
Abstract
Background
Ultra-processed foods (UPF) are industrial formulations derived mostly from substances refined or extracted from foods. UPF intake has been linked to obesity, cardiovascular disease, and adult mortality, with recent studies demonstrating possible associations with asthma and allergy.
Objective
We investigate the association of UPF intake with self-reported sinusitis and other sinonasal symptoms.
Methods
We retrospectively reviewed 3 cycles of the National Health and Nutrition Examination Survey (NHANES), ranging from 2005 to 2014, which includes dietary and sinonasal symptom data on a large, representative sample of the US population. Individuals were divided into quartiles based on the percent of daily caloric intake consisting of Nova category 4 UPF. Multivariable logistic regression was performed to assess the association of UPF intake with sinonasal symptoms, adjusting for demographic data and medical comorbidities.
Results
And 10,068 individuals (mean age 54.2 years, 52.1% female) were studied. Compared to the lowest quartile of UPF intake, the highest quartile had a higher rate of asthma (16% vs 11%, P = .03), obesity (40% vs 30%, P < .001), smoking (51.6% vs 44.4%, P < .001), emphysema (2.9% vs 1.8%, P = .02), and food insecurity (26% vs 21%, P = .002). On multivariable regression, the highest quartile of UPF intake was associated with self-reported sinusitis (odds ratio [OR] = 1.54, 95% confidence interval [CI] 1.15-2.05, P = .007). UPF intake was also associated with xerostomia-related dysgeusia (OR 1.79, CI 1.15-2.80, P = .02) but not with other sinonasal symptoms, including hyposmia, allergies, hay fever, or nasal congestion from allergies.
Conclusion
UPF intake is significantly associated with self-reported sinusitis and xerostomia-related dysgeusia, although not with other sinonasal symptoms. Further studies are needed to elucidate the mechanism of this association.
Keywords
Introduction
Ultra-processed foods (UPF) are industrial formulations derived mostly from substances refined or extracted from foods. Unlike processed foods, which are whole foods preserved by canning, pickling, or other techniques, UPF contain little to no whole foods. These products are inexpensive, easily accessible, and require little to no cooking. Their share in the Western diet has increased significantly in the past several decades, and UPF now provide the majority of energy in the US adult diet. 1 Recent studies have linked UPF intake to unbalanced nutritional profile, obesity among adults and adolescents and poor cardiovascular health, possibly through mechanisms affecting oxidative stress, insulin resistance, and satiety.2,3
UPF have also been associated with asthma, allergies, pro-inflammatory states, and immune dysregulation.4-6 Many mechanisms have been proposed for this immune dysregulation, with several human observational and controlled feeding studies suggesting diet can alter T-cell populations and immune signatures in blood samples, as well as modify the gut microbiota.7-9 However, no studies have assessed the association of UPF intake with sinusitis, which has significant overlap with asthma, allergies, and inflammation. 10 Prior literature has suggested that the Mediterranean diet can serve as a modifiable risk factor in pediatric recurrent acute rhinosinusitis (RARS). 11 This study found that in the pediatric population, the number of acute rhinosinusitis episodes per year decreased from 3.4 episodes at baseline to 0.3 episodes at 1 year after switching to a traditional Mediterranean diet, with more than half of patients not having a single episode. The same group found that the Mediterranean diet also constitutes a modifiable risk factor for otitis media with effusion and nasal obstruction. 12 However, these reports do not evaluate the role of UPF in these otolaryngological conditions and are limited by their focus on the pediatric population as well as the lack of a control group.
In this report, we aim to investigate the association of UPF intake with self-reported sinusitis and sinonasal symptoms.
Methods
This study was exempt from review by our organization's Institutional Review Board because it was conducted using publicly available, de-identified data. Data were retrospectively reviewed from National Health and Nutrition Examination Survey (NHANES), which contains dietary and health data on a large, representative sample of the noninstitutionalized US population. Organized by the National Center for Health Statistics, NHANES is administered via computer-assisted personal interviewing completed by a team of physicians, medical technicians, and health interviewers. Respondents undergo in-person household interview and then physical examination and other testing at a mobile examination center. A stratified, multistage probability cluster design is employed at multiple levels, including county, block, household, and individual. Data were obtained from the 2005-2006, 2011-2012, and 2013-2014 cycles of NHANES, which are the only available NHANES cycles that queried participants on sinonasal symptoms. Survey weights were applied per guidelines provided in NHANES documentation to ensure a representative sample.
