
Abstract
Background
Dendritic cells (DCs) are antigen-presenting cells that play a critical role in airway diseases by initiating and regulating immune responses. DCs are classified into plasmacytoid DCs (pDCs) and conventional DCs (cDCs), with the cDC lineage further divided into cDC1 and cDC2 subsets. Each subset exhibits distinct functions in immune regulation and disease pathogenesis. Thus, analyzing DC subsets is crucial for understanding the pathogenesis of airway diseases with diverse endotypes.
Objective
Allergic rhinitis (AR) and chronic rhinosinusitis (CRS), further divided into eosinophilic CRS (ECRS) and non-eosinophilic CRS (NECRS), are typical upper airway diseases with diverse endotypes. AR and CRS often occur simultaneously, and their severity tends to increase when they are comorbid. To understand the endotypes of AR and CRS, we classified the presence or absence of AR and CRS, analyzed the changes in DC subsets in the nasal mucosa, and compared these results with clinical features.
Methods
Nasal polyp tissues and ethmoid mucosa were collected from 42 patients who underwent endoscopic sinus surgery. DC were analyzed by flow cytometry to detect the expression of blood DC antigen (BDCA)-1, BDCA-2, and BDCA-3.
Results
BDCA-3+ cDC levels were significantly reduced in patients with both AR and CRS, compared to those with AR alone or CRS alone. This reduction was especially prominent in patients with ECRS, polysensitization, and total serum IgE ≥ 200 IU/mL. BDCA-3+ cDC levels were also inversely correlated with preoperative computed tomography scores and serum eosinophil and immunoglobulin E levels.
Conclusion
BDCA-3+ cDC levels may be involved in mucosal immune regulation and are associated with increased disease burden in patients with comorbid AR and ECRS.
Plain Language Summary
Antigen-presenting cells called dendritic cells (DCs) are essential in conditions affecting the airways. These DC are separated into various subsets, each of which may play a special role and develop into sizable immune cell populations that regulate the etiology of illness. These various DC subsets may have distinct roles and mature into important immune cell populations that control disease pathogenesis. As a result, studying DC subsets is essential to comprehending the pathophysiology of illnesses with various endotypes. Common upper airway diseases with a variety of endotypes are allergic rhinitis (AR) and chronic rhinosinusitis (CRS), which are further subdivided into eosinophilic CRS (ECRS) and non-eosinophilic CRS (NECRS). The severity of AR and CRS tends to increase when they co-exist, and they frequently happen at the same time. We categorized the presence or absence of AR and CRS, examined alterations in DC subsets in the nasal mucosa, and contrasted these findings with clinical characteristics in order to comprehend the endotypes of AR and CRS. 42 patients who had endoscopic sinus surgery had their nasal polyp tissues and ethmoid mucosa removed. Regardless of the presence of CRS, BDCA-1+ cDC and BDCA-2+ pDC levels were similar in subjects with AR. DC were examined using flow cytometry to identify the expression of blood DC antigen (BDCA)-1, BDCA-2, and BDCA-3. In comparison to patients without CRS, BDCA-3+ cDC levels were considerably lower in CRS patients and even lower in ECRS patients than in NECRS patients. Patients with CRS and comorbid AR exhibited reduced BDCA-3+ cDC levels, which were further decreased in those who were polysensitized. The mechanisms of severe inflammation in patients with AR and ECRS may be reflected in BDCA-3+ cDC levels, which may be crucial for immunoregulation.
Keywords
Introduction
Both chronic rhinosinusitis (CRS) and allergic rhinitis (AR), which are representative upper airway diseases, are inflammatory conditions of the sinus and nasal mucosa brought on by dysregulated immune responses.1,2 AR is characterized by chronic allergic airway inflammation, mainly pathogenic T-helper 2 immune responses, and increased production of allergen-specific immunoglobulin E (IgE).1,3 According to the European Community Respiratory Health Survey, approximately 7.0% to 47.5% of people worldwide suffer from AR, with regional variations in prevalence. 4
CRS is divided into CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP). 5 In contrast to non-eosinophilic CRS (NECRS), eosinophilic CRS (ECRS) is characterized by eosinophilic inflammation with type 2 cytokines.5,6 ECRS is clinically significant because it has high recurrence rate despite treatment and is strongly associated with AR or asthma, with the coexistence of AR and CRS potentially accelerating the progression of both diseases. 7 CRS affects 12.3%, 10.9%, and 13% of individuals in the USA, Europe, and China, respectively. 8
As a type of immune cell, dendritic cells (DCs) capture antigens and present them to T cells to promote their activation. DCs play a crucial role in the differentiation of Th cells into Th1, Th2, Th17, or regulatory T cells (Tregs) and modulate the balance between immune activation and tolerance.9,10 DCs can be divided into 3 main groups: conventional DCs (cDCs), plasmacytoid DCs (pDCs), and monocyte-derived DCs. cDCs were further divided into types 1 and 2 (Conventional type 1 and 2 DCs: cDC1 and cDC2, respectively). In the human airway, cDC1 expresses the blood DC antigen BDCA-3 (CD141), and cDC2 expresses BDCA-1 (CD1c), while pDCs express BDCA-2 (CD303).11,12 When nasal biopsy cells from allergy sufferers are exposed to allergens, transcriptional changes in CD1c+/CD1a+ cDC2 occur in the direction of the pro-allergic signaling pathways. In contrast, cDC2 expresses inhibitory/tolerogenic transcripts in nonallergic individuals. 13 Increased numbers of BDCA-3+ DCs were detected in the bronchoalveolar lavage fluid of patients with allergic asthma/rhinitis. 14 Moreover, pDC, cDC1, and cDC2 counts are significantly increased in nasal polyps, and an imbalance in the cDC/pDC ratio is a characteristic feature of nasal polyps. 15 These findings suggest that imbalances in DC subsets are linked to the severity of AR and CRS13,14,16–20; however, previous studies focused on changes and functions of DC subsets under standalone AR and CRS conditions. It is essential to consider that AR and CRS may influence each other, and potentially increase their severity if they develop as comorbid conditions. Therefore, in this study, we evaluated the distribution of DC subsets (BDCA-1+, BDCA-2+, BDCA-3+) in the nasal mucosa of patients with AR, CRS, and comorbid AR and CRS. Rather than focusing on functional roles of specific DCs, as done in most previous studies, we aimed to correlate DC subset distribution with clinical features, including eosinophilic inflammation, allergen sensitization, and radiologic severity, to better understand the immunologic endotypes associated with disease severity.
