3 and 4 developed delayed NSPs detected years after surgery, despite no septal perforation being seen at earlier postoperative visits. Of the 4 patients, only patient 1 was symptomatic with nasal whistling and wished to undergo NSP repair. She underwent successful NSP closure with a unilateral anterior ethmoid artery flap without SIG placement. Patients 2 to 4 were not interested in NSP repair as their symptoms were minimal to none. Of note, each surgeon had 2 patients develop NSPs, with one being early and one delayed for each surgeon (JRC: patients 1 and 4; RHD: patients 2 and 3).
Clinical Features of the 4 Patients Who Developed NSPs After Porcine Collagen Graft Placement for Bilateral Apposing Septal Mucosal Tears.
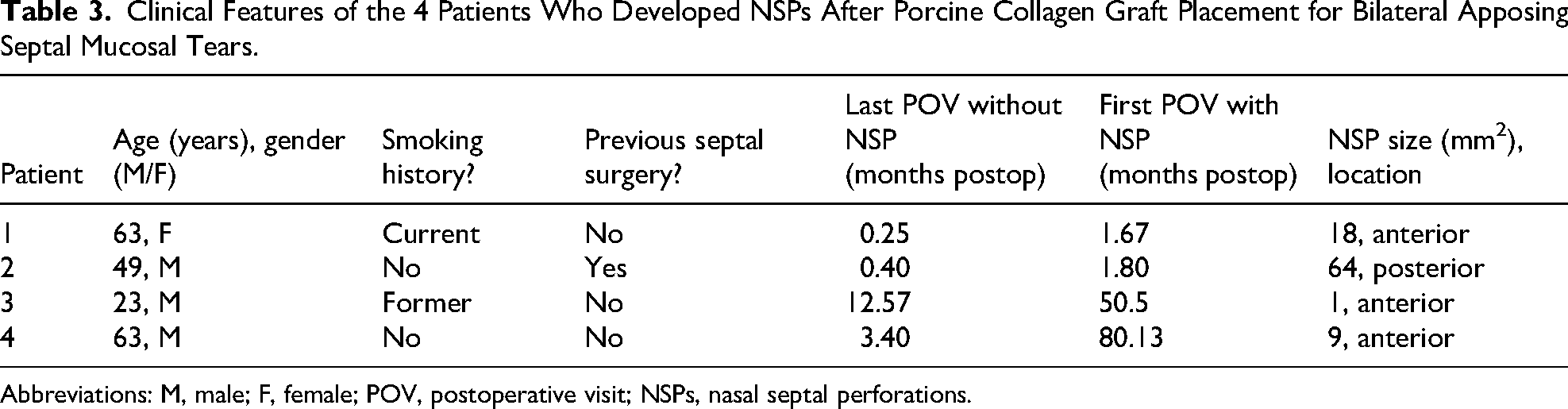
Abbreviations: M, male; F, female; POV, postoperative visit; NSPs, nasal septal perforations.
Figure 3 shows the representative images of a patient who developed an early NSP following SIG placement. Note that the SIG had shifted and extruded through the mucosal tear edges at the first postoperative visit, and despite attempts at SIG repositioning, an NSP subsequently formed. Figure 4 shows the intraoperative images of a patient with large apposing septal tears and SIG placement, and Figure 5 shows the healing of the case at 3 months and 6.5 years postoperatively. The patient developed an asymptomatic small anterior NSP that developed at some point after endoscopic confirmation of complete septal mucosalization 3 months postoperatively.