Dietary recall was obtained from 2 nonconsecutive interviews, in which participants were asked to recall their dietary history over the immediately preceding 24h periods. Foods were categorized based on level of processing in accordance with the Nova food classification, as described elsewhere. 13 Briefly, category 1 describes minimally processed foods such as fresh fruits and vegetables, category 2 includes processed culinary ingredients (eg, salt and olive oil), category 3 comprises food made from combining processed ingredients and unprocessed or minimally processed food (eg, canned vegetables and smoked meat), and category 4 includes UPF that have undergone extensive extraction and chemical modification (eg, cereal, soft drinks, packaged snacks, and fast food). Individuals were divided into quartiles based on the percent of their daily caloric intake consisting of Nova category 4 UPF, averaged over both 24h periods.
Prior to 2011, presence of sinusitis was queried by asking if a “doctor has told you that you have a sinus infection within the last 12 months”. From 2011 onward, patients were asked if they “ever had 2 or more sinus infections.” For allergies and hay fever, respondents were asked if a doctor told them they had these conditions in the past 12 months. For all other assessed symptoms, including dysgeusia, hyposmia, and nasal congestion from allergies, respondents were asked to report if they had these symptoms over the past 12 months. In addition, NHANES does report objective olfactory data. However, this is available for solely for the 2013 to 2014 cycle, with approximately 20% of patients in this cycle undergoing smell testing. Therefore, these data were not included.
All analyses were performed using R version 4.0.5 (R Project for Statistical Computing). Descriptive statistics were applied to report characteristics of the study cohort by quartile of UPF intake. Categorical and continuous variables were compared by the χ2 test of independence and one-way analysis of variance, respectively. All analyses included survey weights supplied by the National Center for Health Statistics to account for sampling bias.
Multivariable logistic regression was performed to assess the association of UPF intake with sinonasal symptoms, adjusting for the following demographic data and medical comorbidities: age, sex, race/ethnicity, education level, income poverty ratio, asthma, overweight status, smoking history, emphysema, and chronic bronchitis. Smoking history was queried by asking respondents if they had smoked at least 100 cigaretes during their lifetime. Education level was defined as parental education level for respondents aged 20 years or younger. A P-value of .05 was defined as the limit of statistical significance.
Results
After excluding patients without dietary recall or sinusitis symptom data, 10,068 individuals (mean age 54.2 years, 52.1% female) were included (Table 1). The prevalence of self-reported sinusitis was 19.7%. In the lowest quartile of UPF intake, respondents had an average of 29.8% of daily calories derived from UPF, with a range of 0% to 40%. In contrast, the highest quartile of UPF intake displayed an average of 74.4% of daily calories derived from UPF, with a range of 64.8% to 100%. Compared to the lowest quartile of UPF intake, the highest quartile had a higher rate of asthma (16% vs 11%, P = .03), overweight status (40% vs 30%, P < .001), smoking (51.6% vs 44.4%, P < .001), and emphysema (2.9% vs 1.8%, P = .02) and food insecurity (26% vs 21%, P = .002).
Cohort Characteristics.