Materials and Methods
Subjects
We included 42 patients who underwent septoplasty or endoscopic sinus surgery, classified as normal, AR, or CRS. AR was diagnosed based on nasal symptoms and positive serological allergy tests, including a grade ≥2 result on a multiple allergen simultaneous test (MAST; AdvanSure™ AlloScreen, LG Life Sciences, Seoul, Korea), 21 a grade ≥1 result on the ImmunoCAP test (Thermo Fisher Scientific, Uppsala, Sweden), or a grade ≥2 result on a skin prick test (Bencard Allergie, Munich, Germany), based on standard clinical interpretations validated in previous studies.22–24 All participants underwent at least one type of allergy test (MAST, Skin Prick Test, or ImmunoCAP), and total serum IgE was measured in all patients. CRS was diagnosed using the criteria defined by the American Academy of Otolaryngology-Head and Neck Surgery Chronic Rhinosinusitis Task Force. 25 Subjects were included if they had a diagnosis of AR or CRS based on clinical history and objective findings. Patients with known immunodeficiency, pregnancy, coagulation disorders, or sinonasal tumors were excluded from the study. CRS was further divided into ECRS and non-ECRS based on a JESREC score of ≥11, 26 serving as a surrogate for type II inflammation. Olfactory function was assessed using the Korean version of the sniff test (KVSS) with the following scoring system: anosmia, ≤5; hyposmia, 6 to 21; and normal, ≥22. 27 Preoperative computed tomography (CT) was performed with 2 to 3 mm slice thickness within 1 month before surgery. The Lund-Mackay scoring system was applied bilaterally, with total scores ranging from 0 to 24. All scans were independently evaluated by 2 otolaryngologists blinded to clinical information. Symptom burden and disease-specific quality of life were assessed using a Sino-Nasal Outcome Test (SNOT-22). The total SNOT-22 score was used for analysis. The study protocol was approved by our institutional review board (4-2016-1153) and adhered to the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants for this study.
Tissue Preparation and Flow-Cytometric Analysis
In non-CRS and CRSsNP patients, the middle turbinate mucosa was obtained during partial middle turbinectomy performed to treat concha bullosa. In cases without concha bullosa, ethmoid mucosa was collected from the uncinate process using standard cold instruments. In CRSwNP patients, nasal polyp tissue was harvested. For each patient, a single mucosal sample was collected from one side of the nasal cavity. Samples were immediately placed in cold sterile phosphate-buffered saline and transported on ice, followed by flow cytometry processing within 4 h of collection (Supplementary Figure 1).
Harvested samples were fragmented and incubated with 30 mg/mL DNase I (Sigma-Aldrich, St. Louis, MO, USA) and 1 mg/mL collagenase D (Worthington Biochemical Corp., Lakewood, NJ, USA) at 37°C for 2 h. Cells were filtered, treated with lysis solution (Sigma-Aldrich), and stained for flow cytometric analysis.
Fc Block (anti-CD16/32; eBioscience, San Diego, CA, USA) was used to block single-cell suspensions for 30 min at 4°C. Following this, the cells were stained with live/dead (BV510; eBioscience), fluorochrome-conjugated anti-CD3/CD20/CD66b/CD335 (FITC; BD Biosciences, San Jose, CA, USA), anti-BDCA-1 (PerCP-Cy5.5; eBioscience), anti-BDCA-2 (PE; eBioscience), anti-BDCA-3 (APC; eBioscience), anti-CD14 (PE-Cy7; BioLegend, San Diego, CA, USA), anti-HLA-DR (APC-Cy7; eBioscience), anti-CD45 (BV421; eBioscience), and anti-CD11c (BV650; eBioscience) antibodies at 4°C for 30 min. Cells stained with appropriate isotype-matched antibodies were used as negative controls. The stained cells were analyzed using X-20 LSR Fortessa flow cytometer (BD Biosciences) and FlowJo software (Tree Star Inc., Ashland, OR, USA). To identify DC populations, we performed positive selection for leukocytes using CD45, and negative selection to exclude lineage markers, including CD3 (T cells), CD20 (B cells), CD66b (neutrophils and eosinophils), CD335 (natural killer cells), and CD14 (macrophages). DCs were identified within HLA-DR+ cells based on BDCA-1, BDCA-2, and BDCA-3 expression levels, indicating clustering into BDCA-1+ cDC, BDCA-2+ pDC, and BDCA-3+ cDC enabled subsets (Figure 1).