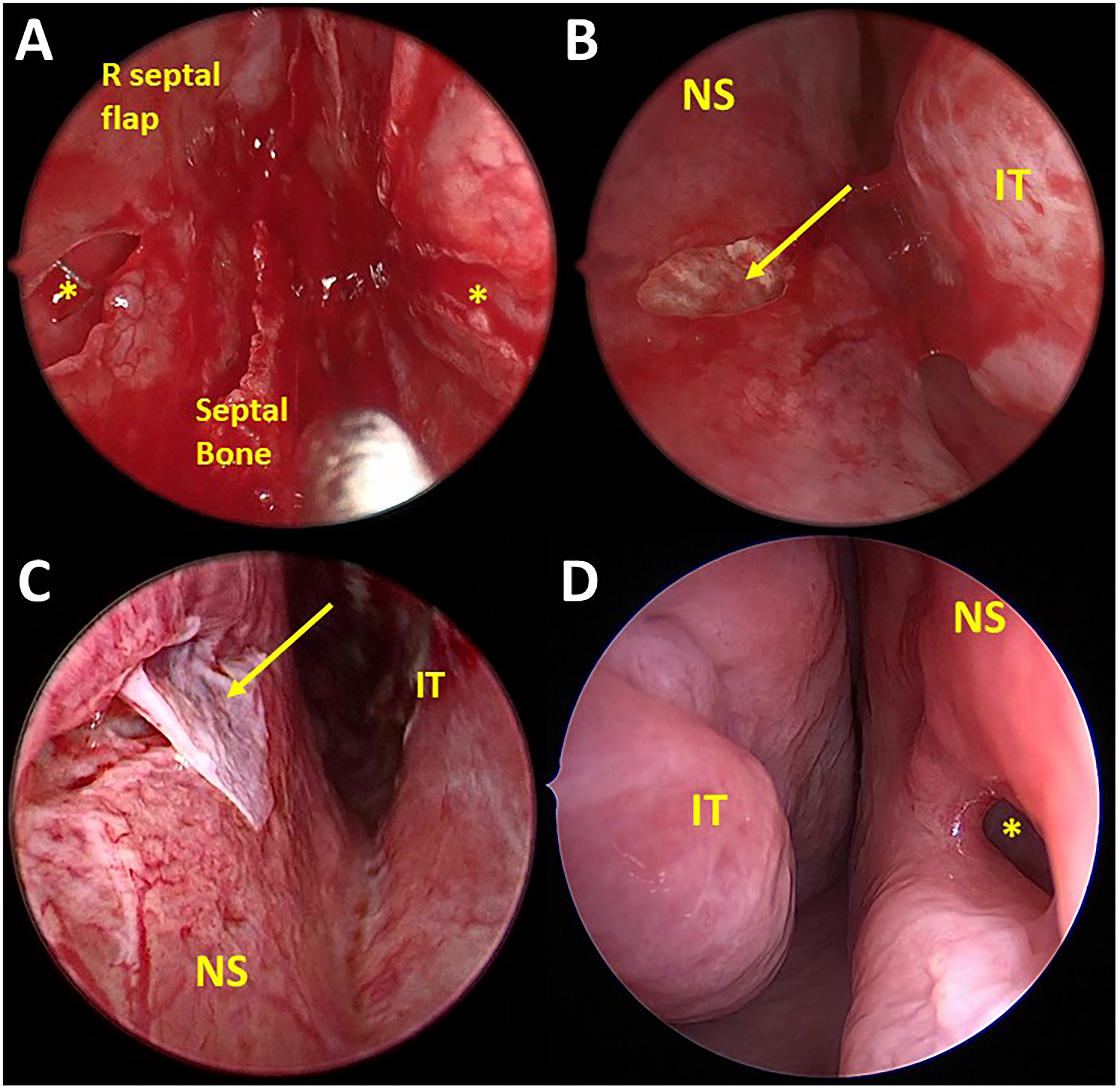
Case Example of Bilateral Apposing Septal Mucosal Tears (BATs) Intraoperatively That Failed to Heal With Porcine Collagen Interposition Graft. (A) Endoscopic View Between the 2 Septal Flaps During Septoplasty, Showing BATs (Yellow Asterisks) on Either Side of the Deviated Septal Bone That Had Been Resected. (B) Left-Sided Nasal Endoscopic View Showing the Collagen Graft in Optimal Position Deep to the Left Septal Mucosal Tear Defect (Yellow Arrow). (C) Left-Sided Endoscopic View 1 Week Postoperatively, Where the Collagen Graft Was Noted to Have Extruded Through the Tear Defect's Inferior Edge. The Graft Was Tucked Back Under the Mucosal Tear's inferior Edge but Did Not Seat Perfectly. (D) The Collagen Graft Failed, and a 6 × 3 mm2 Anterior Nasal Septal Perforation Formed, Which Caused Nasal Whistling and Required Endoscopic Repair. Abbreviations: IT, Inferior Turbinate; NS, Nasal Septum.