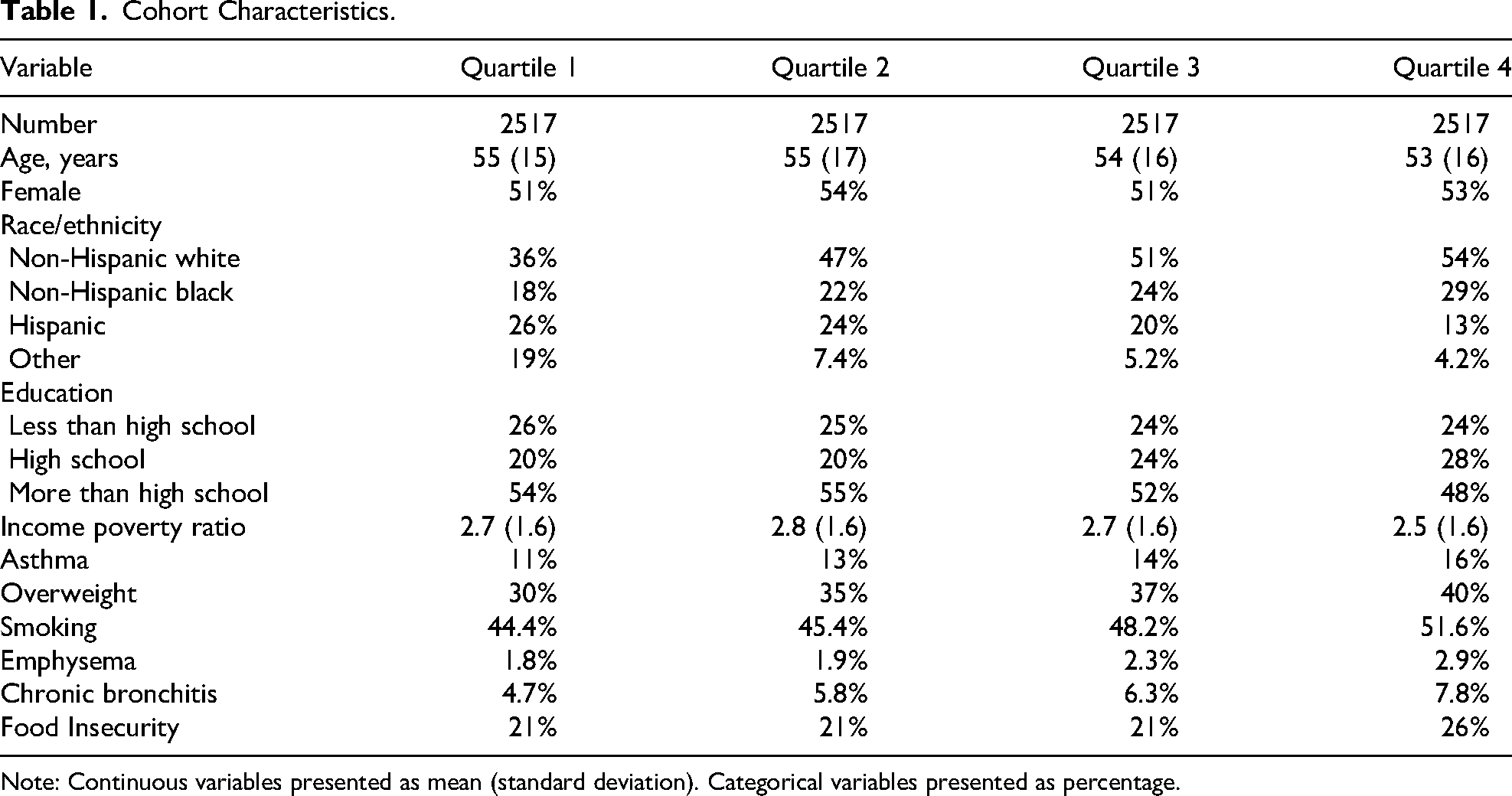
Note: Continuous variables presented as mean (standard deviation). Categorical variables presented as percentage.
On multivariable regression, respondents in the highest quartile of UPF intake displayed higher odds of self-reported sinusitis (odds ratio [OR] 1.54, 95% confidence interval [CI] 1.15-2.05, P = .007, Table 2) and dysgeusia (OR 1.79, CI 1.15-2.80, P = .02, Table 3) compared to the lowest quartile. UPF intake is associated with xerostomia (OR 2.26, CI 1.68, 3.02, P < .001); when adjusted for xerostomia, UPF intake no longer was associated with dysgeusia at a significant level (OR 1.62, CI 1.00-2.62, P = .07). UPF intake was not associated with hyposmia (OR 1.16, CI 0.78-1.74, P = .48), nasal congestion from allergies (OR 1.28, CI 0.97-1.68, P = .10), allergies (OR 1.02, CI 0.77-1.34, P = 0.88), or hay fever (OR 0.93, CI 0.58-1.50, P = .79). UPF intake was not correlated with serum total IgE levels as measured by Pearson correlation coefficient (r = −0.02, P = .17).
Association of UPF Intake With Self-Reported Sinusitis.