Representative flow cytometry plots for DC subsets in the nasal mucosa. The populations of DCs were examined using surface markers, including BDCA-1 and BDCA-3 for cDCs, and BDCA-2 for pDCs. Abbreviations: DCs, dendritic cells; BDCA, blood DC antigen; cDCs, conventional DCs; pDCs, plasmacytoid DCs.
Statistical Analysis
Statistical analyses were performed using GraphPad Prism (v.8.0.1; GraphPad Software, San Diego, CA, USA). For normally distributed variables, data are presented as mean ± standard error of the mean (SEM). The unpaired t-test with Welch's correction and Spearman's rank correlation coefficient were used for correlation analyses. Statistical significance was set at P < 0.05.
Results
Subjects
A total of 42 patients were classified into 4 groups: normal, AR, CRS, and comorbid AR and CRS. Five individuals without AR or CRS were included as healthy controls. Detailed characteristics of all participants are summarized in Table 1.
Clinical Characteristics of Subjects.
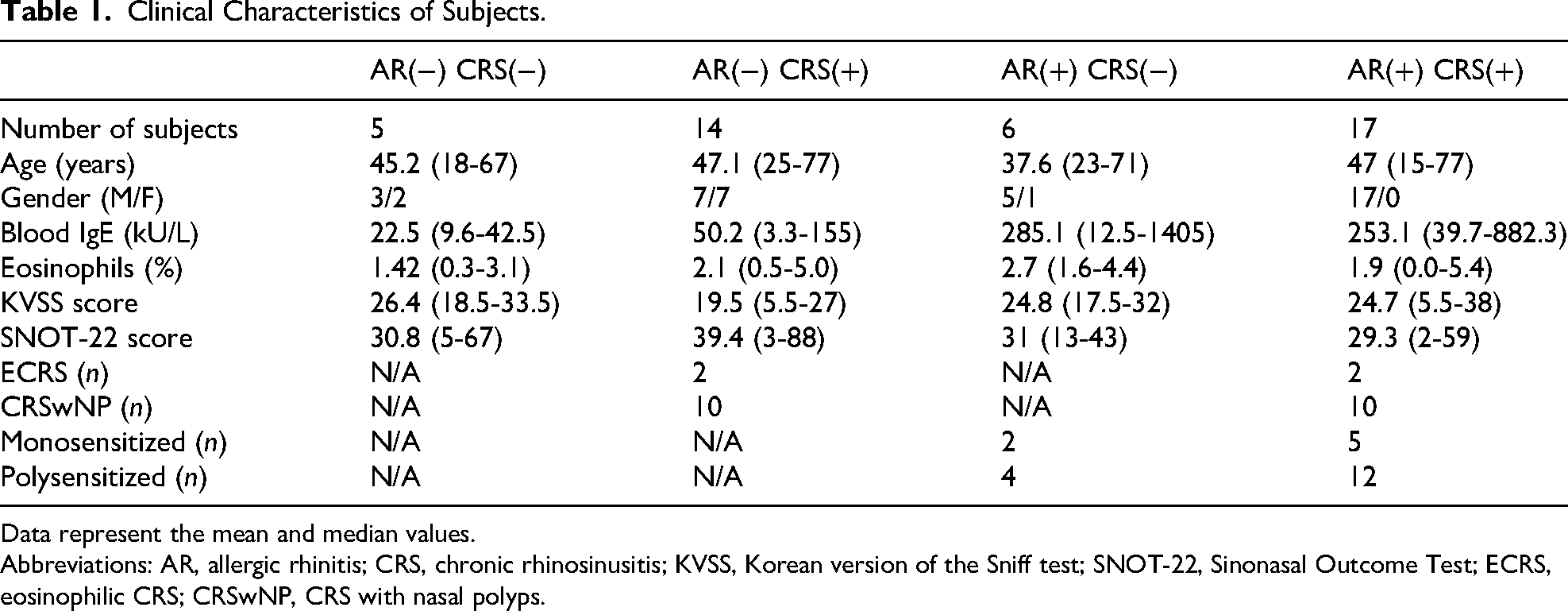
Data represent the mean and median values.
Abbreviations: AR, allergic rhinitis; CRS, chronic rhinosinusitis; KVSS, Korean version of the Sniff test; SNOT-22, Sinonasal Outcome Test; ECRS, eosinophilic CRS; CRSwNP, CRS with nasal polyps.
Reduced BDCA-3+ cDC Levels in AR Patients with Comorbid CRS, Particularly ECRS, and Their Correlation with Disease Severity
Flow cytometric analysis revealed that BDCA-1+ cDCs, BDCA-2+ pDCs, and BDCA-3+ cDCs were higher in patients with AR or CRS than in healthy controls (Supplementary Figure 2). To assess the correlation between comorbid CRS and nasal DC subsets in patients with AR, we analyzed changes in nasal DC subsets in patients with AR based on the presence or absence of CRS. In AR patients, BDCA-1+ cDC and BDCA-2+ pDC percentages were comparable between patients with and without CRS, with no significant differences observed between ECRS and NECRS patients. However, BDCA-3+ cDC levels tended to decrease when comorbid with CRS compared to AR alone. Interestingly, in AR patients with CRS, BDCA-3+ cDC reduction was greater in ECRS than NECRS (Figure 2A).