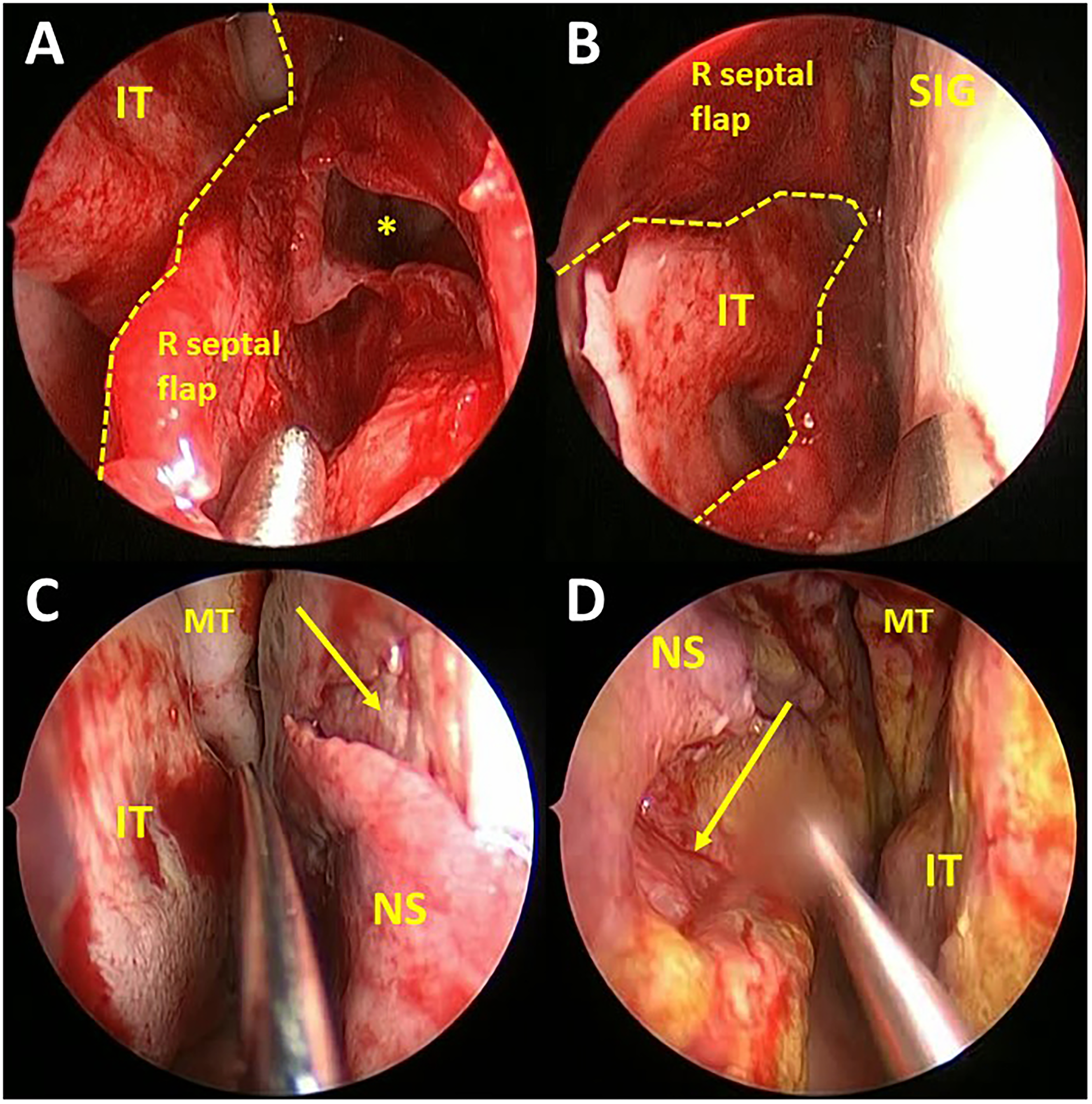
Intraoperative Endoscopic Views of Large Bilateral Apposing Septal Mucosal Tears (BATs) During Septoplasty. (A) Endoscopic View Between Mucosal Flaps Showing a Large Nonlinear Tear Defect on the Right (Border With Yellow Dotted Line). (B) Synthetic Interposition Graft (SIG) Placement Between the Septal Mucosal Flaps and Tears, With the Right Flap Tear Again Outline by a Yellow Dotted Line. (C) Right Nasal Endoscopic View Showing the SIG Appropriately Deep to the Right Septal Flap Defect Edges (Yellow Arrow). (D) Left Nasal Endoscopic View Showing the SIG Deep to the Left Septal Flap Defect Edges (Yellow Arrow). Abbreviations: MT, Middle Turbinate; IT, Inferior Turbinate; NS, Nasal Septum.