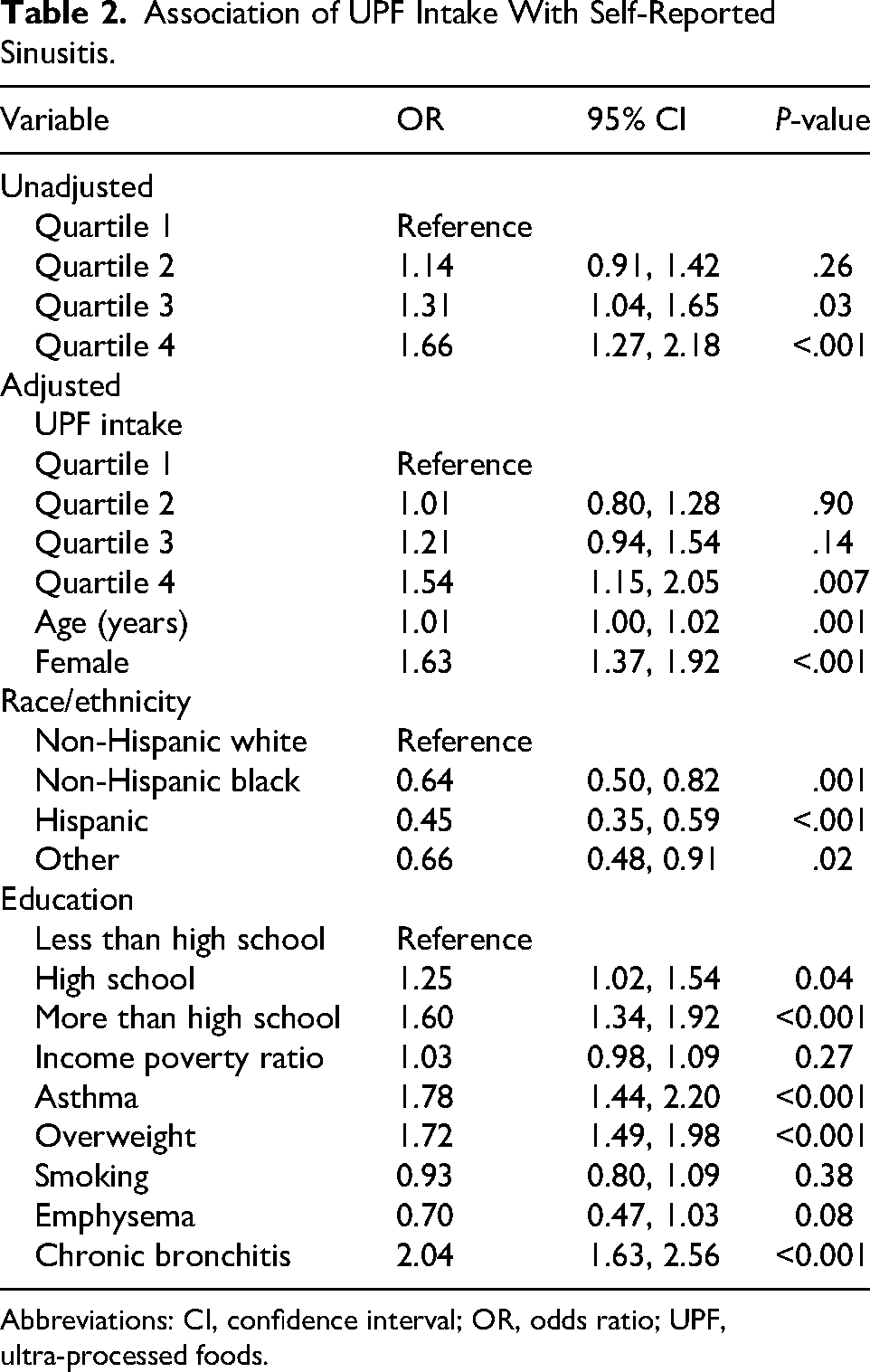
Abbreviations: CI, confidence interval; OR, odds ratio; UPF, ultra-processed foods.
Association of UPF Intake With Dysgeusia.