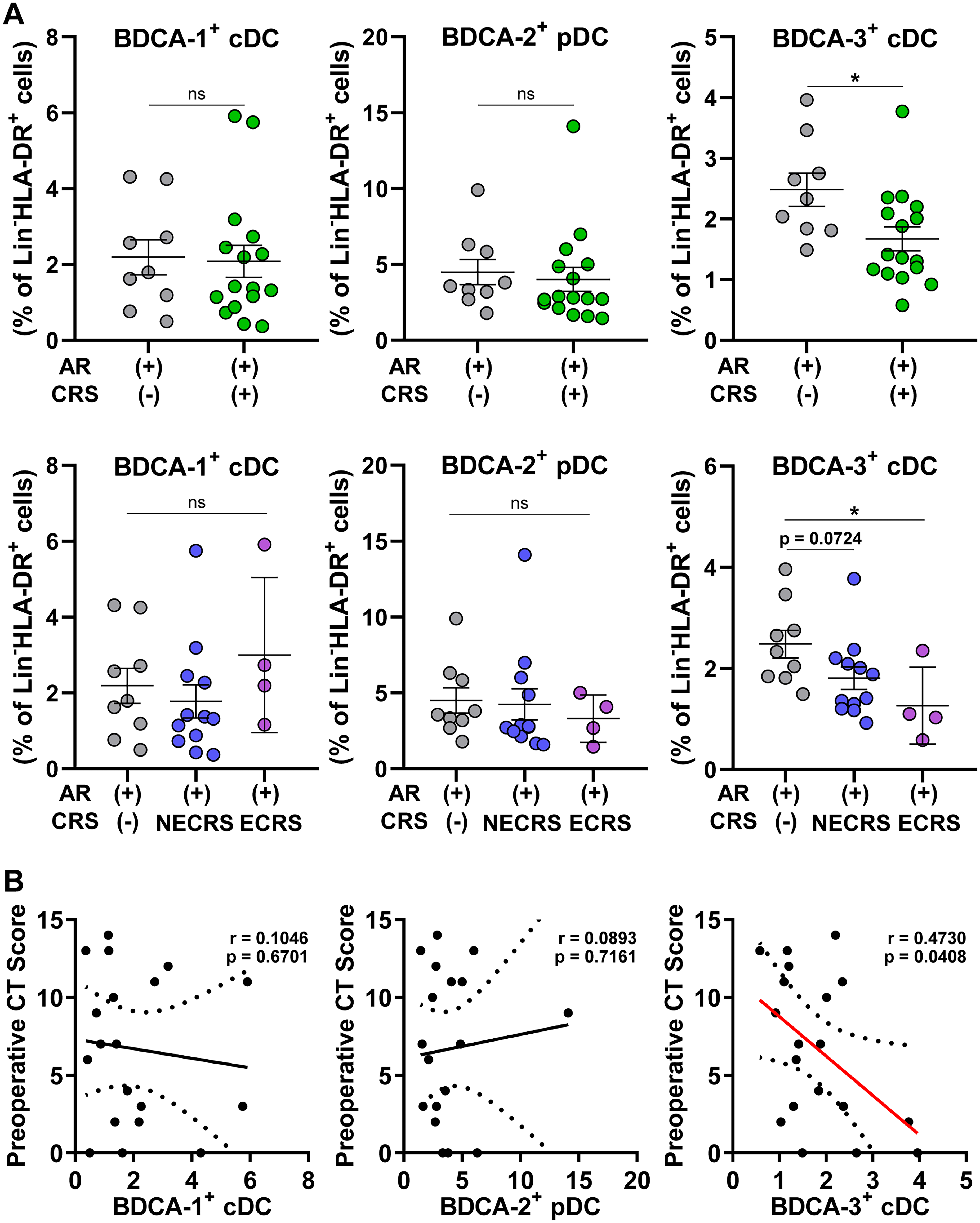
Analysis of DC subsets by CRS presence, CRS subtype, and CT score in AR patients. (A) Populations of BDCA-1+ cDCs, BDCA-2+ pDCs, and BDCA-3+ cDCs in AR patients, categorized by the presence of concomitant CRS, with further subdivision into ECRS and NECRS. (B) The correlation between each DC subset and the preoperative Lund-Mackay CT score. Data are presented as mean ± SEM. *P < 0.05, **P < 0.01; Welch's t-test. Abbreviations: DCs, dendritic cells; CRS, chronic rhinosinusitis; CT, computed tomography; AR, allergic rhinitis; BDCA, blood DC antigen; cDCs, conventional DCs; pDCs, plasmacytoid DCs; ECRS, eosinophilic CRS; NECRS, non-eosinophilic CRS; SEM, standard error of the mean.
We next analyzed the preoperative Lund-Mackay CT scores in patients with AR to determine whether sinus opacification and ostiomeatal complex obstruction, which are symptoms of CRS, correlate with DC subset levels (Figure 2B). The BDCA-1+ cDC and BDCA-2+ pDC populations showed no significant correlation with CT scores; however, BDCA-3+ cDC levels were inversely correlated with preoperative CT scores (Figure 2B). No correlation was found between JESREC score, which is related to CRS classification and endotypes, and nasal DC subsets in patients with AR. Similarly, no correlation was found between nasal DC subsets and SNOT-22 scores, reflecting sinonasal symptoms in patients with AR (Supplementary Figure 3).