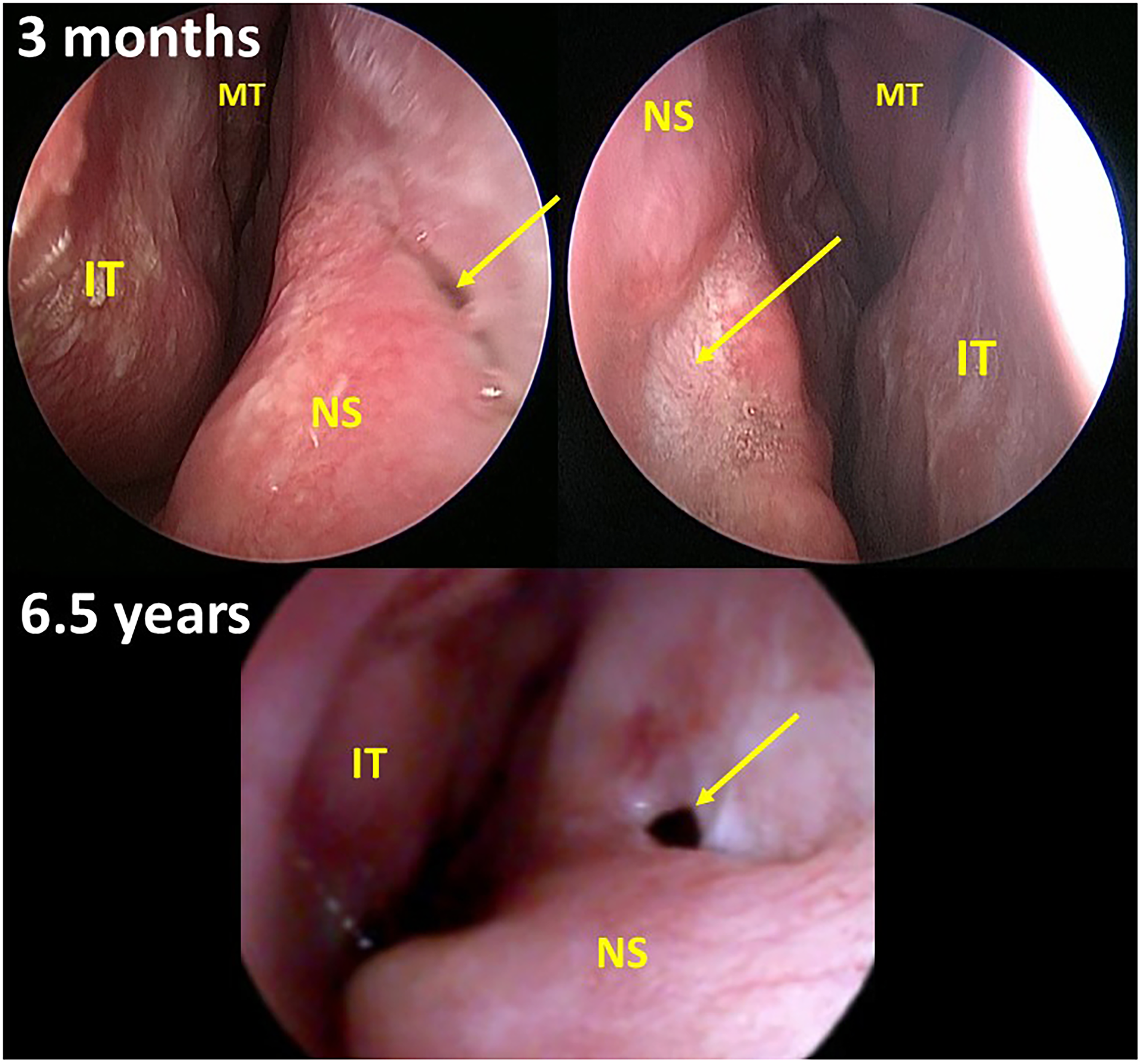
Postoperative Healing of the Case From Figure 4 at 3 Months and 6.5 Years Postoperatively. The Patient Developed an Asymptomatic Small Anterior NSP that Developed at Some Point After Endoscopic Confirmation of Complete Septal Mucosalization 3 Months Postoperatively. At 3 Months, the Arrows Show the Area of Synthetic Interposition Grafting Between the Septal Tears. On the Right Septum, There Was a Linear Depression With Potentially Incomplete Mucosalization (Blue Arrow), but on the Left Nasal Side, There Was Complete Mucosalization Without Perforation (Yellow Arrow). At 6.5 Years, a Perforation Was Noted (Yellow Arrow). Abbreviations: MT, Middle Turbinate; IT, Inferior Turbinate; NS, Nasal Septum.