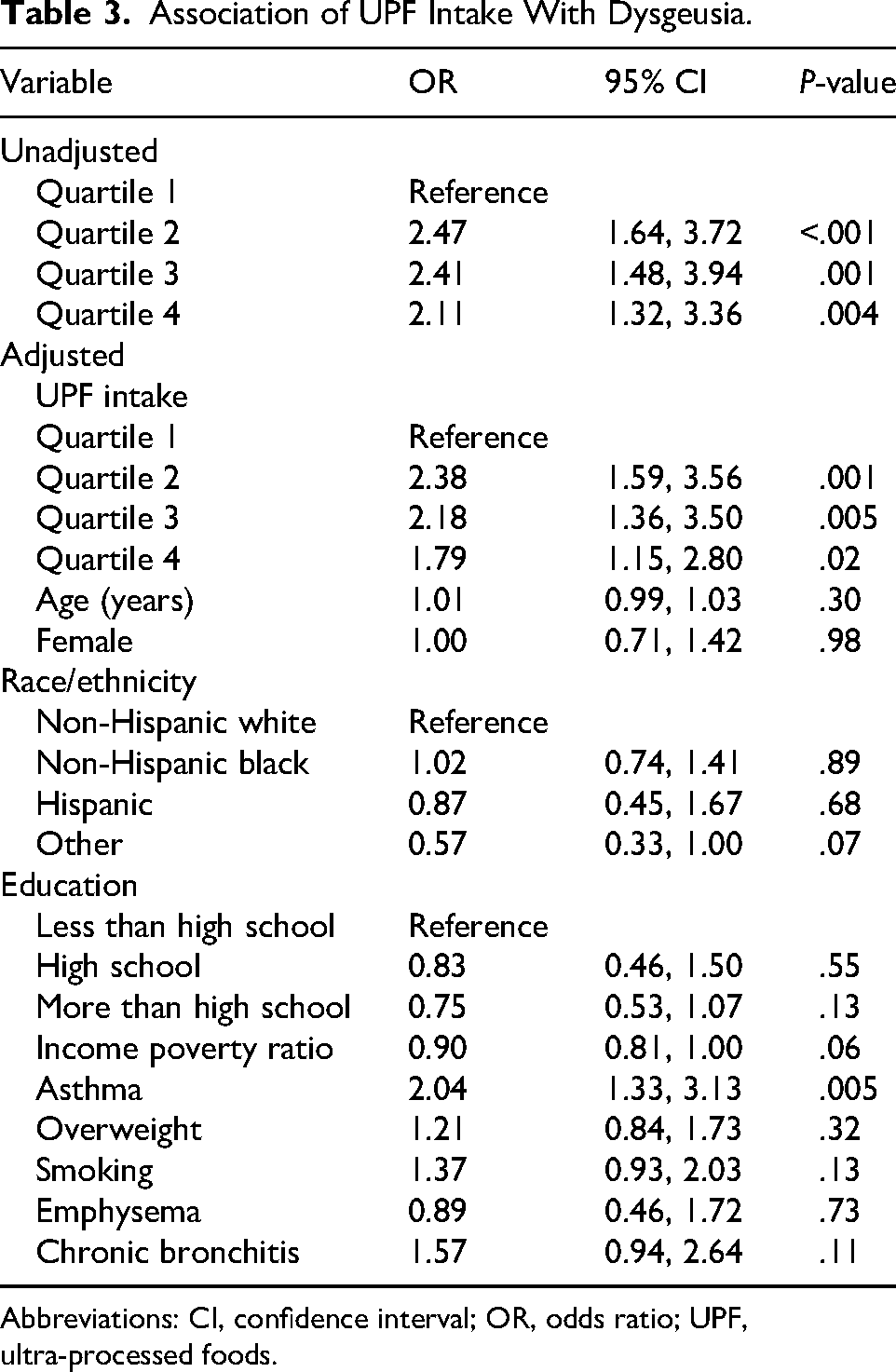
Abbreviations: CI, confidence interval; OR, odds ratio; UPF, ultra-processed foods.
Discussion
In this nationally representative sample, higher UPF intake was associated with a greater prevalence of self-reported sinusitis. The association was modest in magnitude but given the high prevalence of UPF in US diets, even small relative differences may carry meaningful population impact. Results were directionally consistent across model specifications and remained after accounting for key sociodemographic factors. Modeled as a continuous exposure, higher UPF intake showed a graded pattern of higher sinusitis prevalence, supporting a dose-response interpretation. Additionally because recall-based NOVA classification incurs nondifferential exposure misclassification, the results may be conservative.