These results suggest that in patients with AR, CRS occurrence, particularly ECRS, may be associated with reduced nasal BDCA-3+ cDC levels (Figure 2A). When BDCA-3+ cDC levels decrease in patients with AR, CRS symptoms may appear more severe (Figure 2B), suggesting that reduced nasal BDCA-3+ cDC levels in patients with AR may serve as an indicator of increased CRS risk.
BDCA-3+ cDC Reduction in CRSwNP Patients with Comorbid AR and Polysensitization
As observed in patients with AR, BDCA-1+ cDC, BDCA-2+ pDC, and BDCA-3+ cDC levels were increased in the nasal tissues of patients with CRS compared to healthy controls (Supplementary Figure 2). To assess the correlation between nasal DC subsets and AR risk in patients with CRSwNP, we examined the nasal DC subsets in patients with CRSwNP based on the presence of AR and the number of allergens sensitized (Figure 3). Flow cytometric analysis revealed a significant decrease in the BDCA-3+ cDC population in patients with AR, with no differences in BDCA-1+ cDC and BDCA-2+ pDC levels based on AR occurrence in patients with CRSwNP (Figure 3).
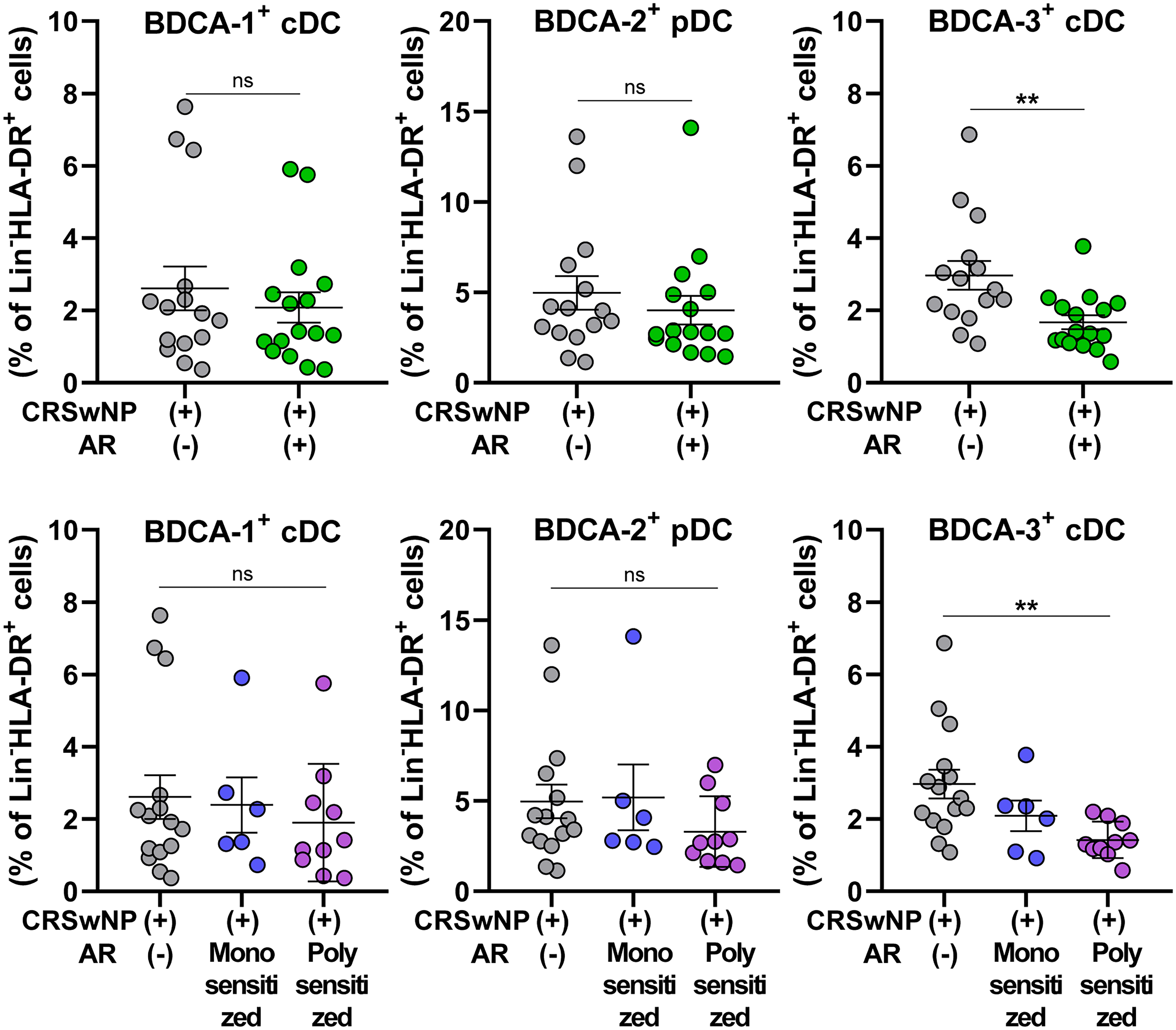
Analysis of DC subsets in CRSwNP patients according to the presence of AR and the number of allergens sensitized. Populations of BDCA-1+ cDCs, BDCA-2+ pDCs, and BDCA-3+ cDCs in CRSwNP patients, categorized by the presence of concomitant AR and further analyzed by allergen sensitization. Data are presented as mean ± SEM. *P < 0.05, **P < 0.01; Welch's t-test. Abbreviations: DCs, dendritic cells; CRSwNP, chronic rhinosinusitis with nasal polyps; AR, allergic rhinitis; BDCA, blood DC antigen; cDCs, conventional DCs; pDCs, plasmacytoid DCs; SEM, standard error of the mean.