Discussion
Septoplasty is highly effective at resolving nasal obstruction due to a deviated nasal septum, and complication rates are low. Among complications, however, NSPs arise in a minority of cases. While NSPs can occur with unilateral or even no septal tears during septal surgery, generally they develop in the setting of BATs, especially if left untreated.11,14,19 Rates of intraoperative BATs have only been reported in a few studies, and range from 5.5% to 11.9%.13,19,20 The current study showed a 4.4% rate of BATs during septal surgery (50/1132). Of these 50 patients, intraseptal SIG placement prevented NSP formation in 92% of cases. It is helpful for surgeons to know that SIG placement for BATs will generally be successful for preventing NSPs, because this is a low-morbidity option for preventing potentially highly morbid NSPs.
NSP prevention is critical because while many authors have reported 60% of NSPs to be asymptomatic, a significant proportion of these patients are symptomatic and require treatment. While some patients can achieve symptomatic relief through topical moisturization with or without a synthetic implant like a septal button, others will warrant surgical intervention. NSP surgical repair is known to be particularly challenging, especially when the etiology is prior septal surgery, so NSP prevention during the initial septoplasty is key.
Avoiding the potential perils of NSP repair following septal surgery begins with optimal surgical technique. With meticulous technique during septal surgery, submucoperichondrial and submucoperiosteal planes can usually be elevated on both sides of the septal bone and cartilage without creating BATs. Flap elevation is optimized with appropriate instrumentation and hemostasis. Maintaining a maximal amount of perichondrium and periosteum with the mucosal flaps ensures the greatest blood supply and mechanical strength, 12 which lessens the risk of NSP. However, despite best efforts, mucosal tears may occur on one or both sides. If one tear occurs, surgeons must take extra care to isolate the tear to prevent enlargement and avoid contralateral tearing, which should mitigate the risk of NSP formation.
When bilateral tears do occur, surgeons should consider some form of interposition grafting to prevent an otherwise likely NSP, and possibly suture closure of one or both BATs. Unfortunately, very few studies have reported success rates of interposition grafts for NSP prevention following BATs during septal surgery. Eren et al 19 reported BATs in 17/143 septoplasties. They sutured closed at least one side of the septal mucosa and placed either cartilage or bone fragments as interposition grafts, and used silicone splints in 78% of cases. One patient developed an NSP (5.9%). Lee et al 13 reported BATs in 34/463 septoplasties, and placed either autologous cartilage alone (n = 23) or cartilage plus fibrin glue applied to mucosal tears (n = 11), plus 4 weeks of silastic sheets. They showed NSP formation in 34.8% of patients who had cartilage interposition grafts alone versus 9.1% of those who also had fibrin glue, though the difference was not statistically significant. Park et al demonstrated a postoperative NSP rate of 5.7% with TnR Nasal Mesh (3D-fabricated polycaprolactone mesh) compared to 54.5% with septal cartilage interposition graft alone. 20 While no studies have specifically studied the use of Biodesign® or Alloderm® for BATs during septal surgery, a recent 12-patient case series showed 100% success with porcine collagen-only repair of true NSPs of maximal diameters 5 to 20 mm. 15 Additionally, Kridel et al 16 (n = 12) and Sharma et al 21 (n = 13) both showed acellular dermal grafts alone to repair NSPs of diameters 2 to 45 mm to be successful in 91.5% and 69.2% of cases, respectively. While these SIG-only NSP repair studies each had small sample sizes, they show that porcine collagen and acellular dermal grafting alone can be successful for closure of small and large NSPs. Compared to mature NSP defects, BAT defects are generally more linear with vascularized wound edges, so it makes sense that SIGs were highly successful in the present study at preventing NSP development. However, a future study could also assess the success of BAT suturing alone without interposition grafting for preventing NSP formation.