In this study, the group with the highest quartile of UPF intake displayed higher rates of overweight status, asthma, and emphysema. These findings are consistent with prior literature linking UPF with respiratory morbidity and systemic inflammation, extending those observations to the sinonasal domain.2,5 No studies have focused on the link between UPF and emphysema, although evidence suggests that UPF intake increases risk for chronic respiratory tract diseases including chronic obstructive pulmonary disease.14,15 Participants in the highest quartile of UPF intake also had a higher propensity for food insecurity, consistent with findings in a prior large study employing NHANES. 16
The association of UPF intake with sinusitis has not previously been reported in the literature. However, a prior report suggests that the Mediterranean diet, which is low in UPF, can reduce the risk of RARS in the pediatric population. 11 The mechanism explaining the association of UPF with self-reported sinusitis remains unclear. In human domiciled controlled-feeding studies, diets high in UPF have been shown to alter CD4+ and CD8+ T-cell immune signatures. 4 This may explain how UPF can be associated with self-reported sinusitis, as cytokines produced by these T-cell populations are involved in sinusitis pathogenesis and define different chronic rhinosinusitis (CRS) endotypes.17-21 UPF also change the composition of the gut microbiome, 9 and recent reports have indicated a growing role for the biodiversity of the gut microbiota in CRS.9,22-24 Further studies are needed to better understand the mechanism underlying the association of UPF and sinusitis and to determine if UPF intake can serve as a modifiable risk factor for sinonasal disease.
Interestingly, despite its association with self-reported sinusitis, UPF intake was not linked with hyposmia, allergies, hay fever, and nasal congestion from allergies. A previous study has linked UPF consumption in children to allergic symptoms including asthma, rash, wheeze, eczema, and hay fever, and found a negative correlation between UPF intake and IgE levels. 6 However, these findings were not found in adults in the same study, consistent with our report showing no association between UPF and allergy, hay fever or serum total IgE levels in a predominantly adult population. Regarding hyposmia, a prior study suggests that individuals with poor diet quality may have a higher risk of subjective olfactory dysfunction, although UPF were not specifically investigated. 25 The previously discussed mechanisms for the UPF-induced sinusitis, including alterations in the microbiome and immune dysregulation, may be expected to trigger a pro-inflammatory state associated with allergy and other sinonasal symptoms. However, this immune dysregulation may also dampen the immune system, predisposing to infections such as sinusitis without promoting allergic symptoms. Alternatively, as the NHANES database does not differentiate between CRS, RARS, or isolated episodes of sinusitis, respondents may be reporting increased episodes of sinusitis without a change to baseline sinonasal symptoms between episodes. Future studies will need to include more rigorous diagnostic criteria to better evaluate the link between UPF and these symptoms.
The association of UPF intake and dysgeusia represents a novel and unexpected finding. One possible explanation involves the high level of preservatives and other artificial substances contained in UPF, which may contribute to xerostomia. In a previous study also utilizing NHANES, xerostomia was reported as the strongest risk factor for dysgeusia. 26 The association between UPF intake and dysgeusia was attenuated after adjusting for xerostomia, suggesting that xerostomia may explain part, but not all, of the observed relationship. Another possibility is that individuals with dysgeusia seek out UPF, which tend to be more flavorful than other foods. Conversely, individuals consuming flavorful UPF may perceive other unprocessed or minimally processed foods as less flavorful and subsequently report decreased ability to taste.
Our study has several limitations. Most notably, sinonasal symptom data were obtained based on respondent report, without objective measures including findings on physical exam, endoscopy, or imaging. Those reporting sinusitis may instead have experienced other conditions with similar symptoms, such as allergic rhinitis. Even for patients with sinusitis, it remains unclear if they have CRS, RARS, or an isolated episode, as previously mentioned, limiting interpretation of our data. Secondly, although data were adjusted for demographic variables and medical comorbidities, confounding may not be eliminated. Similarly, dietary recall was subjectively reported. Although data were collected at 2 time points, with patients asked to recall the immediate 24 h before each interview, recall bias may still affect our results. Lastly, this cross-sectional analysis does not allow for analysis of the mechanism for the association of UPF intake with self-reported sinusitis and xerostomia-associated dysgeusia.
Taken together, these data raise the possibility that the diet quality, and more specifically UPF consumption, plays a role in sinonasal health and merits prospective evaluation. The findings highlight a plausible, common, and potentially modifiable exposure worth clinical and public health attention. Further studies are needed to elucidate the mechanism of this association and to explore whether UPF intake could serve as a modifiable risk factor for sinonasal health.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924251404161 - Supplemental material for Association Between Ultra-Processed Food Intake and Sinusitis
Supplemental material, sj-docx-1-ajr-10.1177_19458924251404161 for Association Between Ultra-Processed Food Intake and Sinusitis by Anthony Thai and Noel F. Ayoub in American Journal of Rhinology & Allergy
Footnotes
Ethical Approval
Ethical approval for this study was waived by the Stanford University School of Medicine Institutional Review Board because it was conducted using publicly available, de-identified data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.