We further analyzed allergen sensitization profiles and found that BDCA-3+ cDC reduction was observed only in CRSwNP patients with polysensitization (Figure 3). Based on these findings, immune responses mediated by nasal BDCA-3+ cDCs likely play a key role in the pathophysiology and outcomes of allergic reactions in patients with CRS.
Inverse Correlations Between BDCA-3+ cDC Levels and Serum Eosinophils, IgE, and Disease Severity Indices
To investigate the association of serological data and clinical parameters with DC subsets, we analyzed DC subsets of all enrolled patients. The BDCA-1+ cDC and BDCA-2+ pDC populations were comparable, regardless of total IgE levels by MAST; however, BDCA-3+ cDC populations tended to decrease with increasing total IgE levels (Figure 4A). Additionally, BDCA-3+ cDC populations were inversely correlated with blood eosinophil counts, whereas the BDCA-1+ cDC and BDCA-2+ pDC populations showed no correlation (Figure 4B).
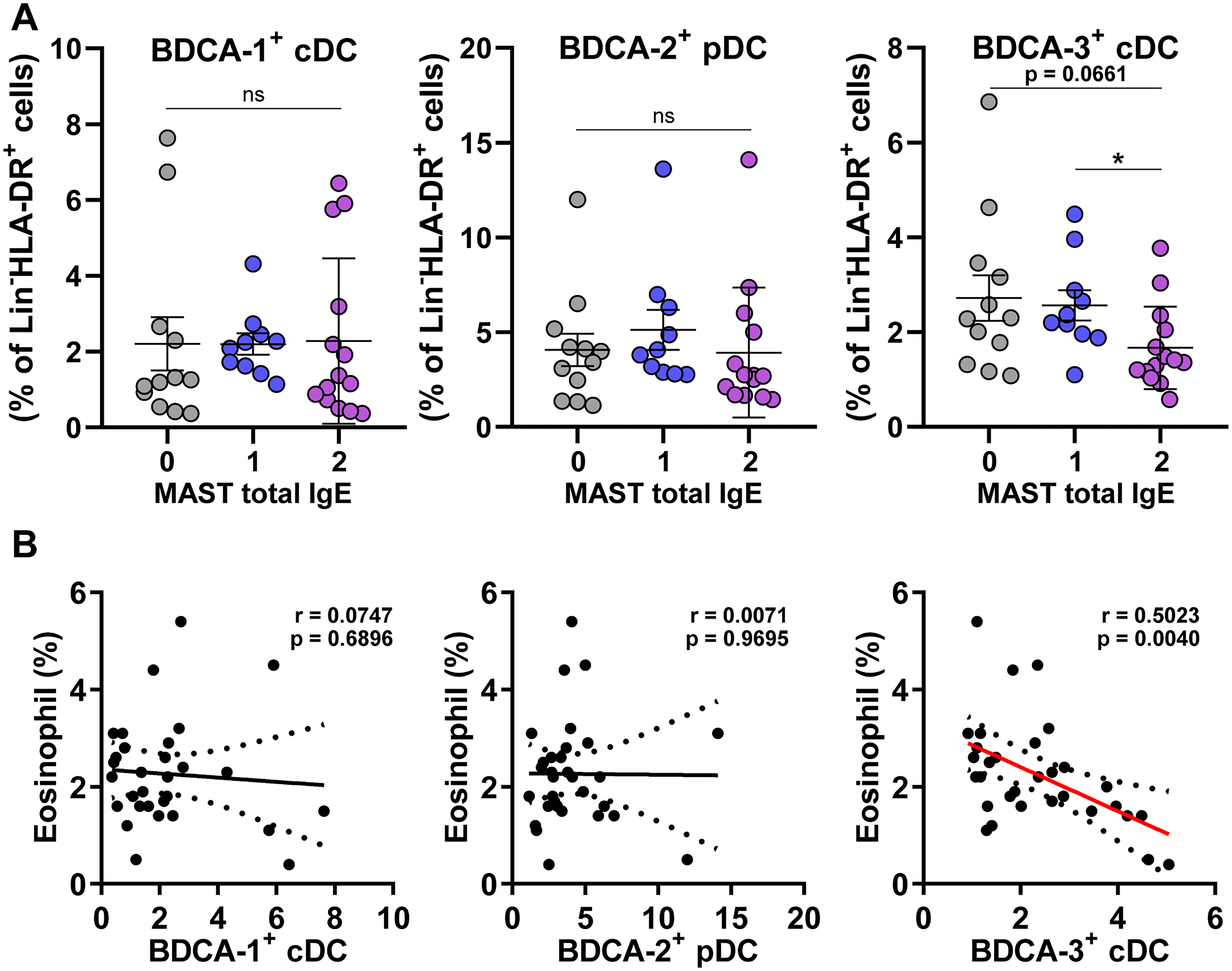
Analysis of DC subsets in the nasal mucosa according to total IgE and eosinophil levels. (A) Populations of BDCA-1+ cDCs, BDCA-2+ pDCs, and BDCA-3+ cDCs in patients according to total serum IgE levels. MAST Total IgE grade: 0: ≤100 IU/mL, 1+: 100 to 200 IU/mL, 2+: ≥200 IU/mL. (B) Correlation between each DC subset and blood eosinophil levels. Data are presented as mean ± SEM. *P < 0.05, **P < 0.01; Welch's t-test. Abbreviations: DCs, dendritic cells; BDCA, blood DC antigen; cDCs, conventional DCs; pDCs, plasmacytoid DCs; MAST, multiple allergen simultaneous test; IgE, immunoglobulin E; SEM, standard error of the mean.