SIGs have multiple benefits compared to autologous materials. While autologous cartilage and bone grafts may be readily available at no added cost to patients, they have demonstrated variable success at preventing NSPs following BATs, and they may require extranasal tissue harvest. SIGs may be more expensive (porcine collagen grafts about $285-$395 USD, and acellular dermal grafts about $443.00 USD), but they avoid other donor site morbidity, are relatively inert, and have been shown to promote wound healing in various body tissues, including the nasal septum.15,16,21 The present study reinforced these previous reports in that no patients developed hypersensitivity reactions or septal infections, and generally led to successful mucosalization.
Regarding the SIG type to use with BATs, the present study showed no statistically significant differences in NSP development between porcine collagen and acellular dermal grafts. However, the small sample sizes of BATs and NSPs prevented robust analysis. While all 4 NSPs formed following porcine collagen grafts, it is important to note that 2/4 patients developed delayed NSPs following successful mucosalization postoperatively. Furthermore, 2 different Biodesign® grafts were used, and both graft types were associated with early and delayed NSPs in different patients. Due to the rarity of NSPs and variable porcine collagen graft types used, no definitive conclusions can be drawn with regard to the efficacy of Alloderm® versus Biodesign® grafts for NSP prevention after BATs. This should be explored in future studies to determine the most optimal and cost-effective SIG to promote nasal septal mucosalization, including comparisons of times to mucosalization between different SIGs.
There were also several limitations with this study. First, this was a single-center retrospective study with 50 patients. While small overall, this sample size was similar to or larger than previous studies with similar objectives,13,20 highlighting how rare BATs are when surgery is performed meticulously. However, larger multicenter studies would be ideal for generating greater generalizability, and the prospective collection of all variables pertinent to risks of NSP development would be optimal. Additionally, it would be helpful to compare a larger sample of post-septoplasty patients with NSPs to patients without NSPs to determine whether these patients differ with regard to subjective nasal obstruction outcomes since NSP patients in this study experienced greater NOSE score reductions (albeit non-significantly). Also notable, long-term follow-up was lacking, with only about 50% of patients having >6 months of follow-up, and 28% having >12 months of follow-up. Some patients could have developed delayed NSPs outside of 6-12 months that would have been missed. Another limitation was the lack of details on the sizes, shapes, degree of overlap, and locations of the mucosal tears. Most of the tears in cases from this study were linear, but some were larger nonlinear defects, and they likely overlapped to varying degrees. As these details were not consistently recorded, one cannot determine whether certain septal mucosal defect sizes, shapes, and degrees of overlap lend themselves to more successful mucosalization after SIG placement. Lastly, anterior tears may be more likely to promote eschar formation through desiccation and subsequent picking, which could affect the SIG success and NSP formation. Future studies should note the geometry and locations of septal mucosal tears when assessing SIG success.
Conclusion
BATs occurred rarely in 4.4% of septoplasties. Intraseptal SIG placement prevented NSP development after BATs in 92% of patients. Future studies should explore the efficacy of different SIGs, autologous grafts, and suturing alone in preventing NSPs following BATs during septal surgery.
Footnotes
Acknowledgments
The authors would like to acknowledge Natalie Craig, graphic designer, for her assistance in formatting the digital images used as figures in this article.
Ethical Considerations
Institutional Review Board approval was obtained from the Henry Ford IRB Committee – IRB Approval Number 10604.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr John Craig is a research consultant for Aerin Medical, Inc.
Data Availability Statement
The research data associated with the paper is available to share upon request.