In analyses based on CRS and the presence of nasal polyp, BDCA-2+ pDCs were most increased in the CRSwNP group, whereas BDCA-1+ cDC and BDCA-3+ cDC populations showed no significant differences between groups (Supplementary Figure 4A). Regarding CRS recurrence, no significant difference was observed in DC subset populations among non-CRS, primary CRS, and recurrent CRS patients (Supplementary Figure 4B). Analysis of correlations between KVSS scores and DC subsets revealed an inverse correlation between BDCA-1+ cDCs and KVSS scores, with no correlation in the BDCA-2+ pDC or BDCA-3+ cDC populations (Supplementary Figure 4C).
Overall, these results confirmed that nasal BDCA-3+ cDCs, in contrast to BDCA-1+ cDCs and BDCA-2+ pDCs, reduced AR and CRS comorbidity compared to each disease individually. Furthermore, BDCA-3+ cDC levels were inversely correlated with preoperative CT scores, serum eosinophil levels, and IgE levels.
Discussion
An important finding of this study is the significant reduction of BDCA-3+ cDCs in patients with comorbid AR and CRS, particularly in ECRS, compared to AR or CRS alone. This suggests that BDCA-3+ cDCs may serve as potential biomarkers for disease severity and progression. Reduced BDCA-3+ cDC levels in comorbid conditions may reflect a failure in maintaining immunological tolerance, leading to exacerbated inflammatory responses. Previous studies have suggested that BDCA-3+ cDCs play a critical role in cross-presentation of antigens and induction of tolerogenic immune responses via Treg activation.28,29 This is supported by our observation of a simultaneous decrease in CD4+ FoxP3+ Tregs in AR and CRS comorbid patients (data not shown). These findings imply a possible mechanistic link between BDCA-3+ cDC depletion and impaired regulatory pathways, which warrants further experimental studies.
A recent transcriptomic study of blood-derived BDCA-3+ DCs from patients with allergic asthma revealed altered gene expression profiles and potential differences in Th2 immune responsiveness compared to non-allergic individuals. 30 While these findings suggest a possible role for BDCA-3+ DCs in allergy-associated immune modulation, their functional relevance in airway-resident DCs remains unclear, highlighting the need for tissue-specific investigations.
In addition, the inverse correlation of BDCA-3+ cDC levels with preoperative CT scores, serum eosinophils, and IgE levels highlights the potential of BDCA-3+ cDCs as a clinical indicator. A previous Korean study reported that polysensitized CRS patients (eg, dust mite and pollen) had higher CT scores and total IgE levels than those with monosensitization. 31 This supports our current finding that BDCA-3+ cDCs were significantly reduced only in CRSwNP patients with polysensitized AR, suggesting a link between BDCA-3+ cDCs and the severity of allergic inflammation.
Considering the substantial comorbidity of CRS and AR with asthma and other allergic disorders, future studies should explore the broader implications of BDCA-3+ cDC dysregulation in systemic allergic and inflammatory diseases. Furthermore, our findings raise the question of whether therapeutic modulation of BDCA-3+ cDCs could ameliorate the severity of AR and CRS, particularly in patients with refractory or recurrent disease.
Compared to previous studies, this study offers significant research advantages. First, we examined the population of DC subsets in the nasal mucosa rather than in the blood. Several studies have used peripheral blood DCs, which do not fully reflect the immunological features of nasal DCs.32,33 During the pathogenesis of AR and CRS, nasal DCs are continuously exposed to numerous antigens and pathogens, triggering secondary immune responses in the nasal cavity that influence the endotypes. Therefore, comprehensive research on nasal DC subsets is essential to understand the pathogenesis of AR and CRS. Second, we used the ethmoid mucosa or middle turbinate tissue as disease-free controls and not the inferior turbinate tissue. Many studies have used inferior turbinate or even nasopharyngeal mucosa for their analyses12,20,34–36; however, these do not represent accurate physiological samples. The extracellular matrix composition in the submucosa of the inferior turbinate is different from that of the middle turbinate and sinus mucosa, whereas the cellular composition of polyp tissue is similar to that of the middle turbinate and sinus mucosa. Therefore, widespread use of the inferior turbinate as a control in CRS studies can lead to methodological errors and misinformation.37,38 Third, we investigated the population of BDCA-3+ cDCs in detail, whereas many previous studies on nasal DCs have only examined cDCs and pDCs as DC subsets.35,36,39 Most importantly, this is the first study to independently evaluate DC subsets under AR and CRS conditions. Previous studies on DC populations in patients with CRS included subjects regardless of AR presence, and DC populations in patients with AR were determined regardless of CRS history,20,34,35,39,40 which could result in a significant bias due to the interaction of AR with CRS.
This study had some limitations. First, quantitative changes in nasal DC subsets were examined only in relation to AR, CRS, and their indicators without confirming the immunological roles of nasal BDCA-3+ cDCs. Although we observed a simultaneous decrease in CD4+ FoxP3+ Tregs in patients with AR and CRS (data not shown), it remains unclear whether nasal BDCA-3+ cDCs can reduce Tregs via their tolerogenic effects. In addition to Tregs, other immune cell populations should also be considered as responders to BDCA-3+ cDCs. Therefore, further investigations are needed to understand how nasal BDCA-3+ cDCs regulate immune responses in AR and CRS and affect endotypes. Second, we observed that nasal BDCA-3+ cDCs increased in AR or CRS alone, but decreased when AR and CRS progressed to comorbid conditions. It is unclear what specific circumstances arising from AR and CRS comorbidities influence the levels and immunological characteristics of BDCA-3+ cDCs. Third, there is a lack of histological or immunohistochemical staining to localize DC subsets in nasal tissue. Future studies will incorporate tissue-level immunostaining to complement the phenotypic profiling achieved through flow cytometry. Finally, we did not consider the patients’ medication history before surgery. Some patients continued medications such as intranasal corticosteroids or oral antibiotics due to poorly controlled symptoms. These agents may influence the population of DC subsets; therefore, the present results may be complicated by these unknown factors. However, to our knowledge, this is the first study to examine Korean patients with AR and CRS, with a focus on comorbidities. CRS has been reported to have different phenotypes and endotypes in Europe, America, and Asia. 41 Therefore, this study serves as a cornerstone for understanding and treating patients with CRS and AR in Asia.
Conclusion
In summary, we found that the number of BDCA-3+ cDCs is lower in patients with AR and CRS comorbidity compared to those with a single disorder. Additionally, the levels of BDCA-3+ cDCs inversely correlated with preoperative CT scores and serum eosinophils and IgE levels. These findings suggest that BDCA-3+ cDCs may be involved in mucosal immune regulation and tolerance in upper airway inflammation. However, these conclusions should be interpreted with caution due to limitations such as variability in biopsy sites and a relatively small sample size. These findings contribute to understanding AR and CRS pathophysiology and provide insights for identifying novel anti-inflammatory therapies in upper airway diseases.
Supplemental Material
sj-tif-1-ajr-10.1177_19458924261416572 - Supplemental material for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis
Supplemental material, sj-tif-1-ajr-10.1177_19458924261416572 for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis by Dahee Shim, Tae-Gyun Kim, Yeeun Bak and Hyung-Ju Cho, Chang-Hoon Kim, Joo-Heon Yoon, Sang Chul Park in American Journal of Rhinology & Allergy
Supplemental Material
sj-tif-2-ajr-10.1177_19458924261416572 - Supplemental material for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis
Supplemental material, sj-tif-2-ajr-10.1177_19458924261416572 for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis by Dahee Shim, Tae-Gyun Kim, Yeeun Bak and Hyung-Ju Cho, Chang-Hoon Kim, Joo-Heon Yoon, Sang Chul Park in American Journal of Rhinology & Allergy
Supplemental Material
sj-tif-3-ajr-10.1177_19458924261416572 - Supplemental material for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis
Supplemental material, sj-tif-3-ajr-10.1177_19458924261416572 for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis by Dahee Shim, Tae-Gyun Kim, Yeeun Bak and Hyung-Ju Cho, Chang-Hoon Kim, Joo-Heon Yoon, Sang Chul Park in American Journal of Rhinology & Allergy
Supplemental Material
sj-tif-4-ajr-10.1177_19458924261416572 - Supplemental material for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis
Supplemental material, sj-tif-4-ajr-10.1177_19458924261416572 for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis by Dahee Shim, Tae-Gyun Kim, Yeeun Bak and Hyung-Ju Cho, Chang-Hoon Kim, Joo-Heon Yoon, Sang Chul Park in American Journal of Rhinology & Allergy
Supplemental Material
sj-docx-5-ajr-10.1177_19458924261416572 - Supplemental material for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis
Supplemental material, sj-docx-5-ajr-10.1177_19458924261416572 for Reduced Numbers of Blood Dendritic Cell Antigen 3 Positive Dendritic Cells in the Nasal Mucosa Contribute to Severe Inflammation in Patients with Allergic Rhinitis and Chronic Rhinosinusitis by Dahee Shim, Tae-Gyun Kim, Yeeun Bak and Hyung-Ju Cho, Chang-Hoon Kim, Joo-Heon Yoon, Sang Chul Park in American Journal of Rhinology & Allergy
Footnotes
Authors’ Note
Some preliminary results of this study were presented as a poster at the American Thoracic Society International Conference 2024 held in San Diego, USA, from May 17 to May 22, 2024.
Ethical Approval and Informed Consent Statements
This study was approved by the Yonsei University College of Medicine Research Ethics Committee (4-2016-1153), and all participants provided written informed consent prior to participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program of the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2020R1I1A3067369). This research was also supported by Hallym University Research Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.